National guidelines and standards of care for diabetes are now available in many countries in the world [1–3]. Despite high prevalence of diabetes, serious long term complications and established evidence-based guidelines for management [1–3], translation of practice recommendations to care is still deficient in Asian [4–5] and developed countries [6–9].
Available literature suggests that the management of diabetes in India is sub-optimal for the majority of patients. Only 40–50% of individuals achieve the target for glycemic control, while lower numbers achieve targets for blood pressure and lipid control [4,10,11]. Studies from other countries have identified several provider and patient-related factors which can influence outcome measures in people with diabetes [12,13].
It is important to assess the quality of diabetic care to identify the extent of lacunae and its reasons to suggest measures to address the same. The present study is an attempt in this direction.
To assess the quality of care provided to diabetic patients attending the medicine outpatient department by using quality indicators laid down by the National Diabetes Quality Improvement Alliance [14].
To assess the extent of knowledge transfer by the provider to the patients regarding diabetes and its complications as a measure of the quality of service.
Materials and Methods
The study design was cross-sectional where the diabetic patients were interviewed by the principal investigator. The audit was conducted among 190 patients with diabetes who attended the Medicine outpatient department over a period of 6 months from Feb 2011 to July 2011. All type II diabetic patients, 30 years and above, who were diagnosed at least one year back without any other co-morbidity satisfied the inclusion criteria. The purpose of the study was explained to the patients and informed consents were taken from those who were willing to take part in the study. The interview schedule included basic demographic data, process indicators, outcome indicators and questions to assess the knowledge of the diabetic patients.
The study methodology comprised of an audit to assess the quality of care provided to the diabetic patients using the quality indicators for diabetes care. These indicators were formulated by the National Diabetes Quality Improvement Alliance based on the priority measures and indicators recommended by American Diabetes Association, American Medical Association, American College of Physicians, Agency for Healthcare Research and Quality, American Academy of Family Physicians, American Association of Clinical Endocrinologists and other well accepted international diabetic guidelines. The audit checklist consisted of diabetes specific process and outcome indicators. The process indicators consist of basic tests that are required to be done in a patient with diabetes. The proximal outcome measures laid down criteria for HB1Ac, BP and LDL cholesterol in the context of evaluating the quality of care [Table/Fig-1].
Audit checklist for quality of care
| Process measures |
| Percentage of patients with one or more HbA1c tests annually |
| Percentage of patients with at least one LDL cholesterol test annually |
| Percentage of patients with at least one test for microalbuminuria during the measurement year or who had evidence of medical attention for existing nephropathy |
| Percentage of patients who received a dilated eye examination or evaluation of retinal photography by an ophthalmologist or optometrist during the current year or during the prior year if the patient is at low risk of retinopathy |
| Percentage of patients receiving at least one foot examination annually |
| Percentage of patients whose smoking status was ascertained and documented annually |
| Outcome measures |
| Percentage of patients with most recent HbA1c level >9.0% ( poor control) |
| Percentage of patients with most recent LDL cholesterol <130 mg/dl |
| Percentage of patients with most recent blood pressure <140/90 mmHg |
Source: National Diabetes Quality Improvement Alliance [14]
There were five process indicators and each positive response was given a score of one. A score of five or more was considered good and any score less than or equal to three was considered poor. Similarly each positive response for a proximal outcome indicator was given a score of one. A score of three was considered as good and score of 0 was considered poor.
Diabetes is a disease for which 95% of the care lies with the patient. A good quality service should transfer the knowledge about the disease condition, its complications, the behaviour modifications which it warrants and the importance of regularity of the follow up. Therefore, the level of knowledge provided is critical to patients’ ability to care well for their diabetes and the assessment in turn indicates the quality of care given to the patients [15].
The diabetic knowledge was assessed by a semi structured questionnaire which measured the knowledge in four key concepts in Diabetes care namely chronicity, knowledge about target blood sugar level, life style modifications (diet and exercise) and complications (Hypoglycemia, complications related to heart and kidney). There were a total of nine questions and each correct response carried one mark. The knowledge was interpreted as poor, average and good, if the scores were less than 4, 4-6 and more than 7 respectively. The study was approved by the Institutional Review Board of the hospital.
