Intra Oral Fibrosarcoma with Various Histopathological Patterns: A Rare Case Report
A. Vikram Simha Reddy1, A. Ravi Prakash2, V. Sai Ram3, K.L Keerthana4, Rukmini Swathi Thorati5
1Reader, Department of Oral and Maxillofacial Pathology, G.Pulla Reddy Dental College, Nandyal Road, Kurnool, India.
2Professor and HOD, Department of Oral Pathology, G.Pulla Reddy Dental College, Nandyal Road, Kurnool, India.
3Professor and HOD, Department of Oral Medicine & Radiology, G.Pulla Reddy Dental College, Nandyal Road, Kurnool, India.
4Post Graduate Student, Department of Oral and Maxillofacial Pathology, G.Pulla Reddy Dental College, Nandyal Road, Kurnool, India.
5Post Graduate Student, Department of Oral and Maxillofacial Pathology, G.Pulla Reddy Dental College, Nandyal Road, Kurnool, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. K.L. Keerthana, Post Graduate Student, Department of Oral Pathology, G. Pulla Reddy Dental College, Nandyal Road, Kurnool-518007, India.
E-mail: Kheer9@gmail.com
Fibrosarcoma has been defined as a malignant mesenchymal tumour, the cells of which recapitulate the appearance of the normal fibroblast, with variable collagen production. Fibrosarcoma is a very uncommon tumour in the head and neck regions constituting only 0.05% of all the fibrosarcomas presenting in humans. They cause no characteristic symptoms and pose difficulty in clinical diagnosis. They have been classified histologically based on their distinct features into myxoid fibrosarcoma, low grade fibromyxoid fibrosarcoma and sclerosing epitheloid sarcoma. Here we present a rare case report of a 45-year-old male patient presenting with a maxillary fibrosarcoma, which histologically presented with different patterns.
Fibroblasts, Oral cavity, Sarcoma
Case Report
A 45-year-old male patient referred to the outpatient department of our college with a chief complaint of pain and swelling in the upper front tooth region. Initially it was slow growing and reached the size of 4 x 3 cm in a duration of 2 months.
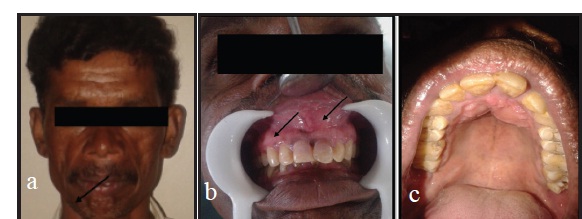
Extra oral examination revealed diffuse swelling present in the anterior surface of the face extending between the alae of the nose crossing the midline, with no secondary changes over the overlying skin [Table/Fig-1a]. On palpation the swelling was tender. Regional lymph nodes were non palpable.
Intra oral examination revealed a solitary, sessile, nodular, pale coloured growth of the maxillary anterior region extending between the right and left maxillary lateral incisors, crossing the midline both on the labial and the palatal side [Table/Fig-1b,c]. The swelling measured about 4x3 cm. approximately. On palpation it was firm and tender. Grade I mobility of 11,12, 21, 22 was observed which were tender on percussion. On radiographic examination a periapical radiolucency involving the apices of 11, 12, 21, 22 measuring about 4 x 3 cm approximately was observed.
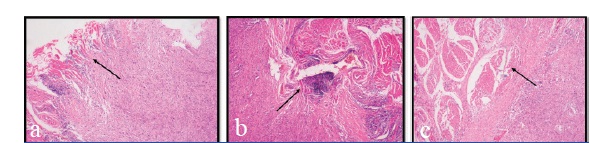
An incisional biopsy was performed in relation to 21, 22 on the labial aspect. The haematoxylin and eosin stained sections showed bizarre looking tumour cells in a connective tissue stroma. The tumour cells were spindle shaped with elongated hyperchromatic nuclei arranged irregularly and infiltrating into the skeletal muscle [Table/Fig-a-c]. These cells were arranged in bundles and fascicles. Few mitotic figures were also seen. The stroma showed myxoid appearance in few areas, with rosette arrangement of the tumour cells, along with highly fibrous areas. Alternative areas of fibrous and myxoid areas were also apparent. Herring bone pattern was also evident at few areas. A primary diagnosis of spindle cell tumour was given Immunohistochemical analysis was done for a definitive diagnosis. The cells showed positive immunoreactivity for vimentin, SMA and 30-40% positivity for mi b-1, whereas they showed negativity for desmin, S-100, CD34.
Based on the clinical, histopathological and immunohistochemical analysis the final diagnosis of low grade fibrosarcoma was given.
Discussion
Fibrosarcoma is a malignant neoplasm arising from the fibroblasts of the connective tissue. This is a common neoplasm of the bone and it is also found in soft tissues. This tumour is usually seen in the 3rd to 5th decades of life with a slight male predilection. When it occurs in the oral cavity, it is usually seen in the mandible rather than in the maxilla [1].
