Isolated Tuberculous Peroneal Tenosynovitis: A Case Report
S.M Ajoy1, Bheemsingh Samorekar2, Sharath Soman3, Mohan Jadhav4
1Assistant Professor (Foot and Ankle Specialist), Department of Orthopaedics,M.S. Ramaiah Medical College, Bangalore, India.
2Post Graduate, Department of Orthopaedics,M.S. Ramaiah Medical College, Bangalore, India.
3Post Graduate, Department of Pathology,M.S. Ramaiah Medical College, Bangalore, India.
4Post Graduate, Department of Orthopaedics,M.S. Ramaiah Medical College, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bheemsingh Samorekar, Post graduate, Department of Orthopaedics, M.S.Ramaiah Medical College, Mattikere, Bangalore-560054, India.
E-mail: bheemsinghvs@gmail.com
Tuberculosis (TB) of osteoarticular sites constitutes less than 3% of total patients with tuberculosis. Involvement of the foot and ankle is less than 0.3% of total disease. Even in a country like India, where the incidence of TB is not uncommon, we do not encounter isolated tenosynovitis. We present a young man with bilateral tubercular peroneal tenosynovitis who was evaluated with relevant investigations and operated upon and started on antitubercular treatment (ATT) in consultation with the pulmonologist. After tenosynovectomy and commencement of ATT, the patient’s symptoms improved.
Peroneal muscles, Tenosynovectomy, Tuberculosis
Case Report
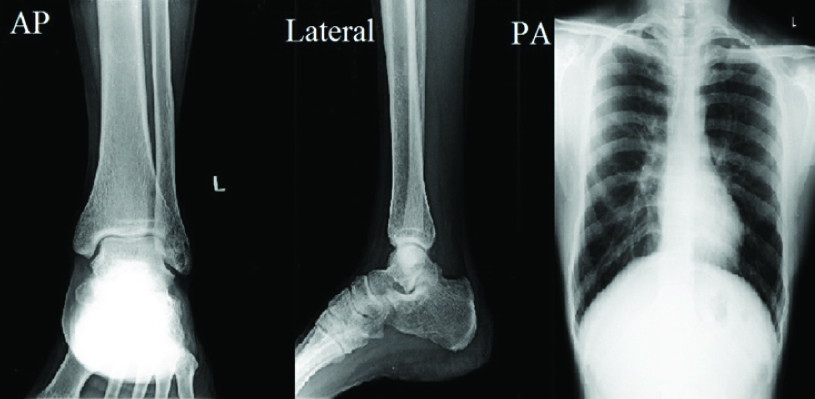
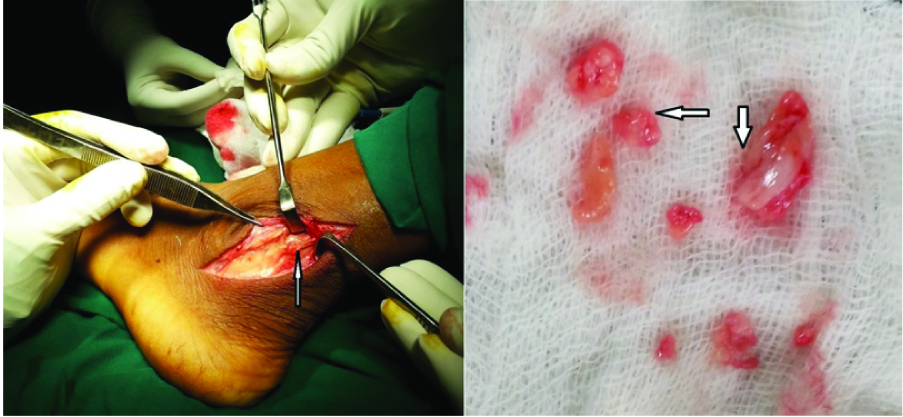
A 26-year-old young man presented to the Department of Orthopaedics with a three month history of pain in both lower legs, aggravated by walking, usually on uneven ground, dull aching type, relieved by rest and analgesics, no diurnal variation existed. It was associated with mild swelling over left ankle. No history of fever, cough, chills, early morning stiffness, trauma/sprain of ankles, other joint involvement, non hypertensive, non diabetic, no contact with TB were present. On examination of both ankles, bilateral peroneal tendons were tender with mild swelling noted posterior to lateral malleolus and left ankle comparatively more swollen [Table/Fig-1]. Tenderness aggravated on eversion of foot. General physical examination and systemic examination was normal. Chest and ankle radiographs [Table/Fig-2] were normal. Complete blood count and ESR were within normal limits. Both ankle MRI [Table/Fig-3] showed bilateral peroneal muscle tendinitis, subcutaneous oedema with soft tissue swelling around lateral malleolus. Patient was operated under spinal anaesthesia and a tourniquet at 300 mmHg pressure for 45 minutes, was applied. Diagnostic and therapeutic biopsy by tenosynovectomy [Table/Fig-4] of peroneal muscles of the left ankle was performed. Fibrosed, thickened and inflamed left peroneal tendon sheath was found during the procedure without impingement and hence only affected part was excised and sent for histopathology examination (HPE). Limb was immobilized in a posterior short leg POP slab for six weeks. Wound was found healthy at follow up. Sutures were removed on day 14 following surgery. Weight bearing commenced once patient was pain free, six weeks following the surgery. No specific physiotherapy programme was followed; patient was encouraged to mobilize the ankle and foot after POP removal.
