Introduction
Hepatic and hepatobiliary diseases are a common cause of morbidity and mortality in children. The term chronic liver disease (CLD) implies a long standing irreversible change in the hepatic structure that may end in complications like cirrhosis leading to premature death. Previously 6 months duration of symptoms was required for making a diagnosis of autoimmune hepatitis. This concept has been recently abandoned [1]. Every case with CLD warrants a complete clinical assessment and thorough biochemical and serological testing including histopathological evaluation of liver biopsy in order to reach a conclusive diagnosis [2].
Specimens of liver tissue can be used to provide precise histology diagnosis, for enzyme analysis to detect inborn errors of metabolism, for analysis of stored material such as iron, copper, to monitor response to therapy & to detect complications of treatment with potentially hepatotoxic drugs [3].
The essential advantages of histopathological study of liver biopsy being, to arrive at exact diagnosis, in metabolic disorders, to gauge the severity of insult; for instance chronic active hepatitis denotes a more severe degree of damage than does chronic persistent hepatitis [4]. To exclude other differential diagnosis, prognosis and follow up of certain diseases like Wilson’s disease. To assist the effects/improvements with treatment, liver biopsy is the choice of investigation.
Liver biopsy is performed through two approaches one is percutaneous, second is transjugular in case of grossly deranged liver function to avoid danger of bleeding. Three types of needles, Menghini’s, Tru-Cut liver biopsy & Vim Silverman needle are used [5].
Aims and Objectives
The aim was to study the clinical profile of disorders of the liver and hepatobiliary system in paediatric patients (1 to 12 years), to evaluate the findings in various liver and hepatobiliary diseases on liver biopsy and to correlate the histopathology findings of liver biopsy with the possible clinical presentations in CLD. Also, to assess the prognosis of CLD proven by biopsy and to know the outcome and the effects of treatment in chronic liver diseases in paediatric age group.
Materials and Methods
This was a prospective study carried in a large teaching hospital. Fifty five children in paediatric age group who presented with CLD comprised the study group. The total duration of study was 28 months. (Feb. 2002 to May’04). The parent’s informed consent was taken after explaining the purpose of the study. The study included the clinical profile of CLD in children and the histopathological correlation. First, the detailed history of the presenting complaints of all the patients was noted in a predesigned proforma.
Biochemical and hematological investigations: CBC, Liver function tests included serum bilirubin levels, liver enzymes, serum proteins (total proteins and serum albumin), prothrombin time (PT) and prothrombin index (PI). Bleeding time (BT) and clotting time (CT), renal function tests were done. In case of suspicion of hepatic encephalopathy, blood ammonia was done.
Serology for viral markers and for special investigations: Other serological investigations like HBsAg, Igm HAV, Igm HEV, anti HCV antibody were done wherever necessary. Protein electrophoresis for α1-Antitrypsin deficiency, α-fetoprotein level, ANA, dsDNA, VDRL, ELISA for HIV. Protein C/S/ AT-III levels were done. TORCH titers done in a case of suspected IU infection. Tests like serum ceruloplasmin levels, 24 hour urinary copper value including pre penicillamine and post penicillamine. Slit lamp examination of eyes for KF ring, MRI brain for copper deposition in basal ganglia and liver biopsy and dry weight of copper in liver tissue was done using atomic absorption spectrometry in patients suspected to have Wilson’s disease. Patients suspected to have autoimmune hepatitis were worked up for the same with antinuclear anti body (ANA), antismooth muscle antibody (ASMA), protein electrophoresis for gammaglobulin levels and anti liver, kidney, microsomal (Anti LKM) antibody levels.
Radiological investigations: X-ray chest and lower limbs (IU infection), USG abdomen, USG Doppler & liver scan were done wherever necessary. CT abdomen, CT spleenoportogram, CT cholangiogram was done. In certain cases, CT brain to confirm intracranial calcification and MRI in case of Wilson’s disease for basal ganglia & MRCP to see obstructive pathology in the hepatobiliary tract was done.
