Background
It was presented that Trichomonas tenax is one of the parasites which is responsible for oral infection. This study was considered to estimate the prevalence of this parasite in oral cavity of Down syndrome patients with periodontal lesions and in healthy population from welfare organization in Tabriz, Iran.
Materials and Methods
In the case-control study, 52 patients with periodontal disease (case group) and 52 individuals with healthy gingiva (control group) selected for the study. Examination was done by dental mirror and periodontal probe. After using plaque detector tablets, sampling was done by entering sterile paper into periodontal pocket for 20 seconds. The amount of plaque was measured by plaque index. Finally samples sent to laboratory for prepared PCR reaction.
Results
In the case group, 14 patients were infected and in the control group 5 individuals. Percentage of infection in case group was 18.8% and in the control group was 3% that difference was statically significant. Plaque index in the case group was 72 ± 10.2 and in the control group was 68 ± 11.4 and difference between two groups was not significant.
Conclusion
Parasitic infections in Down syndrome were higher than healthy children while plaque index was not significantly different between the two groups. Therefore follow-up of orders are necessary in control of parasitic infection in Down syndrome that have intrinsic defect of immune systems.
Anaerobic parasite, Gingivitis, Periodontics
Introduction
The oral cavity of human is colonized by specific bacteria, fungi and protozoa. Among these microorganisms, Trichomonas tenax (T. tenax) is known as common an anaerobic parasite of oral cavity and also found in sub maxillary glands [1].
T. tenax is commonly found in oral cavity and patients with poor oral hygiene and periodontal disease involved. The occurrence of T. tenax is depending on host ‘age. Different factors are responsible for transmission of parasite that includes incidence by saliva through kissing, or application of polluted dishes and drinking water [2,3]. Depending on oral health status, level of contamination is reported between 0 to 25% [2].
Several studies were undertaken in relation to prevalence of periodontal disease in syndrome down (DS) patients (trisomy 21) [4-7]. It has been shown that defective neutrophil chemotaxis influences the progression of periodontal disease in DS patients [8]. Also, the studies display that the level of prostaglandin E2 (PGEl) detected in gingival crevicular fluid (GCF) from DS patients is increased, a fact that may be of importance in the pathogenesis of the periodontal disease frequently seen in these patients [9]. Moreover, pulmonary trichomoniasis is usually caused by aspirated T. tenax [2,10]. Afterwards, health of DS patients could be affected because of this infections and intrinsic defect of the immune system in DS [11]. As correlation to this parasite and periodontal diseases in DS patients, pulmonary trichomoniasis and due to public health importance, this study was performed to determine the prevalence of T. tenaxin oral cavity of DS patients with periodontal disease and in healthy population in Tabriz, Iran.
Materials and Methods
The study comprised 104 individuals that were selected from Welfare Organization of Tabriz, Iran. A total of 52 DS patients (5-12 years old) (24 females and 28 males) with periodontal disease were choice as case group and a total of 52 individuals aged between 5-12 years (31 females and 21 males) without any periodontal disease and healthy gingiva were also picked as control group. Each participant was examined using a dental mirror and a periodontal probe. Then learn how to use plaque disclosing tablets. Individual’s plaque was measured by O’Leary’s index and gingival condition was obtained based on Gingival Index [12]. It scores the marginal and interproximal tissues distinctly on the basis of 0 to 3. The criteria are:
0= Normal gingiva;
1= Mild inflammation – slight change in color and slight edema but no bleeding on probing;
2= Moderate inflammation – redness, edema and glazing, bleeding on probing;
3= Severe inflammation – marked redness and edema, ulceration with tendency to spontaneous bleeding.
A sterile, absorbent paper point was quietly inserted into the periodontal pocket (sulcus). After 20 seconds, the papers were put in a tube having 100μl of NTE buffer {100 mM NaCl, 10 mM Tris-HCl (pH 7.5), 1mM EDTA}. PCR of 18S rRNA gene were used for detection of T.tenax. Total genomic DNA extracted by phenol-chloroform method according to Sambrook. The 18S rRNA gene was amplified directly from dental plaque with the forward and reverse primers TGBK-F and TGBK-R (5′-AGCAGCTGCGGTAATTCCAG-3′ and 5′-CTTGTTACCACTTCTCCTTCC-3′), respectively [13].
A written consent was provided from each patient and the study was approved in the university Ethics Committee. A questionnaire documented the history of patients' general health, any antibiotic consumption (in the three last months), periodontal disease, oral and maxillofacial disease. The statistical analysis was done via SPSS software (Version 11.5) by t-test and Chi-square test to study the correlation between the kind of oral disease, age and sex with the existence of T.tenax.
