A Rare Case of Urachal Sinus
Sunkeswari Sreepadma1, Barkur Raghavendra Chaithra Rao2, Jaideep Ratkal3, Veena Kulkarni4, Rajeev Joshi5
1Assistant Professor, Department of Anatomy, SDM College of Medical Sciences and Hospital, Dharwad, Karnataka, India.
2Assistant Professor, Department of Anatomy, Sapthagiri Institute of Medical Sciences, Bangalore, Karnataka, India.
3Consultant Surgeon, Lifeline Hospital, Hubli, Karnataka, India.
4Professor, Department of Anatomy, SDM College of Medical Sciences and Hospital, Dharwad, Karnataka, India.
5Consultant Physician, Lifeline Hospital, Hubli, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sunkeswari Sreepadma, Assistant Professor, Department of Anatomy, SDM College of Medical Sciences and Hospital, Dharwad, Karnataka-580009, India.
E-mail: sreepadma@gmail.com
Abnormalities in the closure of the intraembryonic portion of the allatoic lumen result in urachal abnormalities. Urachal remnant diseases are rare in adults. Malignant urachal neoplasms, like adenocarcinoma which may probably occur due to metaplasia of the transitional epithelium of the urachal remnant are very rare. Surgical excision of the urachus is needed. The imaging features of the urachal abnormalities are important for correct diagnosis and surgical management.
Allantois, Umbilicus, Urachus
Case Report
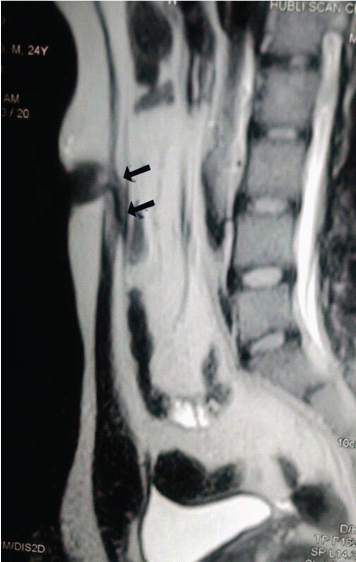
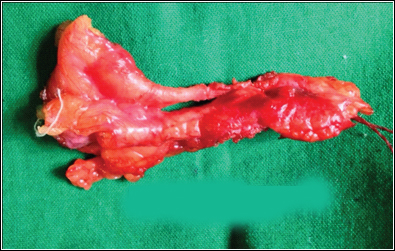
A 24-year old male, came to the Urology department, Lifeline hospital, with history of discharge from the umbilicus. On examination, it was detected as infected remant of urachus. Routine investigations were done. USG reported as ill defined hypoechoic tender tubular lesion underneath parietal wall in the midline infraumbilical region, suggestive of urachal sinus. MRI reported as findings of Urachal sinus extending for a distance of approximately 2.5 cm. A hypotense tract with narrow fluid filled lumen was extending from the umbilicus inferiorly for 2.5 cm approximately in length, beneath the anterior abdominal wall [Table/Fig-1] . No evidence of collection beneath the umbilicus. Urinary bladder had normal thickness. The patient was treated with antibiotics, and surgical excision [Table/Fig-2] of the urachus was done, and during the surgery, cystoscopy was also done. The physician examined for malignancy and found none. Histopathological report indicates chronic inflammatory disease. He was discharged with medications and was advised to do follow up. The patient had come for follow up after 2 weeks, then 4 weeks and then after 3 months and 6 months. He was examined and found no recurrence of the condition.
Discussion
The urachus is a tubular, midline structure, located preperitoneal in the centre of a pyramidal shaped space, lined by obliterated umbilical arteries with its base on the dome on the anterior bladder and the tip directed towards the umbilicus. The urachal length varies from 3 to 10 cm [1]. Urachus or median umbilical ligament is a remant of cloaca, which is the cephalic extension of urogenital sinus and the allantois, which is a derivative of the yolk sac [2]. In late embryonic and fetal life and early postnatal life, the urachal portion, which is microscopic, fails to grow; thus, its lumen narrow and is usually obliterated by fibrous proliferation. The urachus involutes normally before birth and persists as a fibrous band [3]. Congenital urachal anomalies are twice as common in men as in women [4]. In, umbilical-urachal sinus, the urachus obliterates at the bladder level but remains open at the umbilicus.
Umbilical-urachal sinus consists of blind dilatation of the urachus at the umbilical end. A small opening into the umbilicus is generally present and may result in periodic discharge [5,6]. A thickened tubular structure along the midline below the umbilicus can be visualized at USG. There are four types of congenital urachal anomalies [7]: 1) Patent urachus; 2) Urachal cyst; 3) Umbilical-urachal sinus and; 4) Vesicourachal diverticulum. A patent urachus is purely congenital and accounts for about 50% of all cases of congenital anomalies. An urachal cyst (30%), umbilical-urachal sinus (15%), vesicourachal diverticulum (3 % to 5%), may close normally after birth but then reopen in association with pathologic conditions that are often categorized as acquired diseases. The route of infection may be lymphatic, haematogenous, or vesical, and a wide variety of gram-positive and gram-negative micro-organisms have been cultured from infected urachal remnants [3].