Liver Biopsy: The procedure was done only in patients having normal PT and PI or normal platelet count and normal BT, CT. Procedure was done under USG guidance in difficult cases and with all aseptic precautions by an expert paediatricians using Tru-cut liver biopsy needle. An expert pathologist was identified for the study of these biopsy pieces. Treatment on patients was initiated depending on the clinical diagnosis and histopathology. Follow up of the patients included clinical as well as biochemical monitoring.
Specialty opinion: From gastroenterology, paediatric surgery, ophthalmology was done wherever necessary. Liver Biopsy usually undertaken for assessment of Liver parenchymal dysfunction, Cholestatic jaundice, Portal hypertension and Hepatomegaly [6].
Observations and Results
We had total 55 children with CLD. Male predominance (60%) was noted. Incidence of CLD was maximum in the age group of 6-12 years. [Table/Fig-1] highlights the comparison of clinical manifestations of patients in our study with other studies [7-9]. Wilson’s disease work up done in some patients on clinical suspicion with findings mentioned in above [Table/Fig-2]. This [Table/Fig-3] shows the comparison of our study with other studies [10,11] with respect to clinical features, laboratory features, serology, histopathology and outcome in patients with autoimmune hepatitis. Metabolic work up other than Wilson’s disease showed abnormal results like lipid profile/blood sugar/iron studies in few patients as denoted in [Table/Fig-4]. Liver biopsy demonstrated various histopathological abnormalities like inflammation, ballooning of hepatocytes, cholestasis, necrosis, fibrosis, cirrhosis etc as shown in [Table/Fig-5]. The most common group of liver disease in this study was metabolic liver disease. In these 18, Wilson’s disease accounted 12 patients (66.66%), GSD, α1-Antitrypsin deficiency and NLSD in 2 patients each (11.11%) as denoted in [Table/Fig-6]. The [Table/Fig-7] shows the spectrum of chronic liver disease in our study.
Discussion
A very high index of suspicion is required for diagnosis of CLD as only 1.1% of total admissions (55 out of 5146) were patients of CLD. Clinical manifestations of patients in our study were compared with other studies i.e. Qureshi, Malik and Mehnaz et al., as values denoted in [Table/Fig-1]. The most common presenting complaint as noted by us was jaundice, followed by hepatosplenomegaly and abdominal distension. There are a few patients of CLD who did not present with jaundice, 25% of the children did not have jaundice in a study conducted at AIIMS [12]. Jaundice along with abdominal distension indicates advanced disease and is associated with poor outcome [13]. Ascites also features as one of the poor prognostic indicator in liver disease as cited by Child’s grading of cirrhosis [13].
Hepatic encephalopathy was noted in 16 patients (29%). The staging of hepatic encephalopathy was according to level of consciousness, personality, intellect and neurological signs [14]. Five patients had involvement of kidneys, 3 had hepatorenal syndrome and one had lupus nephritis with acute renal failure. Similar observations were made by Yuce et al., [15]. Lameller ichthyosis was present in one child who was detected to have neutral lipid storage disease also called as Dorfman- Chanarin syndrome. This is a very rare and unique condition [16]. Ultrasonography was performed in all patients. Ultrasonography is helpful in the evaluation of ascites, cirrhosis, biliary atresia, portal hypertension [17].
[Table/Fig-2] denotes Wilson’s disease work up. Out of 12 patients of Wilson’s disease, 7 had hepatic manifestations, 3 had neurologic manifestations, and 2 were asymptomatic. Eight patients had positive orcein stain. Siblings were detected to have Wilson’s disease in 4 families. 4 patients had presented with fatal hepatic fibrosis and expired. Data analysing liver histology in patients with Wilson’s disease is available [18,19].