Results
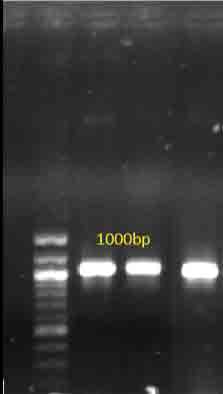
In the case group, 14 DS patients (26.9%) and in the control group 5 individuals (9.6%) were infected to T. tenax and were positive in the PCR [Table/Fig-1,2]. Amplification was approximately 1000 bp that was compatible with published reports [13].
Comparing gingivitis index show that difference between these two groups (case and control) is statistically significant (p<0.001, X2=23.76). But comparing gingivitis index between female and male of the case group (p>0.05, X2=23.76) statistically non-significant. Also, in the control group difference between female and male was statistically non-significant [Table/Fig-3].
Comparing of means on percentage of plaque index was shown in [Table/Fig-4]. According to the result, variances of two groups (case and control) were not equal and this difference was statically nonsignificant. While variances between female and male in case and control group were equal and statically non- significant. Comparison of positive infection to T.tenax in two groups by fisher test showed that difference was statically significant (X2= 5.21, p<0.05). But difference between female and male of two groups was nonsignificant [Table/Fig-5]. Comparison of positive infection to T.tenax between female by fisher test revealed that difference was statically non- significant (X2= 1.24, p > 0.05). But difference between female and was significant. (X2= 4.73, p <0.05) [Table/Fig-6].
Discussion
The result of this study presented that percent of infection to T.tenax and gingival index in the case group (DS patients) were significantly higher than control group although no significant difference was found in plaque index results between the groups. DS patients mostly would be involved in periodontal disease due to poor oral hygiene, irregular teeth and high frenum attachment. For this reason, it is expected that prevalence of T.tenax in DS patients be higher than healthy children and the result of this study exhibited this subject. Percentage of infection to T.tenax was 26.9%. In the previous study, range of infection to this parasite, between children aged 2-12- year-old, reported approximately 4% [14]. Also, showed that DS patients have inappropriate activity of matrix metalloproteinase that increased the risk of periodontal disease [15]. As well as, T.tenax could produce cathepsin B-like proteinases that affect pathological process such as facilitate penetration of the host, digestion of host proteins and interference with the host immune system [16]. Also, in patients with marginal periodontitis or gingivitis, detection of E. gingivalis and T. tenax were examined. According to the results, Entamoeba gingivalis was more dominant among females, whereas T. tenax was not found in both patients and control groups [17].
In the other study prevalence of E. gingivalis and T. tenax were investigated which patients have gingivitis and scale. Results showed that in 48 (21.8%) of the positive 58 specimens, E. gingivalis was discovered alone while T. tenax was present in only two (1%) specimens. In 8 (3.6%) cases, E. gingivalis and T. tenax were recognized together. In addition, other factor such as gum problems, existence of tartar, smoking, brushing and control habits were establish to be statistically significantly associated with the oral protozoa [18].
In the other same study, prevalence of E. gingivalis and T. tenax in oral parasitic infection was evaluated. According to their results, nine infection (6 with E. gingivalis and 3 with T. tenax) in the case group were determined but in the control group just one infection by E.gingivalis was reported [6].
Another research on diagnosis of E. gingivalis and T. tenax was done between 176 specimens (8 to 19-year-old). Finding showed that 25 subjects (14.2%) had only E. gingivalis, 5 (2.9%) had an invasion of E. gingivalis and T. tenax together and 2 individuals (1.1%) had only T. tenax. Result established that oral protozoa was found in the groups (children and teenagers) with having cured or complete dentition. Occurrence rate of parasite was higher in 11 to 19-year-old persons than in the lower age groups. Also, both investigated protozoa can arise simultaneously such that their occurrence rate was deepened on age (increasing with age in rate of E. gingivalis) and sex dependent (rate is higher in boys than girls) [19]. It is noted that DS patients have intrinsic defect of the immune system [11], therefore these results confirmed that DS patient could be more prone to T.tenax infection. Beside determination T.tenax in periodontal patients, it was showed that frequency of occurrence of parasite dependence on state of periodontium and hygiene of oral cavity [20]. It is thought that this parasite could enter into respiratory tract from oropharynx by aspiration. Either determined that it feed from bacteria and alone not able to make pulmonary disease and co-infection was accruing between parasite and bacterial flora of oropharynx [21]. On the other hand clinical and epidemiological studies showed close relationship between plaque and periodontal disease. Which in the poor removal of plaque, gingivitis was created and caused progressive periodontitis [22]. According to our results, it is necessary to following oral and general hygiene order to control of parasitic infestations, especially between DS patients which inhibit progress of periodontal disease and related infection such pulmonary trichomoniasis in DS patients.