Statistical Analysis
Data was entered in Microsoft Excel and analysis was done using SPSS version 20. Descriptive analysis was done for all the variables. Frequencies, percentages were calculated for categorical variables and mean and standard deviation was calculated for continuous variables like scores. Chi-square test was done to find the association of quality of care indicators with variables age, gender, education, duration of disease etc. ANOVA was used to compare the knowledge scores with the standard of quality of care indicators.
Results
More than half (59.5%) of the studied population were between the age group of 30 and 60 years, almost half (50.5%) were females. One fifth of them (23.2%) were illiterate and 35.8% were graduates. 24.7% were professionals and another 20% were engaged in agriculture. About half those (56.8%) had diabetes for less than five years.
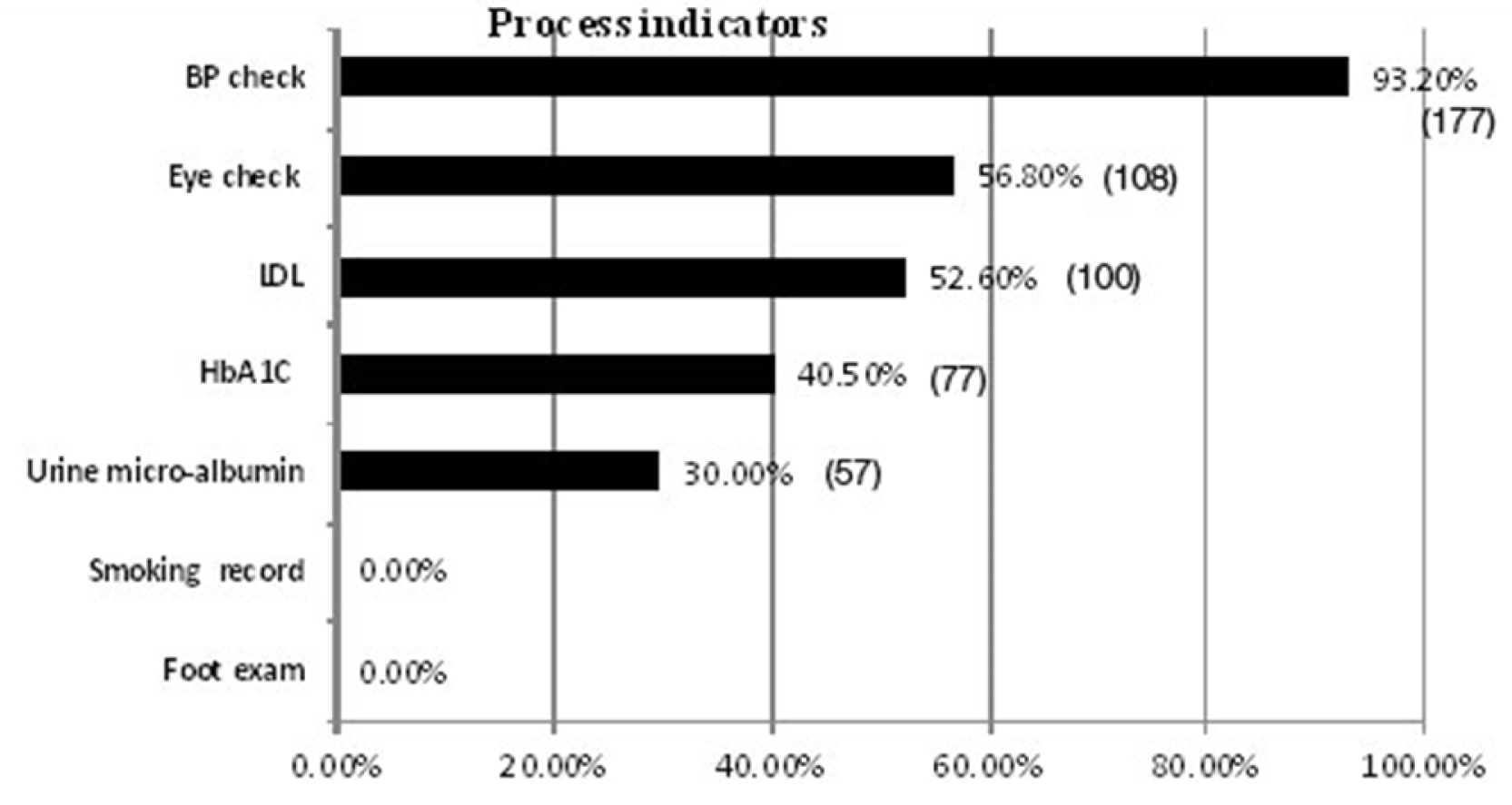
The results revealed that majority of the study population (93%) got their blood pressure examined in their last visit to the hospital. More than half of the patients received LDL cholesterol check up (52.6%) and eye check up (56.8%) whereas only less than a third received urine micro-albumin examination (30%). Annual smoking status recording (0%) and foot examination (0%) proved to be the most unpopular of the recommended guidelines [Table/Fig-2]. The average number of tests per diabetic patient was 2.7. The process indicators were not associated with age (p =0.125), gender (p = 0.58) education (p=0.473), occupation (p=0.92) or duration of diabetes (p=0.24).