Clinical features and investigations of patients with autoimmune hepatitis in our study were compared with similar study of Kansu and Girgorio as demonstrated in [Table/Fig-3]. Autoimmune Hepatitis was diagnosed when all possible causes of liver disease were ruled out [20]. Autoimmune hepatitis was seen in 6 out of 55 patients. Anti SMA antibody was positive in 7 out of 10 patients, of these 5(83%) were finally diagnosed as autoimmune hepatitis. Anti LKM was positive in 4 (66%) of the 10 patients who were labeled as autoimmune hepatitis. ANF was positive in 5 of the 18 patients, 3 (50%) of them had autoimmune hepatitis; All 6 patients of AIH had raised SGOT/SGPT and normal alkaline phosphatase except one. Of these six, 3 were male, 3 were females.
Metabolic investigations as shown in [Table/Fig-4] included plasma and urine aminoacidogram, blood sugar, ammonia, lipid profile, iron studies, α1-Antitrypsin, MPS spot test from urine and urine for porphobilinogen. Abnormal blood sugar was seen in 3 patients, one was a case of hepatic encephalopathy and other two had glycogen storage disease [Table/Fig-8]. The diagnosis was confirmed on histology. We performed lipid profile in 3 patients it was high in 2 children with neutral lipid storage disorder.
Liver biopsy findings included bridging necrosis, piecemeal necrosis, inflammation, distortion of liver architecture and cirrhosis as shown in [Table/Fig-5]. Liver histology was studied in 55 patients, of which 16 were postmortem samples. Bile lakes and bile duct thrombi favour the diagnosis of EHBA [21]. In our study it was found in all cases of EHBA.
[Table/Fig-6] shows interpretation of liver biopsy in our study. Amongst 18 metabolic cases 2 patients were categorized as α1-Antitrypsin deficiency who died due to hepatic encephalopathy. Their postmortem liver biopsy confirmed material that was positive with PAS stain. Cirrhosis was seen in 23 patients (41.8%). Two patients with glycogen storage disorder type III were diagnosed by performing GTT complemented with biopsy showing PAS positive material with diastase solubility. Neonatal cholestasis syndrome (NCS) includes a wide spectrum of clinical conditions ranging from congenital malformation of hepatobiliary tract, infections, inborn errors of metabolism and other rare conditions. We had 13 cases of NCS (23%), EHBA 4 cases, NH 4 cases, TORCH hepatitis 4 cases and one case of Alagille syndrome [Table/Fig-9]. We diagnosed 3 cases of CMV hepatitis and one patient with toxoplasma infection. Out of these 4 TORCH hepatitis, 3 died. We had one patient of primary sclerosing cholangitis [22] who was HBsAg positive, one patient of non cirrhotic portal fibrosis; the diagnosis was confirmed on USG and liver biopsy. We had one patient who had CLD because of EHBO.
[Table/Fig-7] shows the spectrum of chronic liver diseases in our study. Final diagnosis of each patient was based on clinical features, laboratory features and histopathology. We found liver biopsy was an accurate investigation in 96% of cases and could help to differentiate NH and EHBA. All 9 patients diagnosed as hepatitis, underwent extensive investigations to pinpoint the etiology. Five patients were categorized in miscellaneous group, out of which one patient each of Alagille syndrome and lupus hepatitis and Budd-Chiari syndrome were diagnosed. In Budd- Chiari syndrome, we did DSA with IVC gram, it showed obstruction of the hepatic veins, either due to web or thrombosis; similar case report by Kocher et al., [23].
We did not encounter any complication after liver biopsy as it was done in patients with normal PT/PI with standard protocol for liver biopsy [24]. At our level we were able to offer good treatment to patients with Wilson’s disease, autoimmune hepatitis and GSD. In India, it is estimated that 2 lack patients with end stage liver disease die every year [25].
