Introduction
An unpleasant dental appearance can stigmatize a person, hinder professional achievement, encourage negative stereotypes, and have a negative effect on self-esteem. In strict sense of definition, any deviation from normal occlusion can be termed as malocclusion, which may vary from a very slight deviation of a tooth position in the arch to a significant malpositioning of a group of teeth or jaws [1].
Class II division 1 malocclusion is described as a distal relationship of the mandible to the maxilla with labioversion of maxillary incisors which is relatively more prevalent in North Indian population. Class II malocclusion is a complex clinical entity that entails a combination of different three-dimensional dental and skeletal components adversely affecting facial aesthetics [2]. The many combinations regarding the mutual position between the maxilla and mandible in the sagittal plane of class II subjects has been extensively studied mainly for the classification purposes [3]. Also, if we examine the patients with Class II Division 1 malocclusions then often there is transverse discrepancy between the dental arches, reason for which is understood to be reduction in maxillary width.
The reduction in maxillary width has not been extensively studied in the mixed dentition period although a few studies done (Staley et al., [4], Tollaro et al., [5], Baccetti et al., [6]) indicate that the transverse discrepancy can act as an additional input signal for the anteroposterior adjustment between the skeletal bases during developmental stages [3]. To add further, it is important to study whether this discrepancy can be a possible functional cause of distocclusion.
Posterior transverse discrepancy as seen in some cases of Class II Division 1 malocclusion in mixed dentition period can be related to typical skeletofacial characteristics. These features when studied early in the mixed dentition period give a clear view of the desired appropriate treatment plan in a particular case.
The purpose of this study is to establish a simple method to determine the posterior (intermolar) transverse discrepancy between the dental arches during the mixed dentition by absolute intermolar width measurements. Furthermore, craniofacial skeletal features were studied to provide diagnostic and therapeutic guidance in the early approach to Class II Division 1 malocclusion.
Materials and Methods
This study included a sample of 90 subjects in the age group of 7-13 years from the Department of Paediatric and Preventive Dentistry, Guru Nanak Dev Dental College and Research Institute, Sunam, India. The sample consisted of 30 Class II Division 1 subjects with posterior transverse interarch discrepancy (PTID) and 30 Class II Division 1 subjects without PTID and 30 subjects with Class I molar relation taken as control. The subjects were chosen within the mixed dentition period. The patients were examined according to the selection criterion chosen.
Selection Criterion for Class II Division 1 sample-
• Bilateral class II molar relationship in centric occlusion
• Protrusion of maxillary incisors
• No significant medical history
• No history of trauma
• No previous orthodontic, prosthodontic treatment, maxillofacial or plastic surgery
• Absence of congenitally missing teeth
• Absence of traumatic loss of maxillary incisors
• Absence of class II occlusal interferences, such as palatally positioned anterior teeth
No posterior crossbite
• Selection criterion for Class I sample
• Class I molar relationship
• Well-aligned upper and lower dental arches
• Good facial symmetry
• Absence of trauma
• Absence of a medical problem
• No previous orthodontic,
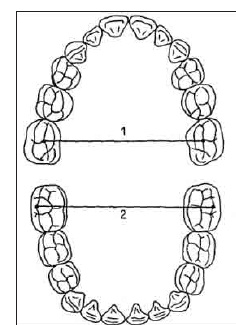
After complete intraoral examination alginate impressions were made for both Class II Division 1 subjects and control (with ideal occlusion) subjects. The following measurements were taken on the dental casts [Table/Fig-1] of subjects with Class II Division 1 malocclusion with the help of digital vernier calliper -
1. Maxillary intermolar width - distance between the central fossa of left and right maxillary first molars [5].
2. Mandibular intermolar width - distance between the tips of distobuccal cusps of right and left mandibular first molars [5].
3. Posterior transverse interarch discrepancy (PTI D) - difference between the maxillary and mandibular intermolar widths [5].
Since, in the Class I molar relationship, the distobuccal cusp of the mandibular molar occludes with the central fossa of the first maxillary molar. Consequently in Class I relation, the maxillary and mandibular intermolar width is same, so PTID is zero.
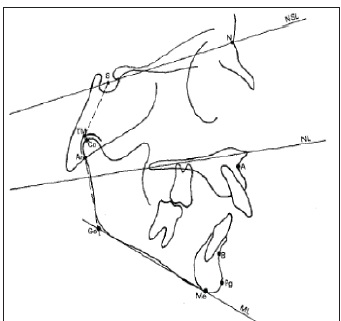
According to the results of cast analysis, the Class II division 1 subjects were further divided into Group A and Group B; according to selected criterion, both including 30 subjects and rest of the samples not fulfilling the criterion were discarded. Group C including 30 subjects with Class I molar relation was taken as control. After performing the measurements on the casts and dividing the patients into their respective groups, standardized lateral cephalograms of all these subjects were taken with the same X-ray device by a single technician [7,8]. The focus median plane is 152 cm and the film median plane distance is 10 cm, allowing an enlargement of 5-7% [Table/Fig-2] [9].
