A Precise Method of Measuring Simultaneous Intrusion and Uprighting of Mandibular Molar Using Denta Scan – A Case Report
Biswas Palukunnu Padmaprabha1, Shaji Aboobacker Ponnambathayil2, Hariprasad Aynipully3, Midhun Vinod4, Deepak Parambath Reghunathan5
1Professor and Head, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
2Reader, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
3Reader, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
4Post Graduate Student, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
5Post Graduate Student, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Midhun Vinod, Sneha (H), Sivapuram (P.O), Mattannur, Kannur, Kerala- 670702, India.
E-mail: midhun.vinod@gmail.com
A commonly encountered problem in prosthetic dentistry is the supra eruption of teeth due to absence of opposing teeth. Consequently, replacement of the missing teeth with prosthesis becomes difficult due to lack of vertical dimension of the edentulous area. This article describes the space regaining procedure in a 14-year-old female patient who wanted a fixed prosthesis for her missing maxillary 1st molar. On examination, it was observed that mandibular 1st molar had supraerupted and tipped lingually. After considering the various treatment modalities it was decided to simultaneously intrude and upright the mandibular molar using a mini-implant. The precise measurements of intrusion and uprighting were done using Dentascan software. Intrusion of 1.8mm and buccolingual uprighting of 2.3mm was achieved in 45 days. The mini-implant is an efficient non-compliance device to intrude and upright the tooth simultaneously. Dentascan is an accurate and very precise method of measuring the intrusion and uprighting of teeth.
Buccolingual, Elastomeric, Mini-implants, Models, Self drilling
Case Report
A 14-year-old female patient reported to the Department of Prosthodontics for the replacement of missing right upper back tooth which was extracted three years back due to dental caries. On intra oral examination it was observed that maxillary right first molar was missing and there was a good amount of supraeruption associated with lingual crown tipping of the opposing mandibular 1st molar [Table/Fig-1]. As the space for the prosthesis was found to be insufficient due to the supraeruption of the opposing lower molar, the case was referred to the department of orthodontics for intrusion and uprighting of the supraerupted tooth.
Treatment options
Orthodontically it could be intruded by sectional mechanics [1], trans-palatal arch [2] and magnets [3] other than using microimplants. An example for sectional mechanics is the rapid molar intruder [4] which uses the force module like that of jasper jumper with vertical forces directed towards the upper and lower molars for intrusion. The reciprocal intrusion of the opposite molar is a disadvantage in this appliance. In this particular situation, apart from true intrusion, the lower molars also required buccolingual uprighting which most appliances mentioned above were incapable.
Treatment
Rubber base impressions were made of upper and lower arches and study models in dental stone were obtained. The study models were then scanned with Dentascan software and measurements recorded. After discussing various treatment options, taking into consideration the esthetics, treatment duration, patient comfort and biomechanics it was decided to treat the case with Temporary skeletal anchorage devices (TSADs) against a full strap up with fixed mechanotherapy.
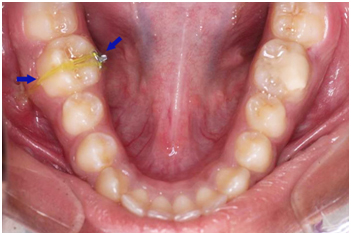
After due consent was taken from the patient, a Tomas mini-implant (Dentaurum, Germany) of 1.2 mm diameter and 6 mm in length was placed in the inter radicular region of lower right 1st molar under local anesthesia with a self drilling method and a lingual attachment was also given for the same tooth. An elastomeric chain was placed from the lingual attachment to the mini-implant with a force value of 300gm [Table/Fig-2] which was changed every two weeks. The total time taken to complete the study was 45 days.
Evaluation of treatment changes
The results were evaluated using a unique and precise method wherein the pre treatment and post treatment study models were taken and converted into three dimensional digital models using Dentascan software. On these digital models certain reference points and lines were drawn and measurements were done to obtain precise results using the software.