Comparison of clinical manifestations of patients in our study with the other studies
| Clinical manifestations | Present study (n=55) | Qureshi [7] (n=55) | Malik [8] (n=30) | Mehnaz [9] (n=80) |
|---|
| No | % | No | % | No | % | No | % |
|---|
| Abdominal dist. | 28 | 51 | 44 | 80 | 9 | 30 | 59 | 73.8 |
| Oedema | 16 | 30 | 44 | 80 | 9 | 30 | 59 | 73.8 |
| Jaundice | 40 | 73 | 27 | 49 | 22 | 73 | 40 | 50 |
| Variceal bleed | 15 | 28 | 23 | 42 | 4 | 13 | 12 | 15 |
| Anemia | 31 | 56 | 52 | 95 | 17 | 56 | 60 | 75 |
| Hepatomegaly | 35 | 63 | 35 | 63 | 20 | 66 | 44 | 55 |
| Spleenomegaly | 33 | 60 | 42 | 76 | 19 | 63 | 40 | 50 |
| Ascites | 23 | 41.8 | 46 | 84 | 9 | 30 | 50 | 62.5 |
| S. no. | Investigation for Wilson’s disease | Done in no. of patients | Abnormal results | % of abn. results |
|---|
| 1. | S. ceruloplasmin | 31 | 15 | 48.38 |
| 2. | 24hours urinary copper | 27 | 10 | 37.03 |
| 3. | Post penicillamine 24 hours urinary copper | 17 | 14 | 82.35 |
| 4. | KF ring on slit lamp examination | 35 | 17 | 49 |
| 5. | Dry wt. of copper of liver | 13 | 6 | 46.15 |
| 6. | MRI brain | 4 | 2 | 50 |
| 7. | Family screening | 6 | 4 | 66.66 |
Autoimmune hepatitis- comparison with other studies
| Clinical features | Present study (n=6) | Kansu [10] (n=10) | Girgorio [11] (n=52) |
|---|
| Females | 3 (50%) | 9 | - |
| Mean duration of symptoms (mths) | 4 | 4 | - |
| Mean age at presentation (year) | 5.2 | 10.7 | 10 |
| Jaundice | 6 (100%) | 9 (90%) | - |
| Portal hypertension | 4(66%) | 6 (60%) | - |
| Elevated transaminases | 6(100%) | 10 (100%) | - |
| ANF positive | 3(50%) | 7(70%) | 32(62%) |
| ASMA positive | 5(83%) | 6 (60%) | - |
| Anti LKM positive | 4(66%) | ND | 20(39%) |
| Cirrhosis in histology | 3 (50%) | 3 (30%) | - |
| Survival | 4(66%) | 8 (80%) | - |
Metabolic work up (except wilson’s disease work up)
| S. no. | Name of investigation | Done in no. of patients | Abnormal result present | % of abn. results |
|---|
| 1. | PAA | 8 | - | - |
| 2. | UAA | 7 | - | - |
| 3. | S. NH3 | 29 | - | - |
| 4. | RBS | 50 | 3 | 6% |
| 5. | Lipid profile | 3 | 2 | 66% |
| 6. | Iron studies | 4 | 2 | 50% |
| 7. | -1 antitrypsin | 1 | - | - |
| 8. | Urine MPS | 2 | - | - |
| 9. | Urine PBG | 1 | - | - |
PAA – Plasma aminoacidogram, UAA – Urine aminoacidogram, RBS – Random blood sugar level, MPS – Mucopolysaccharide, PBG – Porphobilinogen
Various histopathological features seen in liver biopsy (n=55)
| S. no. | Histopathological abnormality | No. of patients | % of patients |
|---|
| 1. | Abnormal liver architecture | 32 | 58.18 |
| 2. | Ballooning of hepatocytes | 41 | 74.54 |
| 3. | Cholestasis – canalicular / intrahepatic | 27 | 49.09 |
| 4. | Inflammation mononuclear /mixed | 44 | 80 |
