Case Report
A 26-year-old male patient reported to out-patient department of Panineeya Dental College, Hyderabad, India with a chief complaint of swelling on the left side of the upper lip, close to midline. Patient first noticed the swelling about 10 years back, and swelling had exhibited a gradual increase in size, over the years. The swelling was painless, and patient had sought medical help, chiefly because of an aesthetic concern. The patient had an uneventful medical history, and there was no associated history of trauma. Also, patient did not have history of deleterious habits.
On clinical examination, a papule, measuring approximately 0.8*0.8 mm in size, with well-defined margins was seen on the left side of upper lip; overlying mucosa was of normal colour without ulcerations [Table/Fig-1].On palpation, the swelling was sessile, firm, and non-tender. The swelling was hypothesized to be a mucocele. Patient consented for a procedure of excisional biopsy with laser.
The swelling was excised under local anaesthesia [Table/Fig-2], using diode laser of specifications: 810nm wavelength, 400 microns diameter tip, and 0.8W power. Safety eyewear was used by clinician, assistant and the patient. The excised tissue was fixed in 10% formalin and sent for histopathological examination and immunohistochemistry.
Histopathology
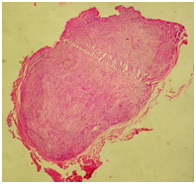
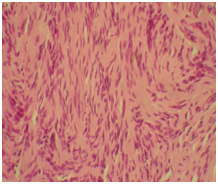
The tissue showed encapsulated connective tissue stroma [Table/Fig-3] consisting of spindle shaped cells. The nuclei were wavy and hyper chromatic and arranged as streaming fascicles separated by clefts at focal areas suggesting neural tissue [Table/Fig-4].
Immunohistochemistry
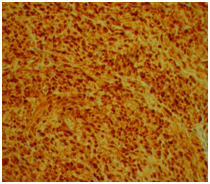
The bundles and fascicles of spindle shaped cells were strongly positive for S100 protein staining. This further confirmed their neural origin [Table/Fig-5]. Thus, a final diagnosis of solitary circumscribed neuroma was made.
The surgical procedure was uneventful, there was no bleeding. Resorbable sutures were placed [Table/Fig-6]; patient was prescribed postoperative symptomatic relief medication and topical antiseptics. Patient was followed up every week for one month, exhibited uneventful healing and thereafter was recalled at six months[Table/Fig-7] and one year after therapy[Table/Fig-8]. There was no recurrence, and patient was satisfied with his aesthetics.
Discussion
Neural tumours can occur in the soft tissues or hard tissues of the oral region, and often manifest as painless, smooth swelling in the soft tissues of the mouth [1]. Palisaded encapsulated neuroma (PEN) was defined by Reeds et al., [2]. Since palisading and encapsulation was not always seen, Fletcher [3] gave this lesion an alternate terminology solitary circumscribed neuroma (SCN).
PEN/SCN is a benign neural tumour which is well circumscribed [1,4] , firm, whitish gray, intradermal, pear shaped nodules [4], with a predilection for the face, in particular the nose, upper eye lid, cheek, chin and lips [1]. The lesion enlarges over several years [5] as has been the case with this patient too. Occasional cases are associated with telangiectasias [5].
The histopathology of this tumour is characterized by interlacing fascicles of spindle cells, the presence of the capsule [1].
The differential diagnosis of oral PEN/SCN includes other benign neurogenic tumours like schwannoma and neurofibroma [6].
PEN differs from schwanoma by a more superficial location, absence of Antoni type tissues, and presence of relatively more number of axons and myelin sheaths [1].
Strong S-100 protein staining within the cytoplasm of spindle cells is crucial in differentiating these lesions from Schwannomas and neurofibromas[1]. Lack of a lobular architecture, fibrosis and, absence of lipoblasts, differentiates PEN from fibrolipomas [7].
Palisaded encapsulated neuroma can be distinguished from neurofibromas in being capsulated and presence of broader fascicles with more axons and myelin sheath and also a lack of significant mucopolysaccaride ground substance and mast cells [1].
A provisional diagnosis of mucocele was made for this patient. Mucocele is a common lesion of the lip. Here, the patient had an asymptomatic swelling of normal mucosal colour, resembling a mucocele. Morever, mucocele being the most common lesion of the lip, second only to infections of the lip [8] and having multiple types of manifestation, would always be the clinician’s choice for a provisional diagnosis.
Histopathology had revealed encapsulation, which is also a feature of ganglioneuromas, but these tumours are not so common in the alimentary tract [9], also no ganglion cells were seen microscopically.
Neurofibromas also form a part of the differential diagnosis. These tumours are deep rooted, are not site specific and feature expansive growth. The microscopic pattern is cells arranged in short fascicles or whorls [9]. They are commonly found in patients with von Recklinghausen’s disease, and this patient did not exhibit any history or any other associated clinical features of this disease.
A diagnosis of traumatic neuroma was ruled out because the patient did not report a history of trauma [9], lesion was asymptomatic. Traumatic neuromas are commonly painful [10] and may present with burning sensation or pareasthesia [9]. Also, absence of inflammatory cells helps to distinguish this tumour from traumatic neuroma [1].
Strong S-100 staining is characteristic of solitary circumscribed neuroma (palisaded encapsulated neuroma) [6]. A negative Glial fibrillary acidic protein staining (GFAP) is confirmatory of PEN/SCN pathology [6] and would have added credibility to our diagnosis, as this would distinguish PEN/SCN from other benign neural tumours.
Treatment of choice for PEN/SCN is gross total excision [6]. Although surgical approach is the traditional method of management, of late; patients are very much aware about less invasive techniques and prefer the same. These techniques like cryosurgery, and laser therapy, are associated with haemostasis and thus, help in proper access, precision of excision, and also improved patient comfort.
Apart from the advantages of good patient comfort, haemostasis, better postoperative healing [7], and anti-bacterial effect than laser treatment provides, laser therapy definitely has an edge over the normal scalpel incision, while performing excisional biopsies, in terms of preserving the tissue for histopathological examination, as the procedure is less invasive and more conservative. The diode laser used to manage the neuroma in this case, is ideal for soft tissue excisions [11].
Laser therapy thus indirectly helps us to achieve the correct diagnosis, as it allows for adequate histological examination [7]. Although laser therapy obviates the need for sutures, the surgical site was approximated with resorbable sutures, so as to achieve better closure of the wound, since the patients chief concern was aesthetics.
PEN, has a low chance of recurrence after treatment. Here, this patient also did not have recurrence of swelling one year post-treatment. Patients can be reassured that excision is curative, with less chance of recurrence, and there is no indication for further investigations for malignancy [5].
Any pathology of the lip can have a wide array of differential diagnosis as the lip contains adipose tissue, connective tissue, vasculature, nerves and salivary glands [12]. Also, many lip lesions are asymptomatic, and correct diagnosis plays a decisive factor in treatment. Since the occurrence of benign and malignant tumours in this region is very common, proper and timely diagnosis is vital and prompt management, namely excisional biopsy is definitely warranted for lip lesions [12].
Pre-operative appearance of swelling