Results
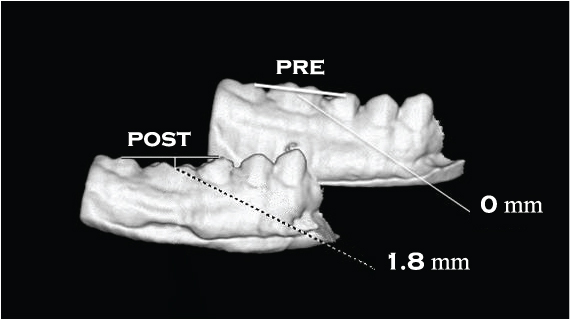
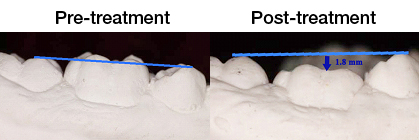
To estimate the amount of intrusion a reference line was drawn by joining the mesiobuccal cusp tip of 2nd molar with the buccal cusp tip of 2nd premolar. The deepest point on the occlusal surface was taken as reference for measuring the amount of intrusion. In pre treatment digital models the reference point was coinciding with the reference line. Post intrusion, the reference point was situated 1.8mm below the reference line, indicating an intrusion of 1.8 mm [Table/Fig-3,4].
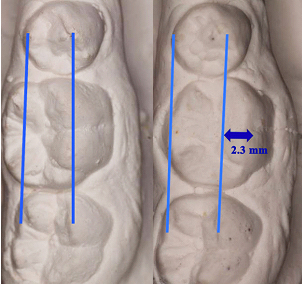
For evaluating the bucco lingual uprighting two parallel lines were drawn on the pre and post treatment digital models using the Dentascan software, first was a lingual line and other was buccal. The lingual line was drawn connecting the mesio lingual cusp tip of 2nd molar with the lingual cusp tip of 2nd premolar. The buccal line was drawn joining the mesio buccal cusp tip of 2nd molar and the buccal cusp tip of 2nd premolar. In the pretreatment model, the lingual line was 2.2mm away from the most lingual point on the occlusal surface of the mandibular 1st molar, whereas the buccal line was corresponding to the buccal surface of the same tooth. In the post treatment model the lingual line was found to be corresponding to the lingual surface of 1st molar and the buccal surface was 2.3mm away from the buccal line from of the occlusal aspect, indicating that the tooth had moved 2.3mm buccally [Table/Fig-5,6]. Thus, a simultaneous intrusion of 1.8 mm and buccolingual uprighting of 2.3mm in 45 days was achieved [Table/Fig-7]. The patient was then referred to the department of Prosthodontics for replacement of the missing maxillary first molar.
Discussion
Most force systems commonly used for intrusion of a single molar will have reciprocal force effects on adjacent teeth and thus makes the system biomechanically unstable. However, these drawbacks could be overcome by using Temporary skeletal anchorage devices (TSADs). Stationary anchorage is achieved by gripping mechanically to cortical bone rather than by osseointegration [4].
Not many studies have been carried out to achieve simultaneous bucco-lingual uprighting and intrusion of the mandibular molar using a mini-implant. Also, in this study a unique 3 dimensional method of measuring the precise intrusion and uprighting has been performed using the Dentascan software. In the present study the amount of true intrusion achieved in 45 days was 1.8 mm. Kartik and Shweta used an “I” shaped miniplate to intrude the mandibular molars [5]. In three months they were able to achieve a maximum intrusion of 2.5mm but it involved an invasive procedure of placing a miniplate when compared to mini-implant placement. As they used OPG to check the amount of intrusion, there would be an accompanied error of magnification and thus the accuracy of measurement was questionable. Whereas, in the present study, actual study models were scanned and compared therefore the measurements were accurate without error in three dimensions of space. Nicolaievsky used miniplates in the maxillary arch and reported an intrusion of 0.75mm per month [6]. In studies related to maxillary molar intrusion [4,7] using mini-implant, the amount of intrusion achieved per month was 0.5 to 1mm and the maximum amount of intrusion achieved was 4.4mm in 6 months [7]. Chung-Chen Jane Yao et al., [8] used a combination of miniplate and mini-implant to intrude the maxillary molars and achieved intrusion of 4mm in 7 months.