Proportion of diabetics who underwent process indicator tests/examination (N=190). (The values are expressed in percentage and the number of patients is given in brackets)
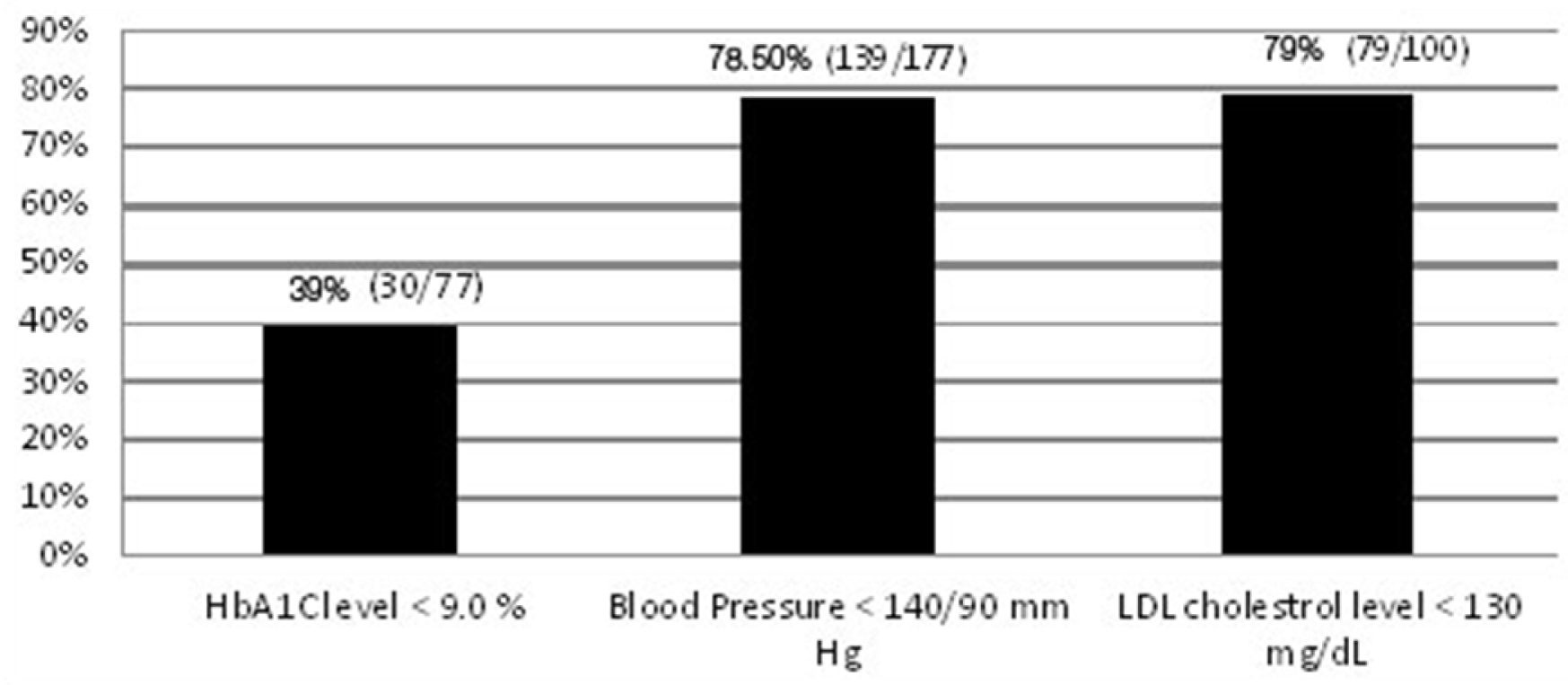
The outcome measures revealed that an alarming 61% (47/77) had a poor long term glycemic control whereas a reasonably good proportion of diabetic patients were maintaining target level blood pressure (78.5%) and LDL cholesterol levels (79%) [Table/Fig-3]. The outcome measures were not associated with age (p=0.332), gender (p=0.72) education (p=0.591) and occupation (p=0.863). The outcome indicators were better for diabetic patients with less than five years of duration (p=.02).