PCR products on the basis of Trichomonas tenax 18S rRNA gene. M: molecular size marker; 100bp
Prevalence of Trichomonas tenax according to the positive PCR bond
| Gender | Examined individual | Positive | % |
|---|
| Case group | female | 24 | 8 | 33.3 |
| male | 28 | 6 | 21.4 |
| total | 52 | 14 | 26.9 |
| Control group | female | 31 | 3 | 9.7 |
| male | 21 | 2 | 9.5 |
| total | 52 | 5 | 9.6 |
Comparison gingivitis index between groups
| | | groups | Total |
|---|
| Case | control |
|---|
| Male | female | total | Male | female | total |
|---|
| gingivitis index | 0 | frequency | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| % | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1 | frequency | 0 | 0 | 0 | 8 | 10 | 18 | 18 |
| % | 0 | 0 | 0 | 38.1 | 32.3 | 34.6 | 17.3 |
| 2 | frequency | 16 | 11 | 27 | 10 | 13 | 23 | 50 |
| % | 57.1 | 45.8 | 51.9 | 47.6 | 41.9 | 44.2 | 48.1 |
| 3 | frequency | 12 | 13 | 25 | 3 | 8 | 11 | 36 |
| % | 42.9 | 54.2 | 48.1 | 14.3 | 25.8 | 21.2 | 34.6 |
| total | | frequency | 28 | 24 | 52 | 21 | 31 | 52 | 104 |
| % | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
Comparison of means on percentage of plaque index
| groups | number | mean | DS* | Deviation of the mean | F | p-value | t | df | p-value |
|---|
| control | 52 | 69.17 | 5.74 | 0.79 | 40.30 | 0.000 | 1.90 | 78.39 | 0.06 |
| case | 52 | 72.36 | 10.63 | 1.47 |
| female (case) | 24 | 73.59 | 9.85 | 2.01 | 2.12 | 0.15 | 0.77 | 50 | 0.44 |
| Male (case) | 28 | 71.301 | 11.32 | 2.14 |
| female (control) | 31 | 68.74 | 5.701 | 1.02 | 0.406 | 0.52 | 0.64 | 50 | 0.52 |
| Male (control) | 21 | 69.79 | 5.88 | 1.28 |
*Deviation Standard
Comparison of infection to T.tenax in two groups
| | | Group | total | total |
|---|
| control | case |
|---|
| male | female | total | male | female | total |
|---|
| Infection to T.tenax | positive | frequency | 2 | 3 | 5 | 6 | 8 | 14 | 19 |
|---|
| % | 9.5 | 9.7 | 9.6 | 21.4 | 33.3 | 26.9 | 18.3 |
| negative | frequency | 19 | 28 | 47 | 22 | 16 | 38 | 85 |
| % | 90.5 | 90.3 | 90.4 | 78.6 | 66.7 | 73.1 | 81.7 |
| total | frequency | 21 | 31 | 52 | 28 | 24 | 52 | 104 |
| % | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
Comparison of positive infection to T.tenax between male and female
| | | Group | total |
|---|
| control | case |
|---|
| male | female | total | male | female | total |
|---|
| Infection to T.tenax | positive | frequency | 6 | 2 | 8 | 8 | 3 | 11 |
|---|
| % | 21.4 | 9.5 | 16.3 | 33.3 | 9.7 | 20 |
| negative | frequency | 22 | 19 | 41 | 16 | 28 | 44 |
| % | 78.6 | 90.5 | 83.7 | 66.7 | 90.3 | 80 |
| total | frequency | 28 | 21 | 49 | 24 | 31 | 55 |
| % | 100 | 100 | 100 | 100 | 100 | 100 |
Conclusion
According to children dental health especially in Down syndrome, detection of parasites responsible to infection is very important. T.tenax was one of parasite determined in DS patients in this study because these children had not high oral hygiene. So for this reason were will be exposure to other high risk disease like as trichomoniasis by infection of T.tenax. Furthermore it is being mentioned that oral health and existence of inflammation is affected T.tenax infection thus identification of this infection in DS patients help them to have healthy oral and teeth. In our study gingivitis and gingiva index was high in DS patients comparing control group. Finally, it can be concluded that DS children should receive dental care to have low infection to T.tenax, related pulmonary disease and gain high hygiene oral cavity.