Histologically Fibrosarcoma (FS) can be classified into 3 variants (i) Myxoid fibrosarcoma (myxofibrosarcoma); (ii) low grade fibrom- yxoid sarcoma/ hyalinizing spindle cell tumour with giant cell rosettes; and (iii) Sclerosing epitheloid fibrosarcoma [1]. Myxoid fibrosarcoma is a multinodular tumour of low cellularity with the spindle cells arranged in a prominent myxoid matrix. The spindle cells show mild pleomorphism with rare mitotic figures. Fibromyxoidsarcoma shows low or moderate cellularity composed of bland spindle shaped cells with mild pleomorphism and little mitotic activity. The cells are deposited in a variably fibroid and myxoid stroma that tends to alternate in different areas of the tumour. The fibromyxoid type with giant rosettes shows the presence of rosettes that merge imperceptibly with the surrounding hyalinized or spindled stroma [1]. The rosettes are composed of central collagen fibres, surrounded by rounded to oval cells. Sclerosing epitheloid fibrosarcoma shows cytologicaly bland epitheloid cells deposited in a densely hyalinized collagenous matrix. The stroma is composed predominantly of densely arranged deeply acidophillic collagen which sometimes may completely obliterate the neoplastic cells [1].
The histologic grading of FS is mainly based on the degree of cellularity, degree of cellular differentiation, number of mitotic figures, amount of collagen produced by the tumour cells and extent of necrosis into well differentiated and poorly differentiated FS. Well differentiated fibrosarcomas are characterized by a uniform, orderly appearance of the spindle cells, oriented interlacing fascicles, forming a classic herring bone pattern. In others a hyalinized stroma may also be present. Poorly differentiated FS are characterized by closely packed, less well oriented tumour cells with numerous mitotic figures, areas of necrosis. The herring bone pattern is less distinct [1].
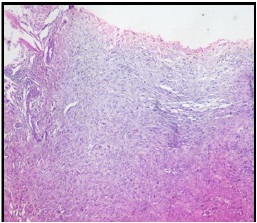
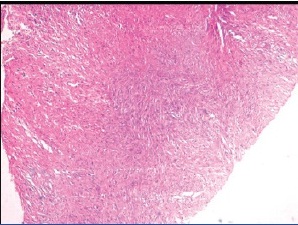
In our present report, the patient showed myxoid areas with low cellularity in a hyalinized stroma in few areas representing the myxoid fibrosarcoma[Table/Fig-3]. Few areas also showed the alternating fibroid and myxoid areas[Table/Fig-4]along with giant rosettes seen in fibromyxoid sarcoma. At focal areas the neoplastic epitheloid cells between the dense collagen fibres resembling Sclerosing epitheloid fibrosarcoma were also seen [Table/Fig-5]. Along with these features, the classic herring bone pattern was also evident [Table/Fig-6]. Therefore all the different variants of FS were evident in this case, resembling a hybrid variant of FS.
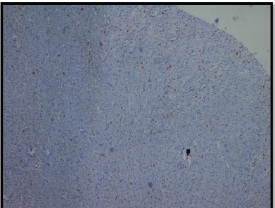
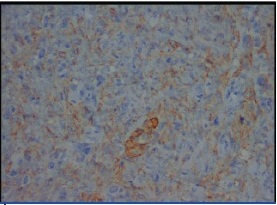
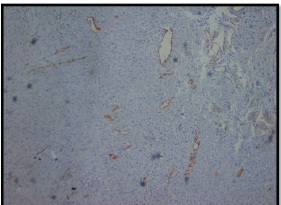
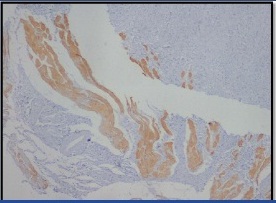
Masson’s Trichrome special stain also demonstrated the positive staining of collagen rosettes [Table/Fig-7]. Immunohistochemical analysis was made using a panel of markers which included Vimentin- a mesenchymal marker, MIB-1 which is useful in determining the proliferative index. S-100 – a protein distributed widely in the peripheral and central nervous system CD-34 – an endothelial and vascular marker, Cytokeratin – an epithelial marker, Desmin and SMA–muscle markers. The sections showed strong positivity for Vimentin [Table/Fig-8] and focal positive staining for MIB-1 [Table/Fig-9]. SMA positivity was also seen representing the myofibroblastic differentiation of the neoplastic spindle cells seen in Low Grade Fibromyxoid type [Table/Fig-10] [1]. It stained negative for all other markers including S-100, CD-34[Table/Fig-11], Desmin [Table/Fig-12].