Cephalometric Measurements Done Are
1. Anteroposterior relationships [10]
• Maxillary sagittal position: SNA angle
• Mandibular sagittal position: SNB angle
• Maxillomandibular sagittal discrepancy: ANB angle
• Anteroposterior position of the glenoid fossa: N-S-TM Angle
2. Vertical relationships [11]
• Maxillary inclination relative to cranial base: NL/NSL angle
• Mandibular inclination relative to cranial base: ML/NSLangle
• Maxillomandibular vertical relationship: NL/ML angle
• Gonial angle: Ar-Go-Me angle
3. Mandibular dimensions [12]
• Length of mandibular body: Go-Pg
• Length of mandibular ramus: Co-Go
• Total body length: Co-Pg
The results were tabulated and statistically analysed. The normal values were determined according to the standard norms [13,14].
Results
Descriptive statistics for dental cast analysis and cephalometric measurements are shown in [Table/Fig-3,4,5,6].
Dental Cast Analysis: The results showed that posterior transverse interarch discrepancy (PTID) in Class II (1) PTID was due to a narrower maxillary intermolar width when compared with the Class II (1) NPTID and Class I control group (p= 0.008). However, mandibular intermolar width was not significantly different among the three groups (p= 0.808).
Cephalometric measurements: The comparison between both Class II Groups and Class I control group revealed no statistically significant differences for the sagittal position of the maxilla (p= 0.127), whereas both Class II groups showed a significant mandibular retrusion (p<0.001). It was observed that both the Class II Division 1 malocclusion groups showed a statistically significant lower Ar- Go-Me angle when compared to the Class I group in the mixed dentition period (p= 0.001). The three groups were homogeneous as to anteroposterior position of the glenoid fossa and vertical relationships. The analysis of mandibular dimensions showed a statistically significant smaller body and total lengths of the mandible in Class II (1) NPTID when compared with Class II (1) PTID and with Class I group. (p>0.05)
Discussion
The many combinations regarding the mutual position between the maxilla and mandible in the sagittal plane of Class II subjects has been extensively studied mainly for the classification purposes [3]. However, clinical examination of patients with Class II Division 1 malocclusions often reveals a transverse discrepancy between the dental arches, generally attributed to the reduction in maxillary width [3]. Staley et al., extensively assessed transverse maxillary deficiency and posterior crossbite tendency in a Class II sample when compared to Class I sample in adults and they concluded that patients with Class II Division 1 malocclusion had narrower maxillary intercanine, intermolar, and alveolar widths [4]. Tollaro et al., proved that an underlying negative posterior transverse interarch discrepancy (PTID) (i.e., a narrow maxillary arch when compared with the mandibular arch) exists in dental arches with Class II malocclusion and seemingly normal buccal relationships [5]. Baccetti et al., demonstrated that a negative PTID is recorded consistently in Class II subjects in the deciduous dentition and this negative PTID is maintained or it worsens in the transition to the mixed dentition [6].
A general perception is that maxillary arch width is narrow in Class II patients. However, the reduction in maxillary width has not been extensively studied in the mixed dentition period although a few studies (Staley et al., Tollaro et al., Baccetti et al.,) indicate that the transverse discrepancy can act as an additional input signal for the anteroposterior adjustment between the skeletal bases during developmental stages [2,4-6].
The results of this study showed that posterior transverse interarch discrepancy (PTID) in Class II (1) PTID was due to a narrower maxillary intermolar width when compared with the Class II (1) NPTID and Class I control group. However, mandibular intermolar width was not significantly different among the three groups. Furthermore, the comparison between both Class II Groups and Class I control group revealed no statistically significant differences for the sagittal position of the maxilla, whereas both Class II Groups showed a significant mandibular retrusion. It was observed that both the Class II Division 1 malocclusion groups showed a statistically significant lower Ar- Go-Me angle when compared to the Class I Group in the mixed dentition period. The three groups were homogeneous as to anteroposterior position of the glenoid fossa and vertical relationships. The analysis of mandibular dimensions showed a statistically significant smaller body and total lengths of the mandible in Class II (1) NPTID when compared with Class II (1) PTID and with Class I Group.