HPE report showed granulomatous inflammation with Langhan’s giant cells and epithelioid cells favouring TB [Table/Fig-5a,b]. TB-PCR (polymerase chain reaction) was negative. Aerobic Culture showed no growth. Pulmonologist’s opinion was obtained and Anti Tuberculosis treatment as per revised National Tuberculosis Control Programme for Osteoarticular TB with isoniazid (H), rifampicin (R),
pyrazinamide (Z) and ethambutol (E) was commenced. Patient was under regular follow up with us and pulmonologist for ATT. After completing 9 months of ATT (2 months HRZE + 7months HR),
patient’s symptoms completely resolved [Table/Fig-6].
Discussion
TB of the foot and ankle accounts for Less than 10% [1,2] of osteoarticular tuberculosis, isolated TB of peroneal tendons being extremely rare and has been reported only twice in English language literature, to the best of our knowledge. Generally osteoarticular TB is associated with pulmonary TB as well. Independent occurrence is also possible, though not the norm. In a developing country like India TB is looked upon as a stigma in society. Though endemic, it’s diagnosis is a challenging job. Most common organism involved is acid fast bacilli (AFB) M tuberculosis, but due to increased HIV infection, mycobacterium avium complex (MAC) is also not uncommon [3]. There are reports of TB talus, calcaneus, talocalcaneal joint, calcaneocuboid, anterior compartment muscles of leg [4] etc. Usually pulmonary TB (PTB) is suspected by history of cough, fever more than two weeks, weight loss, loss of appetite, immunodeficiency state like chronic steroid use, immunosuppressant therapy in transplantations, HIV etc.
On clinical examination, crepitations on auscultation of chest, lymph node enlargement etc is noted. Investigations show anaemia (of chronic diseases), total white cell count is increased, lymphocytemonocyte (5:1) ratio is increased. ESR is increased [2]. CRP is increased and shows acute inflammatory disease. Sputum examination for AFB stain and culture is recommended. Chest X-ray to rule out PTB, and local site X-rays as in hip joint for classification and staging should be obtained. Mantoux test in paediatric age group is indicative of tuberculosis. Core, needle or open biopsy can be done and histopathological examination may show typical chronic granulomas, tuberculomas, caseation necrosis, epithelioid cells etc., Recent tests for Tuberculosis include TB ELISA – IgG for old healed TB and IgM for active TB, Quantiferon gold assay, TB PCR [2]. Once diagnosis of TB is made, chemotherapy is to be started with antitubercular drugs.
