The damage or loss of anterior teeth causes a negative impact on the patient in many ways. In adolescents and young patients, the provisional replacement with artificial teeth may minimize this impact. Many approaches have been described for provisional restorations. This article discusses about a chairside fixed provisional restoration technique that was adjusted into the edentulous area of a 15-year-old girl.
Case Report
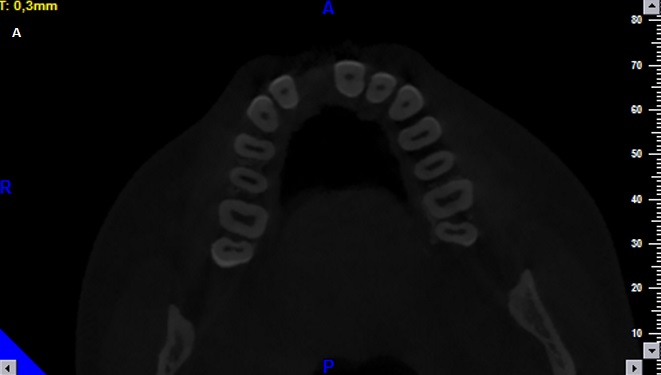
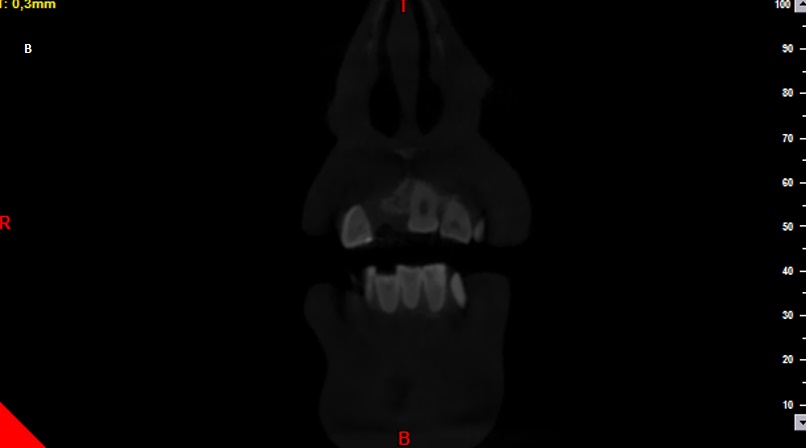
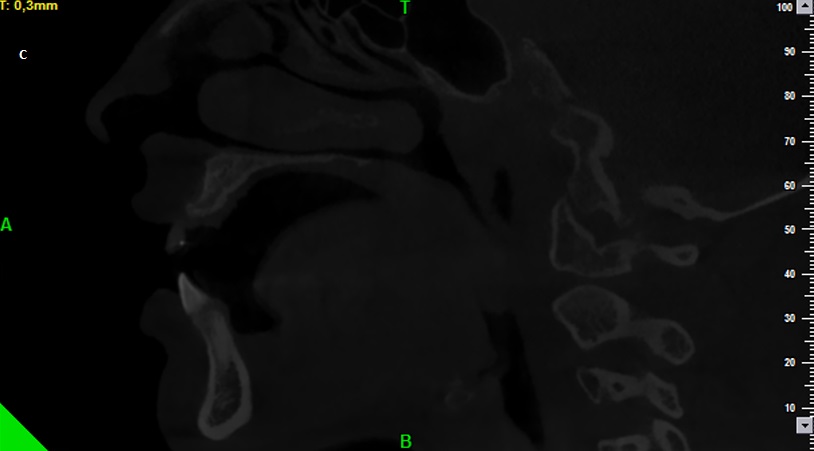
A 15-year-old female patient was referred to the Department of Prosthodontics, University of Erciyes, Faculty of Dentistry for her prosthetic rehabilitation of right upper front tooth, which was lost due to an accident that occured five months ago. Before the patient was referred to the department of prosthodontics, an implant-supported fixed prosthesis was planned in the department of oral and maxillo-facial surgery. However, because of the fact that there was no adequate bucco-lingual bone thickness, the implant placement was deferred and a bone grafting procedure was done. A bone graft was placed in order to get adequate bone volume for the placement of the implant. A CBCT was done post operatively [Table/Fig-1a,b,c].
In addition, since growth pattern of the patient was ongoing, therefore definitive implant treatment was delayed for 3years after the placement of the bone graft [Table/Fig-2].
A fixed provisional restoration was taken planned because the patient did not agree to the use of a removable apparatus as she was highly concerned about her aesthetics. Therefore, following the soft tissue healing, the fabrication of a provisional restoration for the rehabilitation of function and aesthetics was planned for the edentulous area.
An impression was made with silicone elastomeric impression material (Zetaplus, Zhermack, Italy) in order to obtain a definite cast model, and casts were poured with dental stone (GC FUJIROCK EP, Leuven, Belgium). After obtaining the cast model, a provisional fixed restoration was planned using the orthodontic lingual retainer wire (PentaOne, Masel) [Table/Fig-3] and an A2 shade-artificial acrylic denture tooth (Vita, Germany) [Table/Fig-4,5].
For this purpose, a ditch was made mesiodistally on the posterior part of the acrylic tooth[Table/Fig-6].
The orthodontic lingual retainer wire was adapted into the cavity with no chemical process, using only composite resin (ClearfilTM Majesty, Kuraray, Japan) and with mechanical retention and adjusted to the model [Table/Fig-7,8].
The restoration was then adjusted to the patient’s edentulous area. Premature contacts were eliminated and the restoration was cemented using resin cement (Panavia F, Kuraray, Japan) [Table/Fig-9,10].
The patient was followed up for a period of 3 years. Three years later, she was called to remove her provisional fixed restoration in order to provide her an implant retained permanent restoration. An implant (Dentium, Seoul, Korea) was placed into the right central incisor area. Following soft tissue healing, the colored provisional restoration was polished and re-adapted [Table/Fig-11,12].
Finally, an implant-supported permanent fixed restoration was made 6 months later and the patient was satisfied with the treatment [Table/Fig-13].
Discussion
Provisional restorations provide aesthetics, function, space maintenance, and soft-tissue healing [1]. Aesthetics is one of the most important functions of a provisional restoration, especially in the anterior region. Provisional restorations can be used to provide patient comfort and satisfaction [2] and may be produced in two parts, including fixed and removable appliances. Removable appliances are usually used in the event of tooth loss before final dentures or after implant surgery, until osseointegration has taken place. Artificial acrylic teeth are often used in partial dentures. These artificial teeth are also used as a space maintainer after early tooth loss in the pediatric dentistry setting [3]. However, in the case of a single missing tooth, patients may not agree to use a removable appliance,therefore a fixed provisional restoration can be planned.
In the current case report, a technique was applied to produce a fixed provisional restoration for a patient who had a missing tooth. At the end of the final implant-supported restoration process, the patient was satisfied. Before the implant surgery, orthodontic treatment was offered to gain equal mesio-distal distance between the cimetric central tooth and to achieve a more aesthetically pleasing outcome, however, the patient did not accept this offer.
Because of the fact that it is difficult to achieve patient satisfaction, provisional treatment is important for the dentist, especially in the anterior area [4]. Irrespective of the various treatment options available, patients reject delayed replacement and often desire provisional alternative solution in the post-extraction phase[5].
In this case report, an acyrlic tooth was used to make a provisional restoration. If the patient's own extracted tooth would have been available for use then it would have been the first choice of the dentist to be used as an option for the replacement. There are several studies in the literature about restorations that were conducted using the patient's own tooth [6,7]. Bhandari et al., reported a case that included a fixed partial denture that was obtained using multiflex orthodontic wire and the patient’s own extracted tooth that had been lost due to periodontal reasons [7]. Mengrong et al., reported a case that included a maxillary anterior tooth restoration by using a fiber-reinforced composite with a natural tooth pontic [6]. However, there are no studies that address using orthodontic multi-flex wire and an acrylic artificial tooth.
One advantage of this technique is that it is less expensive and simpler than fiber-reinforced restorations. Another advantage of this technique is that, no cavity preparation was needed on the adjacent teeth. Only etching and bonding procedures were applied to the adjacent teeth.
Ulusoy et al., reported a case report that was used a fixed provisional restoration for a patient who had lost a maxillary cental tooth because of trauma [5]. In their report, two molar bands and 0.9 mm orthodontic wire had been used, therefore their aparatus was quite voluminous. A large aparatus is not comfortable and patients may find it difficult to use. In the present case, the fixed restoration was fairly small and was quite comfortable.
On the other hand, the aparatus produced by Ulusoy et al., had more stability, due to having a large bonding area. In this case, the bonding area was smaller than Ulusoy et al., however the patient had never complains of any decementation.
Axial view of the dental tomography after applied bone graft
Coronal view of the dental tomography after applied bone graft
Sagittal view of the dental tomography after applied bone graft
View of the edentulous area after applied bone graft