| 5. | Necrosis – focal / piecemeal / massive | 15 | 27.27 |
| 6. | Fibrosis – periportal / bridging | 40 | 72.72 |
| 7. | Glycogenation of hepatocytes | 15 | 27.27 |
| 8. | Special stain positive – (Reticulin / Orcein/PB/PAS/D) | 13 | 23.63 |
| 9. | Cirrhosis | 23 | 41.81 |
Interpretation of liver biopsy (n=55)
| S. no. | Biopsy | Cirrhosis | Non cirrhosis | Total |
|---|
| 1. | Hepatitis | - | 9 | 9 |
| 2. | Autoimmune hepatitis | 3 | 3 | 6 |
| 3. | Wilson’s disease | 9 | 3 | 12 |
| 4. | α-1 Antitrypsin deficiency | 2 | - | 2 |
| 5. | GSD | 1 | 1 | 2 |
| 6. | NLSD | - | 2 | 2 |
| 7. | CMV / Toxoplasma hepatitis | - | 4 | 4 |
| 8. | EHBA | 3 | 1 | 4 |
| 9. | Neonatal hepatitis | 3 | 2 | 5 |
| 10. | Tuberculosis | - | 4 | 4 |
| 11. | Miscellaneous-EHBO Lupus hepatitis | 1 1 | 1 Sclerosing chola. 1 BCS 1 Normal | 5 |
| Total | 23 | 32 | 55 |
NLSD – Neutral Lipid Storage Disorder , EHBO–Extrahepatic biliary obstruction , BCS – Budd -Chiari Syndrome
Spectrum of chronic liver disease (n=55)
| S. no. | System involved | No. of cases | Percentage % |
|---|
| 1. | Metabolic liver disease | 18 | 32.72 |
| 2. | Autoimmune hepatitis | 6 | 10.90 |
| 3. | Hepatitis | 9 | 16.36 |
| 4. | Neonatal hepatitis | 5 | 9.09 |
| 5. | Tuberculosis | 4 | 7.27 |
| 6. | TORCH hepatitis | 4 | 7.27 |
| 7. | EHBA | 4 | 7.27 |
| 8. | Miscellaneous | 5 | 9.09 |
| Total | 55 | 100 |
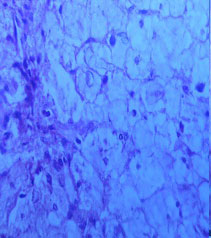
Glycogen Storage Disease (Type IV): Histopathology showing loss of normal architecture, hepatocytes severely distended with granular cytoplasm and glycogenated nuclei
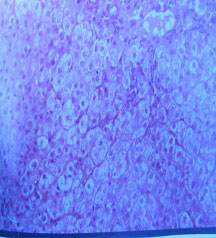
Syndrome: Liver biopsy shows near absence of bile ductules in interlobular septae, pseudoxanthomatous transformation of hepatocytes
Conclusion
Some uncommon causes of CLD in children were seen in our study like Neutral Lipid Storage Disease (2 cases), α1-Antitrypsin deficiency (2cases) and 1 case each of lupus hepatitis, Alagille syndrome and Budd-Chiari syndrome. Detailed information regarding chronic liver disease and family history forms an important source of information for diagnosis of CLD. Absence of jaundice does not rule out CLD. A patient of CLD with jaundice and hepatomegaly and patient with hepatic encephalopathy should be treated aggressively as those are the poor prognostic indicators of the disease. Liver biopsy histopathology by an expert and its correlation with laboratory investigations plays an important role in the diagnosis of CLD. The major cause of deaths in patients with CLD is due to end stage liver disease and fulminant hepatic failure and the only way to prevent and treat these patients is by liver transplantation.