Proportion of diabetics with favorable proximal outcome indicators.
{Percentage (no of patients with favorable result/total number of patients who got the test done)}
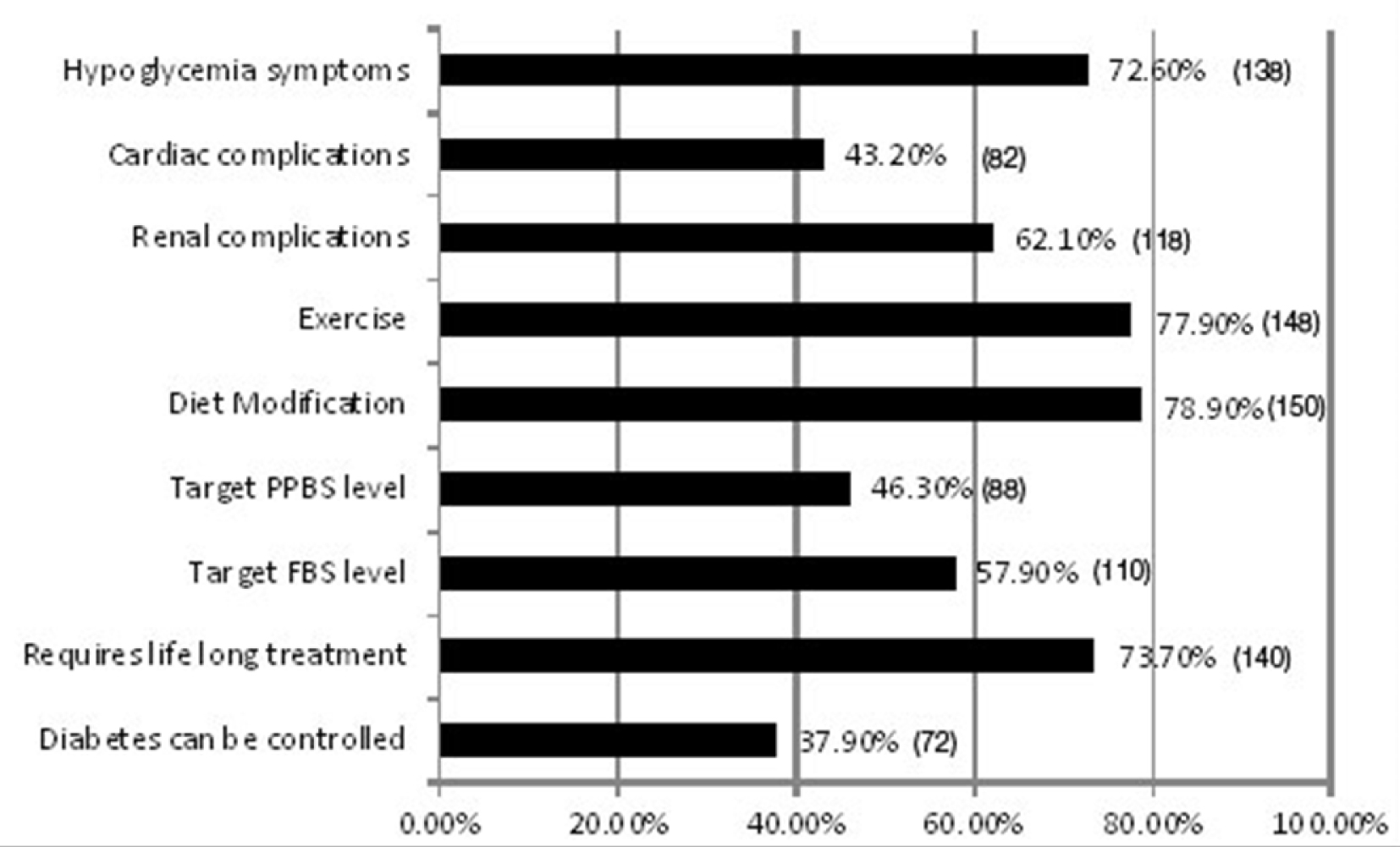
The knowledge questionnaire showed that more than 70% of the diabetic patients know that their condition requires lifelong management, the required diet modifications and the exercises that they need to do and the symptoms of hypoglycemia. The mean score was 5.4. Only 57% and 46% knew their target fasting and post prandial blood sugar respectively [Table/Fig-4]. Gender, education, occupation and duration of diabetes were associated with knowledge score [Table/Fig-5].