Studies using radiographic methods [5,7] for evaluating the amount of intrusion had inborn error of magnification which lead to inaccurate measurements. Chung-Chen Jane Yao et al., [8] used 3-D digitizer to estimate the amount of intrusion, the results were found out to be more accurate without any magnification error. This method was almost similar to our study as they also analysed the intrusion three dimensionally. The present study generated the models using CT scan while the latter used a manual digitizer machine whose accuracy is dependent on the operator’s skill. To add, none of these methods evaluated the bucco lingual uprighting like the dentascan models did, wherein a total 2.3mm of movement was achieved. The elastic force produced a moment with respect to the centre of resistance of mandibular first molar tooth which provided the simultaneous uprighting and intrusion effect on the tooth. This was a unique advantage of this precise 3 dimensional method.
Supraeruption associated with lingual crown tipping of mandibular 1st molar causing displacement with reduced vertical clearance

Elastomeric chain from the lingual attachment to the mini-implant
Denta scan showing molar intrusion by 1.8 mm
Models showing molar intrusion by 1.8 mm
Dentascan showing buccolingual uprighting of molar by 2.3 mm
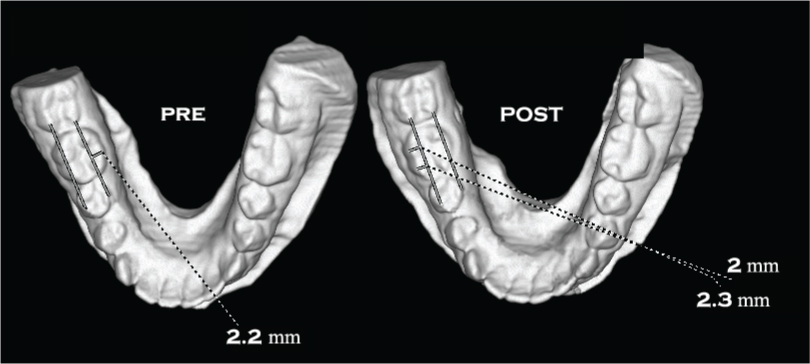
Models showing buccolingual uprighting of molar by 2.3 mm
Post treatment- simultaneous intrusion and buccolingual uprighting of mandibular first molar

Conclusion
The mini-implant is an efficient non-compliance device to intrude and upright the tooth simultaneously. It produces rapid intrusion without causing any adverse effects on any of the adjacent teeth. In this case report, efficient buccolingual uprighting and true intrusion of the mandibular molar was possible in 45 days and accurate measurement of intrusion and uprighting was done using dentascan software.
1]. A Carano, G Siciliani, J Bowman, Treatment of Skeletal Open Bite with a Device for Rapid Molar Intrusion: A Preliminary ReportAngle Orthod 2005 75:736-46. [Google Scholar]
[2]. JA McNamara, WL Brudon, Text book of Orthodontic and Orthopaedic Treatment in the Mixed Dentition1st Edition:182-84. [Google Scholar]
[3]. HS Hwang, KH Lee, Intrusion of overerupted molars by corticotomy and magnets.Am J Orthod Dentofacial Orthop 2001 120:209-16. [Google Scholar]
[4]. ND Kravitz, B Kusnoto, TP Tsay, WF Hohlt, The use of temporary anchorage devices for molar intrusion.JADA. 2007 138:56-64. [Google Scholar]
[5]. KD Dholakia, SR Bhat, Double impact: Intrusion of two mandibular molars using an SAS— A case reportOrthodontics (Chic) 2011 12(4):378-85. [Google Scholar]
[6]. E Nicolaievsky, The use of temporary anchorage devices for molar intrusion & treatment of anterior open biteBlum Oral-Facial Surgery Associates. Available from:https://www.drblumoralsurg.com [Google Scholar]
[7]. ND Kravitz, B Kusnoto, TP Tsay, WF Hohlt, Intrusion of Overerupted Upper First Molar Using Two Orthodontic MiniscrewsAngle Orthod 2007 77:915-22. [Google Scholar]
[8]. S Hoste, Vercruyssen M, Quirynen M and Willems G. Risk factors and indications of orthodontic temporary anchorage devices: a literature reviewAust Orthod J. 2008 24:140-48. [Google Scholar]