Based on the clinical, epidemiological, microscopic and immunohistochemical analysis, a diagnosis of Intra oral Fibrosarcoma representing a hybrid variant was given.
The treatment of choice is surgical excision with a wide margin [2,3]. The need for adjuvant radiotherapy or chemotherapy is still controversial and usually indicated in high grade tumours that may present with metastases. Our patient was treated with a surgical excision followed by chemotherapy. Unfortunately, the patient expired due to recurrence 6 months after surgery.
The prognosis of FS is influenced by multiple factors like the site of origin (bone or soft tissue), age and systemic health of the patient, and the histological appearance of the tumour. Peripheral fibrosarcomas like in the oral cavity enjoyed a more favourable 5-year survival rate of 69% than did central fibrosarcoma 27% [4].The prognostic factors include a high grade of differentiation, absence of local recurrences with an overall survival rate of 21.8% to 83% in 10 years [5,6].
(a) Extraoral view of the patient with a swelling of the maxilla crossing the midline. There are no secondary changes on the overlying skin. (b&c) Solitary, sessile, nodular, pale coloured growth of the maxillary anterior region extending between the right and left maxillary lateral incisors, crossing the midline both on the labial and the palatal side
(a) Arrow shows the tumour cells infiltrating into the surrounding skeletal muscle. (b) Arrow shows the spindle shaped tumour cells encircling and infiltrating the skeletal muscle bundles. (c) The tumour cells arranged irregularly and encircling the skeletal muscle bundles
Myxoidfibrosarcoma showing the minimally pleomorphic cells separated by copious amounts of myxoid stroma
Alternative areas of myxoid and fibroid areas in the stroma with herring bone pattern
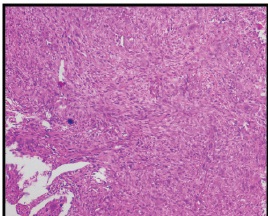
Sclerosing Epitheloid fibrosarcoma characterised by abundant hyalinized collagen fibres with small rounded tumour cells
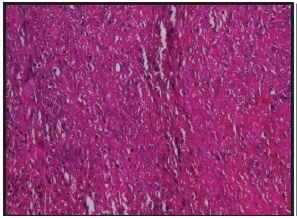
Herring bone pattern of arrangement of the spindle cells in fascicles
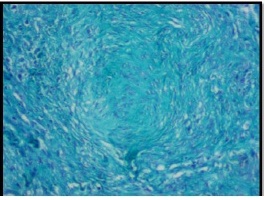
MassonsTrichrome staining of collagen rosette demonstrating the central portion of collagen with tumour cells
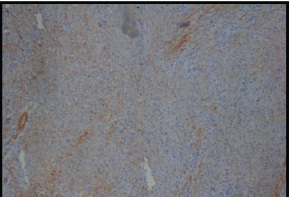
Strong positive staining for Vimentin
Focal positive staining for MIB-1
SMA positivity is seen as focal areas representing the myofibroblastic differentiation of the cells
Negative staining of CD34 which is a vascular marker
Negative staining of the fibroblasts for desmin. Only the muscle fibres show positives staining for desmin (4 X magnification)
Conclusion
Fibrosarcoma which usually presents in the long bones of the body is a rare tumour in the oral cavity. When FS is suspected, it should be differentiated from other tumours in the oral cavity. Immunohistochemical analysis using a panel of markers should be done and after diagnosis a proper follow up of the patient is essential as this tumour possess high recurrence and poor survival rates.
[1]. FM Enzinger, SW Weiss, Fibrosarcoma 1990 2nd EditionNew DelhiThe C V Mosby Company; B I publications Pvt Ltd:409--44. [Google Scholar]
[2]. AD Rapidis, H Gakiopoulou, SD Stavrianos, GA Vilos, G Faratzis, EE Douzinas, Sarcomas of the head and neck. Results from the treatment of 25 patientsEur J Surg Oncol 2005 31(2):177-82. [Google Scholar]
[3]. PK Pellitteri, A Ferlito, PJ Bradley, AR Shaha, A Rinaldo, Management of sarcomas of the head and neck in adultsOral Oncol 2003 39:2-12. [Google Scholar]
[4]. LR Eversole, WD Schwartz, WR Sabes, Central and peripheral fibrogenic and neurogenic sarcoma in the oral regions.Oral Surgery Oral Medicine Oral Pathology 1973 36:49-61. [Google Scholar]
[5]. F Bertoni, R Capanna, P Calderoni, Primary central (medullary) fibrosarcoma of bone,Semin Diagn Pathol 1984 1:185-98. [Google Scholar]
[6]. JC atsakis, DH Rice, DR Howard, The pathology of head and neck tumours: spindle cell lesions (sarcomatoid carcinomas, nodular fasciitis, and fibrosarcoma) of the aereo digestive tracts. Part 14Head Neck Surg 1982 4:499-513. [Google Scholar]