Emphysematous Cholecystitis in 24-Year-old Male Without Predisposing Factors
Asli Tanrivermis Sayit1, Hediye Pinar Gunbey2
1Faculty, Department of Radiology, Samsun Gazi State Hospital, Samsun, Turkey.
2Faculty, Department of Radiology, Ondokuz Mayis University Faculty of Medicine, Samsun, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Asli Tanrivermis Sayit, Faculty, Department of Radiology, Samsun Gazi State Hospital, Samsun, Turkey.
E-mail: draslitanrivermissayit@gmail.com
Emphysematous cholecystitis (EC) is a life threatening condition characterized by gangrene of the gallbladder due to an infection with gas-forming organisms. It is more common in elderly men and has been associated with systemic disease, especially diabetes and vascular disease. Computed tomography is the most important and accurate imaging modality for the diagnosis of EC. EC should be thought of when the radiographic presence of gas is detected within the gallbladder wall or lumen. Emergency surgical intervention and antibiotic treatment for the gas-forming organism should be initiated after the diagnosis of the EC. Here, we present the imaging and pathologic findings of a 24-year-old male with EC without any predisposing factors, successfully treated with laparoscopic cholecystectomy.
Computed tomography, Gall bladder, Gangrene
Case Report
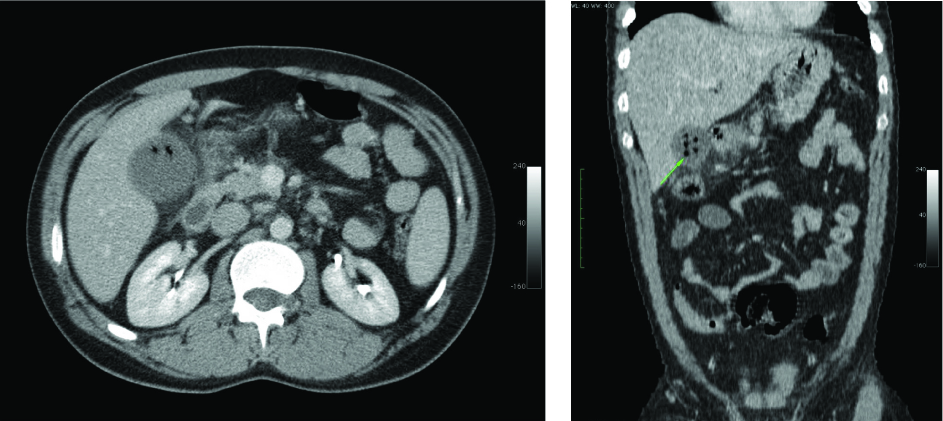
A 24-year-old male patient was admitted to the emergency service of Gazi State Hospital with epigastric pain exceeding two days despite treatment. Vital signs were normal on admission. Physical examination was normal except for mid-epigastric tenderness to palpation. The patient’s past medical history was normal. Laboratory results revealed leukocytosis with 15,000/mm3 (85.9% neutrophils), total bilirubin 2.35 mg/dl and direct bilirubin 0.71 mg/dl. Chest x-ray and abdominal X-ray [Table/Fig-1] in upright position were normal. Computed tomograpgy (CT) was performed on the patient due to his lack of response to medical therapy. Gas was observed in the gallbladder lumen by CT [Table/Fig-2a,b]. This was considered to be compatible with emphysematous cholecystitis (EC). There was no opaque stone in the gallbladder lumen. Intrahepatic bile ducts were normal. Free air was not detected, suggesting a perforation in the abdomen. The patient underwent laparoscopic cholecystectomy approximately two hours after the diagnosis of EC. Exploration of the abdominal cavity showed hydrops and necrosis of the gallbladder wall. Minimal pericholecystic and perihepatic collection were seen. The gallbladder was resected without complication. Multiple pigment yellow gallstones were found in the lumen of the resected gallbladder [Table/Fig-3a,b]. A drain was placed in the foramen of Winslow. The patient was treated with third-generation cephalosporin, proton pump inhibitors, and NSAIDs for three days. The patient was discharged at the end of the third day without any fluid in the drain.
Discussion
EC is a rare variant of ischemic disease of the gallbladder, which clinically mimics acute cholecystitis [1]. The mortality rate is 1.4% in uncomplicated patients [2]. However, the mortality and the morbidity rates can reach 25% and 50%, respectively, in complicated patients [1]. The male-to-female ratio is 7/3; 40% of EC patients also suffer from diabetes mellitus (DM). Most patients are over 50-year-old, and EC is rarely seen with gallstones [3,4]. EC occurs as a result of primarly ischemic pathologies and predisposing factors include DM, vasculitis, atherosclerosis and arterial embolic diseases [3]. Also, abdominal surgery and trauma are the other risk factors of the EC [3]. Here, we present the case of a 24-year-old male patient who was diagnosed with EC without any predisposing factors.