Intraoperative – Excision

Immun ohistochemistry 10x
Intra-operative picture-Resorbable sutures

Postoperative photograph- 6 months

Postoperative photograph-1 year

Conclusion
Oral PEN/SCN, although a common mucocutaneous peripheral nerve sheath lesion to the best of authors knowledge does not seem to have as many cases documented. This raises the question of whether the tumour is rare or very commonly misdiagnosed or underdiagnosed, as they are asymptomatic.
The inference is that with lesions of the lip, histopathology holds key to correct diagnosis. Moreover, the knowledge of the clinician is instrumental in arriving at a good range of differential diagnosis to investigate and confirm final diagnosis and management.
[1]. B Maharudrappa, GS Kumar, Neural Tumours of Oral and Para Oral RegionInt J dent Clin. 2011 3(1):34-43. [Google Scholar]
[2]. R Reed, R Fine, H Meltzer, Palisaded encapsulated neuromas of the skinArch Dermatol 1972 106(6):865-70. [Google Scholar]
[3]. CD Fletcher, Solitary circumscribed neuroma of the skin (so-called palisaded, encapsulated neuroma). A clinicopathologic and immunohistochemical study.Am J Surg Pathol 1989 13(7):574-80. [Google Scholar]
[4]. A Samdurkar, S Poudel, S Regmi, S Khurana, Palisaded Encapsulated Neuroma (PEN): A Case Report.J Univers Coll Med Sci 2013 1(1):28-32. [Google Scholar]
[5]. MD Newman, S Milgraum, Palisaded encapsulated neuroma (PEN): an often misdiagnosed neural tumour.Dermatol Online J. 2008 14(7):12 [Google Scholar]
[6]. IG Koutlas, BW Scheithauer, Palisaded encapsulated ("solitary circumscribed") neuroma of the oral cavity: a review of 55 casesHead Neck Pathol 2010 4(1):15-26. [Google Scholar]
[7]. S Capodiferro, E Maiorano, AM Loiudice, F Scarpelli, G Favia, Fibrolipoma of the lip treated by diode laser surgery: A case report.J Med Case Reports 2008 2(301) [Google Scholar]
[8]. S Patil, S Maheshwari, Prevalence of lip lesions in an Indian populationJ Clin Exp Dent. 2014 6:e374-78. [Google Scholar]
[9]. MA Lopes, PA Vargas, OP Almida, A Takahama, JE Leon, Oral traumatic neuroma with mature ganglion cells: A case report and review of the literatureJ Oral Maxillofac Pathol 2009 13:67-69. [Google Scholar]
[10]. AL Anbinder, TV Paiva, RC Mariano, MR Quirino, MR.Traumatic neuroma of the lower lip.West Indian Med J. 2009 58(6):604-06. [Google Scholar]
[11]. G Agarwal, A Mehra, A Agarwal, Laser vaporization of extravasation type of mucocele of the lower lip with 940nm diode laserIndian J Dent Res 2013 24(278) [Google Scholar]
[12]. IZ Mustapha, Jr Boucree SA, Mucocele of the upper lip: case report of an uncommon presentation and its differential diagnosisJ Can Dent Assoc 2004 70(5):318-21. [Google Scholar]