*Deviation Standard
[1]. C Duboucher, M Mogenet, G Perie, Salivary trichomoniasis. A case report of infestation of a submaxillary gland by Trichomonas tenaxArch Pathol Lab Med 1995 119(3):277-79. [Google Scholar]
[2]. SM Hersh, Pulmonary trichomoniasis and Trichomonas tenaxJ Med Microbiol 1985 20(1):1-10. [Google Scholar]
[3]. G Radosavljevic-Asic, Trichomonas in pleural effusionEur Respir J 1994 7(10):1906-08. [Google Scholar]
[4]. D Boyd, A Quick, C Murray, The Down syndrome patient in dental practice, Part II: clinical considerations N Z Dent J 2004 100(1):4-9. [Google Scholar]
[5]. J Merrick, J Shapira, Dental concerns in Down syndromeInt J Adolesc Med Health 2000 12(1):75-80. [Google Scholar]
[6]. J Ghabanchi, Prevalence of oral Entamoeba gingivalis and Trichomonas tenax in patients with periodontal disease and healthy population in Shiraz, southern Iran.Indian J Dent Res 2010 21(1):89-91. [Google Scholar]
[7]. A Frydman, H Nowzari, Down syndrome-associated periodontitis: a critical review of the literatureCompend Contin Educ Dent 2012 33(1):356-61. [Google Scholar]
[8]. Y Izumi, Defective neutrophil chemotaxis in Down's syndrome patients and its relationship to periodontal destructionJ Periodontol 1989 60(5):238-42. [Google Scholar]
[9]. M Barr-Agholme, Prostaglandin E2 Level in Gingival Crevicular Fluid from Patients with Down Syndrome Acta Odontologica Scandinavica 1997 55(3):101-05. [Google Scholar]
[10]. MM El Sibaein, Growth kinetics, antigen profiling, and proteinase activity of Egyptian Trichomonas tenax isolates derived from patients having oral infectionsExp Parasitol 2012 130(4):416-22. [Google Scholar]
[11]. MA Kusters, Intrinsic defect of the immune system in children with Down syndrome: a reviewClin Exp Immunol 2009 156(2):189-93. [Google Scholar]
[12]. H Löe, J Silness, Periodontal Disease in Pregnancy I. Prevalence and SeverityActa Odontologica Scandinavica 1963 21(6):533-51. [Google Scholar]
[13]. Thai Kristina, Stander Duran, Rogers Joel, Shon Jae Ryong, The Prevalence of Entamoeba gingivalis and Trichomonas tenax in Tropical North Oueensland OfficialJournal of The Australasian College of Tropical Medicine 2013 14(1):27 [Google Scholar]
[14]. WW Wantland, D Lauer, Correlation of some oral hygiene variables with age, sex, and incidence of oral protozoaJ Dent Res 1970 49(2):293-97. [Google Scholar]
[15]. S Halinen, Characterization of matrix metalloproteinase (MMP-8 and -9) activities in the saliva and in gingival crevicular fluid of children with Down's syndromeJ Periodontol 1996 67(8):748-54. [Google Scholar]
[16]. A Yamamoto, Characterization of the cathepsin B-like proteinases of Trichomonas tenax ATCC 30207Oral Microbiol Immuno 2000 15(6):360-4. [Google Scholar]
[17]. IA el Hayawan, MM Bayoumy, The prevalence of Entamoeba gingivalis and Trichomonas tenax in periodontal diseaseJ Egypt Soc Parasitol 1992 22(1):101-15. [Google Scholar]
[18]. S Ozcelik, Investigation of the relationship between oral and dental health and presence of Entamoeba gingivalis and Trichomonas tenax Turkiye Parazitol Derg 2010 34(4):155-59. [Google Scholar]
[19]. J Vrablic, Morphology and diagnosis of Entamoeba gingivalis and Trichomonas tenax and their occurrence in children and adolescentsBratisl Lek Listy 1991 92(5):241-46. [Google Scholar]
[20]. AJ Kurnatowska, A Dudko, P Kurnatowski, Invasion of Trichomonas tenax in patients with periodontal diseasesWiad Parazytol 2004 50(3):397-403. [Google Scholar]
[21]. H Mallatn, Molecular characterization of Trichomonas tenax causing pulmonary infectionJournal of clinical microbiology 2004 42(2):3886-87. [Google Scholar]
[22]. J Lindhe, SE Hamp, H Loe, Plaque induced periodontal disease in beagle dogs. A 4-year clinical, roentgenographical and histometrical studyJ Periodontal Res 1975 10(5):243-55. [Google Scholar]