The classification system identified in this study has led us to divide Class II Division 1 malocclusion groups into two groups on the basis of their transverse component and after the determination of various dental and skeletal parameters in these groups and comparing them with each other and with the normal Class I patients. It could be concluded that different treatment strategies could be planned according to the transverse component of Class II Division 1 groups in the mixed dentition period.
1. Class II cases with PTID need a preliminary expansion of the maxillary arch. Subsequently, the sagittal position of the mandible should be monitored, as a forward repositioning of the lower jaw may take place spontaneously. If not, functional forward guidance of the mandible has to be attained [5].
2. Class II cases without PTID do not need an early treatment phase of maxillary expansion.
The immediate aim of therapy is to attempt to increase the total length of the mandible. Condylar cartilage growth should be optimally stimulated through proper functional appliances, in accordance with the literature [5].
Finally, this study confirmed the role of occlusion in the control of maxillomandibular skeletal relationships. It should be stressed that the transverse component of occlusal patterns represents an additional input signal for the anteroposterior adjustment between the skeletal bases during developmental ages. Transverse interarch discrepancy due to a narrow maxillary intermolar width may be considered as a possible functional cause of distocclusion.
Dental cast measurements [5]
1. Maxillary intermolar width
2. Mandibular intermolar width
Cephalometric planes used in the study [5]
Mean values and the statistical derivatives of dental cast analysis for the three groups
| | N* | Mean±SD** | SE*** | Minimum | Maximum |
|---|
| Maxillary Intermolar width | Group A | 30 | 44.6337±2.53803 | .46338 | 40.39 | 48.81 |
| Group B | 30 | 46.3677±2.95978 | .54038 | 39.53 | 50.72 |
| Group C | 30 | 46.6860±2.56288 | .46792 | 43.03 | 51.01 |
| Mandibular Intermolar Width | Group A | 30 | 46.2293±2.81925 | .51472 | 41.75 | 50.65 |
| Group B | 30 | 46.3593±2.95988 | .54040 | 39.53 | 50.73 |
| Group C | 30 | 46.6860±2.56288 | .46792 | 43.03 | 51.01 |
*N- Number of Patients in Each Group
**SD- Standard Deviation
***SE- Standard Error
Intergroup comparisons for dental cast measurements among the groups
| | Sig. |
|---|
| Maxillary Intermolar Width | Between Groups | 0.008** |
| Mandibular Intermolar Width | Between Groups | 0.808 |
p<0.05 = significant; p>0.05 = non- significant; p <0.001 = highly significant; *= significant; **=highly significant
Mean values and the statistical derivatives of cephalometric measurements for the three groups
| | N | Mean±Std. Deviation | Std. Error |
|---|
| SNA | GROUP A | 30 | 81.3667±3.45895 | .63152 |
| GROUP B | 30 | 82.1667±3.10820 | .56748 |
| GROUP C | 30 | 82.9333±2.13240 | .38932 |
| SNB | GROUP A | 30 | 74.0333±3.59581 | .65650 |
| GROUP B | 30 | 75.3333±3.20918 | .58591 |
| GROUP C | 30 | 79.4000±2.42970 | .44360 |
| ANB | GROUP A | 30 | 7.0667±1.63861 | .29917 |
| GROUP B | 30 | 6.5000±1.30648 | .23853 |
| GROUP C | 30 | 3.4667±1.07425 | .19613 |
| N-S-TM | GROUP A | 30 | 128.9667±4.42160 | .80727 |
| GROUP B | 30 | 133.1000±8.45006 | 1.54276 |
| GROUP C | 30 | 130.9667±7.94587 | 1.45071 |
| NL/NSL | GROUP A | 30 | 7.9333±1.89251 | .34552 |
| GROUP B | 30 | 8.2667±2.18037 | .39808 |
| GROUP C | 30 | 7.8000±1.84578 | .33699 |
| ML/NSL | GROUP A | 30 | 30.2000±4.87357 | .88979 |
| GROUP B | 30 | 28.7667±3.97998 | .72664 |
| GROUP C | 30 | 30.9667±3.87283 | .70708 |
| NL/ML | GROUP A | 30 | 23.1667±5.16008 | .94210 |
| GROUP B | 30 | 22.3667±3.92589 | .71677 |
| GROUP C | 30 | 24.8667±3.35007 | .61164 |
| Ar-Go-Me | GROUP A | 30 | 122.2333±3.68298 | .67242 |
| GROUP B | 30 | 122.9333±6.73608 | 1.22983 |
| GROUP C | 30 | 126.7667±3.11485 | .56869 |
| Go- Pg | GROUP A | 30 | 72.8333±4.36351 | .79666 |
| GROUP B | 30 | 68.3333±5.48561 | 1.00153 |