In India, revised national tuberculosis control programme has only two categories [5] of treatment currently: Category-1 contains all conditions other than sputum positive cases. Category-2 denotes sputum positive patients including fresh patients or relapse, defaulters, etc. Category-1 has 2 months intensive phase with isoniazid (H), rifampicin (R), pyrazinamide (Z), ethambutol (E) and 4 months continuation phase of HR. Category-2 has 2 months intensive phase with HRZES (streptomycin) +1 month HRZE and 5 months continuation phase of HRE [5].
Tenosynovectomy removes the diseased tissue along with neovascularisation. WHO 2011 survey shows annual incidence of TB in India of 2.3 million compared to 9 million global with prevalence of 3.1 million TB cases [6]. Hence, it is a prime disease of concern requiring thorough treatment both medical and surgical.
As per our literature search, isolated TB involving the peroneal muscles was reported once by Abdelwahab et al., [7] in a computer technologist born in United States. He presented with right lateral malleolus swelling without trauma. The patient’s father had chronic pulmonary tuberculosis and was from China. He was diagnosed of tuberculous peroneal tenosynovitis on MRI. More recently, KP Raju et al., reported “tuberculosis tenosynovitis of ankle with rice bodies” which was diagnosed on MRI, intraoperative findings and histopathology with no recurrence after anti-tubercular treatment on a two year follow up [8].
Swelling posterior to lateral malleolus of left foot

Radiographs of left ankle (AP, lateral) and chest (PA)
MRI- multiplanar T1W,T2W & STIR images left ankle showing subcutaneous oedema showing mild soft tissue swelling around lateral mallelous

Intra operative picture showing inflamed left peroneal sheath posterior to lateral malleolus along with the tenosynovectomy tissue sample
Histopathology showing fibrocollagenous tissue with congested blood vessels and granulomatous (A) and Langhan’s giant cells (B) inflammation with epithelioid cells

Follow up after 6 and 9 months showing decreased left ankle swelling behind lateral malleolus with healthy surgical scar

Conclusion
We recommend a differential diagnosis of TB to be kept in mind while evaluating a patient with chronic ankle pain, in a country like India where TB is not uncommon. Use of the modern investigations like CT scan, MRI, TB PCR, TB ELISA, Quantiferon gold assay along with biopsy and other serological tests when available to rule out TB whenever strong suspicions are entertained, commencing of appropriate ATT with or without surgery like synovectomy, debridement, drainage etc is recommended.
Written informed consent was obtained from patient for publication of this case report and accompanying images.
[1]. SM Tuli, Tuberculosis of the skeletal system 2010 4th EditionNew DelhiJaypee Brothers Medical Publishers:187-90. [Google Scholar]
[2]. MS Dhillon, ON Nagi, Tuberculosis of the foot and ankleClin Orthop Relat Research 2002 398:107-13. [Google Scholar]
[3]. K-i Uchiya, H Takahashi, T Nakagawa, T Yagi, M Moriyama, T Inagaki, Characterization of a novel plasmid, pMAH135, from Mycobacterium avium Subsp. hominissuisPLoS ONE. 2015;10(2):e0117797. doi:10.1371/journal.pone.0117797 [Google Scholar]
[4]. A Tavakkolizadeh, Case report tuberculous tenosynovitis of the anterior compartment of the legFoot and Ankle Surgery 2004 10(4):221-24. [Google Scholar]
[5]. http://www.tbcindia.nic.in/rntcp.html. [Google Scholar]
[6]. http://tbcindia.nic.in/pdfs/Technical%20&%20Operational%20guidelines%20for%20TB%20Control.pdf [Google Scholar]
[7]. Abdelwahab I F, Kenan S, Hermann G, Klein M J, Lewis M M, Tuberculous peroneal tenosynovitisJ Bone Joint Surg Am 1993 75(11):1687-90. [Google Scholar]
[8]. KP Raju, J Mohan Kumar, R Shetty, Tuberculous tenosynovitis of ankle with rice bodiesFoot and Ankle Online Journal 2013 6(10) [Google Scholar]