Urachal abnormalities result from incomplete regression of the fetal urachus. If the allantois remains patent and urine appears through umbilicus, it is patent urachus. If the proximal and distal parts of allantois are obliterated and only the middle part is patent, it is urachal cyst. When the allantois is patent only at the umbilical end, rest of the part is fibrosed then it is urachal sinus. If the allantois is forming a small diverticulum at the vesical end, it forms vesicourachal diverticulum. In vesicourachal diverticulum, the urachus communicates only with the bladder dome.
Urachus is surrounded by the umbilicovesical fascia, disease process usually remain contained inside the pyramidal space. The urachus can remain completely open or obliterate partially, leading to the formation of cystic structures throughout its course. Ashey et al., reported amongst 176 patients diagnosed with urachal anomaly, and urachal remnants were found in 46 children and 130 adults. Surgical treatment in children consisted of simple excision, whereas more than 50% adults required radical or partial cystectomy due to malignancy. There was no reported evidence that a persistence urachal remnant would lead to cancer development in later life [8]. Galati et al., reported in 23 children with urachal remnants, 10 of whom underwent excision due to symptomatic problems. They found that spontaneous resolution with non-operative management is likely with remnants in patients younger than 6 months [9]. The characteristics of the drainage fluid are a clue to its cause. Persistent clear fluid leakage (likely urine) in an infant is highly suggestive of a patent urachus while cloudy, serous, or bloody fluid is more indicative of an urachal sinus or cyst. The differential diagnosis of umbilical drainage also includes omphalitis, omphalomesenteric duct remnant, or an umbilical granuloma [10]. During routine radiographic evaluation for the other diseases of urinary system, urachal anomalies can be incidentally found. Excision of the urachal remnant is curative. The main surgical dilemma occurs in patients who present with an asymptomatic lesion that is incidentally discovered in imaging. Pathological analysis of excised urachal remnants showed persistent epithelium in the remnant [11].
MRI Showing remnant urachus. Arrows Pointing at the Urachal sinus
Surgically excised urachus
Conclusion
Urachal sinus is a blind dilatation of urachus at the umbilical end and is subject to infection. The accurate diagnosis can be done by USG, CT, VCUG and MRI. Urachal tumours are very rare. Histological sections of remnant urachus show non-regressing epithelium. The transformation remnant epithelium into a malignancy is unknown. The anatomy and imaging of these urachal diseases is essential for proper diagnosis and interventions. Such rare urachal remnant anomalies knowledge is essential for surgeons and urologists.
[1]. DC Frimberger, BP Kropp, Bladder anomalies in children.In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-Walsh Urology 2012 10th EditionPhiladelphiSaunders;:3381-85. [Google Scholar]
[2]. KL Moore, Edwin Jr, The urogenital system. In: Moore KL, eds. The developing human 1982 17th EditionPhiladelphiaSaunders,:255-97. [Google Scholar]
[3]. JS Yu, KW Kim, HJ Lee, YJ Lee, CS Yoon, MJ Kim, Urachal remnant diseases: spectrum of CT and US findings.Radio Graphics 2001 21(2):451-61. [Google Scholar]
[4]. GW Friedland, PA Devries, NM Matilde, R Cohen, MD Rifkin, Congenital anomalies of the urinary tract. In: Pollack HM, ed. Clinical urography 1990 PhiladelphiaSaunders,:559-787. [Google Scholar]
[5]. SM Berman, BM Tolia, E Laor, RE Reid, SP Schweizerhof, SZ Freed, Urachal remnants in adults.Urology. 1988 31(8):17-21. [Google Scholar]
[6]. M Blichert-Toft, OV Nielsen, A congenital patent urachus and acquired variantsActa Chir Scand 1971 137:807-14. [Google Scholar]
[7]. M Blichert-Toft, F Koch, OV Nielsen, Anatomic variants of the urachus related toclinical appearance and surgical treatment of urachal lesionsSurg Gynecol Obstet 1973 137:51-54. [Google Scholar]
[8]. RA Ashey, BA Inman, JC Routh, Urachal anomalies: a longitudinal study of urachal remnants in children and adults.J Urol 2007 178:1615-18. [Google Scholar]
[9]. VG Galati, B Donovan, F Ramji, Management of urachal remnants in early childhoodJ Urol 2008 180:1824-27. [Google Scholar]
[10]. BG Cilento, SB Bauer, AB Retik, Urachal anomalies: defining the best diagnostic modality.Urol. 1998 52:120-22. [Google Scholar]
[11]. HL Copp, IY Wong, C Krishnan, S Malhotra, WA Kennedy, Clinical presentation and urachal remnant pathology: implications for treatment.J Urol 2009 182:1921-24. [Google Scholar]