PAA – Plasma aminoacidogram, UAA – Urine aminoacidogram, RBS – Random blood sugar level, MPS – Mucopolysaccharide, PBG – Porphobilinogen
NLSD – Neutral Lipid Storage Disorder , EHBO–Extrahepatic biliary obstruction , BCS – Budd -Chiari Syndrome
[1]. GM Vergani, D Vergani, Autoimmune Liver Disease. In Symposium on HepatologyInd J Paediatr 2002 69(1):93-98. [Google Scholar]
[2]. B Sharda, Recent Advances in Paediatrics- SpecialGastroenterology, Hepatology and Nutrition 2000 617th EditionNew DelhiJaypee:281-83. [Google Scholar]
[3]. Lee Vicky, Ballistreri Nelson’s Textbook of Paediatrics 2004 17th International EditionPhiladelphia, USASaunders:1308-12. [Google Scholar]
[4]. J Snyder, L Pickering, Viral Hepatitis, Nelson’s Textbook of Paediatrics 2004 17th International EditionPhiladelphia, USASaunders:1327-1330. [Google Scholar]
[5]. A Bravo, S Sheth, S Chopra, Liver BiopsyThe New England Journal of Medicine 2001 344:495-500. [Google Scholar]
[6]. Patrick RS, McGee J., Biopsy Pathology of the LiverLondon: Chapman and Hall 1980 7:318-22. [Google Scholar]
[7]. H Qureshi, M Hanif, J Raza, Z Issani, etiology of Chronic Liver Disease in ChildrenJ Pak Med Asso 2004 54(3):119-22. [Google Scholar]
[8]. M Malik, M Hussain, M Aslam, S Magbool, Clinical Spectrum of Chronic Liver Disease in Pakistani Hospitalised ChildrenPakistan Ped J 2000 24:9-12. [Google Scholar]
[9]. A Mehnaz, Chronic Liver Disease in Children An overviewMed Spect 1999 20:7-11. [Google Scholar]
[10]. A Kansu, A Kalayci, B Altuntas, T Doganci, N Girginn, Autoimmune Hepatitis in Children, a Report of Ten CasesTurkey J Med Sci 2000 30:55-61. [Google Scholar]
[11]. G Gregorio, B Portmann, F Reid, P Donaldson, D Doherty, M Mc Cartney, Autoimmune Hepatitis in Childhood, a 20 Year ExperienceHepatology 1997 25:541-47. [Google Scholar]
[12]. NK Arora, R Lodha, P Mathur, N Arora, Child with Chronic Liver DiseasePaediatrics Today 1998 1(2):207-11. [Google Scholar]
[13]. Kumar Clark Clinical MedicineTetracyclineTeratology 2002 5th EditionPhiladelphia, USASaunders:365-366. [Google Scholar]
[14]. J Frederick, Nelson’s Textbook of PaediatricsTetracyclineTeratology 2004 17th International EditionPhiladelphia, USASaunders:1341-43. [Google Scholar]
[15]. A Yuce, N Kocak, F Gurakan, H Ozen, Wilson’s Disease with Hepatic Presentation in ChildhoodInd Paediatr 2000 37(9):31-36. [Google Scholar]
[16]. M Tullu, M Muranjan, S Khubchandani, Dorfaman - Chanarin Syndrome, A rare Neutral Lipid Storage DiseaseInd Paediatr 2000 37(1):88-92. [Google Scholar]
[17]. JA Zhu, B Hu, Ultrasonography in Predicting and Screening Liver Cirrhosis in Children, a Preliminary StudyWorld J Gastroenterol 2003 9(10):2348-49. [Google Scholar]
[18]. V Kalra, D Khurana, R Mittal, Wilson’s Disease, Early onset and Lessons from a Paediatric Cohort in IndiaInd Paediatr 2000 37(6):595-601. [Google Scholar]
[19]. A Pandit, A Bavdekar, S Bhave, Wilson’s diseaseInd J Paediatr 2002 69:785-91. [Google Scholar]
[20]. Roberts Eve A, Autoimmune Hepatitis, Symposium on Hepatology –1Ind J Paediatr 1995 62(5):525-31. [Google Scholar]
[21]. NC Nayak, N Vasdev, Neonatal Cholestasis Syndrome, Identifying the Disease from Liver BiopsyInd. Paediatr 2002 39(5):421-25. [Google Scholar]
[22]. Davison Suzanne, Diseases of the Liver and Biliary System in ChildrenEdinburgh: Blackwell 1999 :110-12. [Google Scholar]
[23]. M Issaivanan, S Kochhar, B Poddar, J Goraya, Budd - Chiari Syndrome, Case ReportInd. Paediatr 2002 39(1):83-84. [Google Scholar]
[24]. Kelly Deirdre A., Diseases of the Liver and Biliary System in Children 1999 EdinburghBlackwell [Google Scholar]
[25]. Sibal Anupam, Recent Advances in Paediatrics- Special Volume 6 Gastroenterology, Hepatology and Nutrition 2000 6New DelhiJaypee:377-80. [Google Scholar]