View of the multiflex orthodontic wire
Buccal view of the artificial acrylic denture tooth

Palatinal view of the artificial acrylic denture tooth

View of the cavity along the mesio-distal strike

View of wire adjusted to the cast model

View of the artificial acrylic denture tooth adjusted to the cast model

Final provisional restoration

The incisal view of the provisional restoration

Radiographic view of the implant after healing

Re-adapted provisional restoration

Clinical view of the final implant-supported restoration

Conclusion
It is important to select the type of provisional restoration in order to achieve anterior aesthetic. Because aesthetic outcomes are affected by the type of provisional restorations and it can be challenging for a clinician. This case report described a technique for producing an aesthetic provisional restoration. The patient did not want a removable aparatus. Due to its several advantages, a fixed provisional restoration was fabricated for the patient. This technique can be an alternative solution to produce an anterior fixed provisional restoration.
[1]. AS Bidra, A Manzotti, A direct technique for fabricating esthetic anterior fixed provisional restorations using polycarbonate veneersCompend Contin Educ Dent. 2012 33:452-56. [Google Scholar]
[2]. YS Al Jabbari, A Al-Rasheed, JW Smith, AM Jacopino, An indirect technique for assuring simplicity and marginal integrity of provisional restorations during full mouth rehabilitationSaudi Dent J 2013 25:39-42. [Google Scholar]
[3]. P Chalakkal, RS Devi, GV Srinivas, P Venkataramana, Dentulous appliance for upper anterior edentulous span.J Clin Diagn Res 2013 7:3086-87. [Google Scholar]
[4]. PS Fu, YM Wu, CF Tsai, TK Huang, WC Chen, CC Hung, Immediate provisional restoration of a single-tooth implant in the esthetic zone: a case reportKaohsiung J Med Sci. 2011 27:80-84. [Google Scholar]
[5]. AT Ulusoy, ZC Cehreli, Provisional use of a natural tooth crown following failure of replantation: a case reportDent Traumatol 2008 24:96-99. [Google Scholar]
[6]. XU Mengrong, Q Zhang, H Qiu, Maxillary anterior tooth restoration by using fiber-reinforced composite with a natural tooth pontic: a case reportHua Xi Kou Qiang Yi Xue Za Zhi 2013 31:638-40. [Google Scholar]
[7]. S Bhandari, R Chaturvedi, Immediate natural tooth pontic: a viable yet temporary prosthetic solution: a patient reported outcomeIndian J Dent Res 2012 23:59-63. [Google Scholar]