EC usually begins as acute cholecystitis; after that, ischemia and gangrene develop in the gallbladder wall [4]. Gas accumulation in the wall and lumen of the gallbladder is a result of the mural translocation of the gas producing anaerobic bacteria. Clostridium welchii, Clostridium perfringens, Escherichia coli, Klebsiella and Streptococci have been reported in the literature as causative organisms [5]. Clostridia is the most common bacterial agent for EC. The symptoms of EC are similar to those of acute cholecystitis, including right upper quadrant pain, nausea, vomiting, and lowgrade fever [1]. EC is generally considered a surgical emergency, and patients should be treated immediately. EC is associated with much higher rates of gangrene and perforation of the gallbladder and significantly increased rates of mortality when compared with nonemphysematous cholecystitis [5]. Also, pericholecystic abscess, and bile peritonitis are the other complications of the EC [2].
Imaging modalities such as plain radiography, ultrasonography (USG), and CT can be used for the diagnosis. Plain radiography can show a gaseous halo around the gallbladder and gas-fluid level in the gallbladder [3]. USG is an operator-dependent technique and findings of EC can vary depending on the number of air pockets and localization. Echogenic foci with reverberation artifacts can be seen in the gallbladder lumen due to a small amount of air. A large amount of air can be seen as a broadband with a posterior acoustic shadow. USG is less sensitive and specific for detecting the air in the soft tissues compared to other imaging modalities [2]. A gallbladder completely filled with stones or a porcelain gallbladder may be difficult to visualize with USG. Also, in some cases pericholecystic fluid can mingle with the intestinal loops, causing false negative results [2,3]. CT is the most sensitive and specific imaging modality for identification of gas in the gallbladder lumen and biliary ducts [2]. In addition to gas in the gallbladder wall, gas-fluid level in the lumen and pericholecystic oedema can be seen. CT is a useful modality that helps to confirm the diagnosis and exclude other differential diagnosis [5]. In our case, a chest X-ray and abdominal X-ray in the upright position were normal. But CT showed gas in the hydropic gallbladder lumen without radioopaque gallstones. Also, there was no gas in the biliary ducts and there was free gas in the abdomen suggesting perforation of the gallbladder [5]. A definitive diagnosis can be made with a cholecystectomy, so patients with a diagnosis of EC should be operated on immediately. Intravenous antibiotics should also be initiated against anaerobes and other digestive germs. In the present case, the patient was taken to surgery about two hours after the diagnosis. He was also treated with third-generation generation cephalosporin, proton pump inhibitors, and NSAID for three days. We preferred a laparoscopic cholecystectomy because of the young age of the patient; the laparoscopy was performed without any complication.
Upright abdominopelvic X-ray was normal
Abdominopelvic computed tomographic (CT) scans of axial and coronal views showed intraluminal gas consistent with emphysematous changes
A macroscopic image of the gallbladder and yellow cholesterol gallstones

Conclusion
It should be kept in mind that EC can be seen in patients with symptoms of acute cholecystitis. CT should be performed on patients not diagnosed by plain radiography and USG, because delayed diagnosis increases complications. Our case presentation is remarkable due to the young age of the patient and his lack of any predisposing factor. It should kept in mind that EC can be seen in younger patients, and abdominopelvic CT should be performed on suspected cases of EC, including in the case of young patients with epigastric pain that does not respond to treatment.
[1]. H Katagiri, Y Yoshinaga, Y Kanda, K Mizokami, Emphysematous cholecystitis successfully treated by laparoscopic surgeryJ Surg Case Rep 2014 4 pii:rju027. doi: 10.1093/jscr/rju027 [Google Scholar]
[2]. A Sunnapwar, AA Raut, AM Nagar, R Katrey, Emphysematous cholecystitis: Imaging findings in nine patientsIndian J Radiol Imaging 2011 2:142-46. [Google Scholar]
[3]. JC Le Brun, RM Katz, AA Nasr, JJ Rommens, Emphysematous cholecystitis in a non-diabetic patientJBR-BTR 2013 96:316 [Google Scholar]
[4]. H Miyahara, D Shida, H Matsunaga, Y Takahama, S Miyamoto, Emphysematous cholecystitis with massive gas in the abdominal cavityWorld J Gastroenterol 2013 19:604-06. [Google Scholar]
[5]. JW Hazey, FJ Brody, SM Rosenblatt, J Brodsky, J Malm, JL Ponsky, Laparoscopic management and clinical outcome of emphysematous cholecystitis Surg Endosc 2001 15:1217-20. [Google Scholar]