Proportion of patients who had adequate knowledge in essential concepts in diabetes (N=190). (The values are expressed in percentage and the number of patients is given in brackets)
Association of variables with knowledge scores
| Parameter | Category | Good score (> 7) | Average score (4-6) | Poor score (< 4) | Total | p value |
|---|
| No. | % | No. | % | No. | % | No. |
|---|
| Age | 30-60 | 44 | 38.94% | 42 | 37.17% | 27 | 23.89% | 113 | 0.221 |
| >60 | 26 | 33.77% | 38 | 49.35% | 13 | 16.88% | 77 |
| Gender | Male | 42 | 44.68% | 30 | 31.91% | 22 | 23.40% | 94 | 0.017 |
| Female | 28 | 29.17% | 50 | 52.08% | 18 | 18.75% | 96 |
| Education | Illiterate | 6 | 13.64% | 24 | 54.55% | 14 | 31.82% | 44 | 0.00 |
| 1-10 years of schooling | 8 | 16.33% | 23 | 46.94% | 18 | 36.73% | 49 |
| PUC | 33 | 48.53% | 27 | 39.71% | 8 | 11.76% | 68 |
| Graduation | 23 | 79.31% | 6 | 20.69% | 0 | 0.00% | 29 |
| Occupation | Professional | 20 | 42.55% | 17 | 36.17% | 10 | 21.28% | 47 |
| Clerical | 23 | 67.65% | 10 | 29.41% | 1 | 2.94% | 34 | 0.00 |
| Agriculture | 7 | 18.42% | 19 | 50.00% | 12 | 31.58% | 38 |
| None | 20 | 28.17% | 34 | 47.89% | 17 | 23.94% | 71 |
| Duration of diabetes | <5 years | 30 | 27.78% | 44 | 40.74% | 34 | 31.48% | 108 |
| 5 - 10years | 29 | 56.86% | 17 | 33.34% | 5 | 9.80% | 51 | 0.00 |
| >10 years | 11 | 35.48% | 19 | 61.29% | 1 | 3.23% | 31 |
| 70 | 36.84% | 80 | 42.11% | 40 | 21.05% | 190 |
The mean knowledge scores were compared among people who had better process indicator and outcome indicators to others who had poor process and using ANOVA. The analysis revealed that there was no association between knowledge scores with process indicators and outcome indicators [Table/Fig-6].