| GROUP C | 30 | 71.3000±4.10340 | .74918 |
| Co-Go | GROUP A | 30 | 53.7333±4.62328 | .84409 |
| GROUP B | 30 | 55.2333±5.39274 | .98457 |
| GROUP C | 30 | 53.3333±6.79926 | 1.24137 |
| Co- Pg | GROUP A | 30 | 104.1333±4.90414 | .89537 |
| GROUP B | 30 | 98.7333±4.17656 | .76253 |
| GROUP C | 30 | 102.9667±6.77970 | 1.23780 |
Intergroup comparisons for cephalometric measurements among the groups
| Level of Significance |
|---|
| SNA | 0.127 |
| SNB | <0.001** |
| ANB | <0.001** |
| N-S-TM | 0.088 |
| NL/NSL | 0.644 |
| ML/NSL | 0.134 |
| NL/ML | 0.069 |
| Ar-Go-Me | 0.001** |
| Go-Pg | 0.001** |
| Co-Go | 0.397 |
| Co-Pg | <0.001** |
p<0.05 = significant; p>0.05 = non- significant; p <0.001 = highly significant; *= significant; **=highly significant
Conclusion
This study concluded that the skeletal features of the Class II group without PTID are those of the skeletal Class II associated with ‘anatomic’ mandibular retrusion (due to a micrognathic mandible) and those of the Class II group with PTID as skeletal Class II associated with only a ‘functional’ mandibular retrusion (due to a posteriorly displaced mandible of normal size). The role of occlusion in the control of maxillomandibular skeletal relationships was confirmed so the treatment strategies could be planned on the basis of the transverse component of Class II Division 1 groups in the mixed dentition period.
*N- Number of Patients in Each Group**SD- Standard Deviation***SE- Standard Error
p<0.05 = significant; p>0.05 = non- significant; p <0.001 = highly significant; *= significant; **=highly significant
p<0.05 = significant; p>0.05 = non- significant; p <0.001 = highly significant; *= significant; **=highly significant
[1]. OP Kharbanda, Orthodontics: diagnosis and management of malooclusion and dentofacial deformities Mosby Elsevier India 2009 :28-45. [Google Scholar]
[2]. M Alarashi, L Franchi, A Marinelli, E Defraia, Morphometric Analysis of the Transverse Dentoskeletal Features of Class II Malocclusion in the Mixed DentitionAngle Orthodontist 2003 73(1):21-25. [Google Scholar]
[3]. A Marinelli, M Mariotti, E Defraia, Transverse dimensions of dental arches in subjects with Class II malocclusion in the early mixed dentitionProgress in orthodontics Mediterranean journal of orthodontics 2011 12:31-37. [Google Scholar]
[4]. RN Staley, RO Stuntz, LC Peterson, A comparison of arch width in adults with normal occlusion and adults with class II div 1 malocclusionAmerican Journal of Orthodontics and Dentofacial Orthopaedics 1985 88:163-69. [Google Scholar]
[5]. I Tollaro, T Baccetti, L Franchi, CD Tanasescu, Role of posterior transverse interarch discrepancy in Class II, Division 1 malocclusion during the mixed dentition phaseAmerican Journal of Orthodontics and Dentofacial Orthopedics 1996 101:417-22. [Google Scholar]
[6]. T Baccetti, L Franchi, JA McNamara, I Tollaro, Early dentofacialfeatures of Class II malocclusion: a longitudinal study from the deciduous through the mixed dentitionAmerican Journal of Orthodontics and Dentofacial Orthopedics 1997 11:502-09. [Google Scholar]
[7]. AE Athanasiouy, Orthodontic cephalometryMosby-Wolfe 1995 [Google Scholar]
[8]. KJ Kumar, A handbook of cephalometric norms for Indian ethnic groupsIndiaThe Indian Orthodontic Society [Google Scholar]
[9]. JA Mc Namara, Components of class II malocclusion in children 8-10 years of age Angle orthodontist 1981 51:177-202. [Google Scholar]
[10]. CC Steiner, Cephalometrics for you and meAmerican Journal of Orthodontics and Dentofacial Orthopedics 1953 39:729-55. [Google Scholar]
[11]. CC Steiner, Cephalometrics in Clinical PracticeAngle Orthodontist 1959 29(1):8-29. [Google Scholar]
[12]. T Rakosi, An atlas and manual of cephalometric radiography 1981 Year Book Medical Publishers [Google Scholar]
[13]. RE Moyers, Handbook of Orthodontics 1988 4th EditionYear Book Medical Publishers:292-96. [Google Scholar]
[14]. A Jacobson, L Jacobsonn, Radiographic cephalometry: from basics to 3-D imaging 2006 Quintessence publications [Google Scholar]