Association of knowledge scores with process and outcome indicators
| Parameter | No. of people | Mean knowledge score | Standard Deviation | F-value p-value |
|---|
| No. | % |
|---|
| Process indicator & Knowledge score |
| No tests | 7 | 3.7 | 5.9 | 2.42 | F-value: 0.033 p-value: 0.99 |
| One test | 37 | 19.5 | 6.2 | 2.31 |
| Two tests | 50 | 26.3 | 6.2 | 2.34 |
| Three tests | 35 | 18.4 | 6.1 | 2.32 |
| Four tests | 28 | 14.7 | 6.1 | 2.32 |
| Five tests | 33 | 17.4 | 6.2 | 2.30 |
| Proximal outcome indicator & Knowledge score |
| No tests | 37 | 19.5 | 5.42 | 2.31 | F-value:2.345 p-value =0.074 |
| One test | 73 | 38.4 | 5.2 | 2.307 |
| Two tests | 65 | 34.2 | 5.8 | 2.303 |
| Three tests | 15 | 7.9 | 4.13 | 2.249 |
Discussion
Even though India is regarded as the Diabetic Capital of the World and multiple players are dealing diabetes at different settings, there are not many Indian studies which have assessed the quality of diabetes care. DEDICOM study done in Delhi is the only published study which had similar objective in mind.
The results revealed that blood pressure is the only parameter which is regularly monitored in majority of the diabetics. Hb1AC, LDL cholesterol and eye check-up were done only in 40%, 52.6% and 56.8% of diabetics respectively. Less than a third received urine micro-albumin examination (30%). Only 33(17.37%) had at least 5 of the 7 essential parameters monitored at least once in the last year. This reveals that the minimum standards have to be reinforced among doctors and patients to achieve quality.
Majority of the study population (93%) got their blood pressure examined in their last visit to the hospital. This is higher compared to CODI study (54.3%) and the study conducted by Rossi et al., (77%). No separate queue, no waiting time, no extra charges, being non invasive technique, patient demand and sensitized physicians may be attributed to the popularity of this measurement.
Urine micro albuminuria is relatively unpopular even in developed countries [16,17]. The physicians prefer to send for renal function tests (Serum Creatinine) even though urine micro albuminuria is the earliest and cost effective indicator for real failure. In general it was noticed that physician show more inclination towards blood tests than urine tests.
The proportion of people getting their eye check up was comparable to the studies conducted by Suwatee et al., [6]. The initial changes in the retina usually have no bearing on vision, hence the patients often postpone their ophthalmology consultation.
Only 40.5% had their Hb1AC checked in the last year. The proportion was considerably lower than the study conducted by Rossi M et al., [17] and Suwatee et al., [6]. However, it was better than CODI [18], Duncan et al., [19] and DEDICOM study. It was observed that the doctors relied on FBS and PPBS value for dose adjustments rather than Hb1AC. Annual smoking status recording (0%) and foot examination (0%) proved to be the most unpopular of the recommended guidelines.
Another important observation of the study was, there is no association between the knowledge scores of the patients and the tests undertaken. It was assumed that better the knowledge about the disease, the better will be the process indicators. But it was seen that there was no difference in the knowledge scores between the people who had no essential tests done and those diabetics who got five essential tests done. It shows that these tests are mainly provider driven.
The current study showed that there was no association between knowledge scores and test results. There was no significant variation in knowledge scores between people whose parameters were controlled and not controlled. If practice questions would have been asked instead of knowledge questions, there could have been a difference between groups. The achievement of indicators for quality of care in the current study namely HbA1c testing, LDL cholesterol, eye check-up and BP check-up can be considered to be better than other Indian Studies. But since the DEDICOM [10] and CODI [15] studies are population based studies, better results may be expected in the present study as care may be better in tertiary hospital samples. It is evident that the process and outcome indicators show better results when compared to other studies but still we have a long way to go in filling the gaps between provision and utilization of health care facilities.
Diabetes mellitus poses a major health challenge both epidemiologically and economically in India. Today’s challenges do not arise from a lack of efficacious diabetes treatments. Rather, these challenges lie with effectively implementing them across the population. Numerous barriers to implementation are located at several levels including the societal, health care system, provider, and patient levels [20]. A quality indicator is a measurable element of practice performance for which there is evidence or consensus that it can be used to assess the quality, and hence change the quality of care provided [14]. A well planned audit conducted regularly can bring about beneficial change for patient and clinician.
Conclusion
There is a need to formulate the local standards of care and clinical practice guidelines for the management of diabetes that are easily affordable and available to the health care providers and applicable to our country at the national level. Continuing audit of patients with diabetes is a feasible and a very useful method of promoting and helping to achieve the management goals of a good quality care.
Source: National Diabetes Quality Improvement Alliance [14]