Introduction
Dental caries is one of the most prevalent diseases of the oral cavity, having a multifactorial etiology and characterized by the destruction of organic and inorganic matrix. It has no sex predilection and equally effects individuals from all age groups [1]. In 17th century, Leeuwenhoek found the role of bacteria in the etiology of dental caries and coined the term “little animalcules” [2]. Later in 1890, the association of these bacteria with pulpal and periapical pathologies was reported by WD Miller. There has been greater research on bacteria causing caries initiation and early caries progression, although microbiology of dentinal caries is yet to be fully characterized [3].
The most commonly isolated microorganism from a carious lesion is S.mutans and has been target microorganism for routine cultures. However, Clarke in 1924 noted that caries could develop in the absence of S.mutans and a wide variety of microorganisms (Lactobacillus acidophilus, Staphylococcus, proteolytic bacteria, anaerobic organism including Prevotella, Vellionella, Fusobacterium, Actinomyces viscosus, etc) were identified which aid in caries initation and progression [4,5].
Multiple factors, such as the interaction of bacteria, diet, oral hygiene, plaque, immunity, time and host respons, all influence dental caries initiation and progression. It is uniformly agreed that caries cannot occur without microorganisms. Bacterial accumulation is mediated by both bacterially derived polymers and salivary components. Although saliva plays an important role in optimal oral health and new research suggests that salivary pH is even more critical to theAhluwalia5caries development and progression, as low salivary pH promotes the growth of acidogenic bacteria in the oral cavity [6].
From past so many years, surgical treatment has been followed in many dental offices to remove the decayed tooth structure. The flaw in this approach is that the causative organisms are not removed completely and to overcome these problems antimicrobials like penicillin, erythromycin was used. But with time, resistance has developed among the various caries pathogens against these antimicrobial drugs. This results in compelling evidence to progress with clinical assessments of antibiotic susceptibility and various microbiological efforts to understand the limits of this everlasting problem [7].
Aim
The aim of study was to evaluate the caries pathogens from dentinal caries other than S. mutans and to screen the emergence of drug resistance among the caries causing pathogenic microorganisms.
Materials and Methods
The study was conducted from May 2014 to September 2014 in the Department of Oral Pathology at Vyas Dental College and Hospital. In the present study 75 patients with permanent dentition, having dental caries were selected. The presence of caries was confirmed by visual and radiographic examination. Soft carious dentin, easily removable with spoon excavator was isolated from the lesion and was used as specimen for culturing. The collected specimens were processed after obtaining the informed consent from the patients and a proforma was recorded for each study case to analyse the age, sex, occupation, marital status, food habits and detailed clinical examination.
After the removal of superficial plaque and debris overlying the lesion, the carious zone of decalcified and partially decalcified dentine was washed with sterile saline, carious dentine was then excavated with sterile spoon excavators which was transferred in to vials of sterile normal saline to a concentration of approximately 10 mg (wet weight) of dentine per ml prior to processing [Table/Fig-1].
The collected samples were brought to the microbiology laboratory and were processed within 3 hours of collection. Samples were dispersed in the transport medium by using a Vortex mixer and the broth was incubated at 37°C for 2 hours. Later on broth was inoculated on to, nutrient agar and mac-conkey agar which was incubated at 37°C for 48 hours each.
The isolates were then identified by colony morphology; grams staining and were stored at 4°C until subjected for the antimicrobial susceptibility test. Briefly, colonies of the test organisms were touched with a sterile loop and transferred into sterile Mueller Hinton broth under aseptic conditions and were incubated at 37°C for 2 hours until the density of each microbial suspension reached to 106 colony forming units per ml (CFU/ ml).
One hundred microliter of the inoculum of each test organism was spread as lawn cultures onto sterile Mueller Hinton agar plates using L-rods to achieve a confluent growth. Discs of first, second, third line of antibiotics, along with newer (beta lactam) antibiotics were placed on the culture plates of staphylococcus and pseudomonas strains [Table/Fig-2], the plates were then incubated at 37°C for 18 hours and the zone of inhibition was measured by using Kirby Bauer’s disc diffusion method [8].
Results
In this study out of 75 patients more common isolates were Staphylococcus aureus, Klebsiella, Pseudomonas aeruginosa, Yeast. The predominant were Staphylococcus and Pseudomonas [Table/Fig-3].
The most prevalent micro-organisms were Staphylococcus aureus and Pseudomonas aeroguinosa. These strains were isolated and the antibiotic sensitivity tests were carried out. Microorganisms which were sensitive showed zones of inhibition, which were resistant, showed absence of zone of inhibition [Table/Fig-4]. After which, statistical analysis of the samples was done using paired t-test and p-value was calculated. P-value was found to be significant in case of first, second and third line antibiotics against both strains (Pseudomonas and Staphylococcus), whereas it was highly significant in case of newer antibiotics [Table/Fig-5]. Thereby, newer antibiotics were proved to be effective against the microbial pathogens.
Discussion
Dental caries is an irreversible microbial disease of the calcified tissues of the teeth, which often leads to cavitation in the teeth. It is a complex and dynamic process where a multiple factors influence and initiate the progression of disease [9]. The microbiology of caries is complex and dependent upon interactions of protective and pathologic factors in saliva and plaque biofilm as well as balance between the cariogenic and non-cariogenic microbial population that reside in saliva [10,11]. Some of the oral cariogenic bacteria like Staphylococcus aures, Klebisella, Pseudomonas aeruginosa were also identified in the present study.
The mutans group of streptococci play a central role in the initiation of caries on the smooth surfaces and fissures of the crowns in the teeth of adults and children. They also have a potent etiologic role in the induction of root surface caries [12]. Although S. mutans is most commonly found microorganism in dental caries, but the presence of staphylococci has been recognized in few detailed studies [13].
It is evident from this study that the dentinal caries were contaminated with cultivable microorganisms other than streptococci, which is in full agreement with the results of studies done by several authors. Alicia et al., identified staphylococcus species and Candida ablicans in dental caries and periodontal pockets of periodontal disease patients [14]. Oluremi et al., found prevalence of staphylococcus, followed by other microorganisms (S.mutans, Lactobacilli) in dental caries [15]. Daniyan et al., found prevalence and susceptibility of staphylococcus isolates of dental caries in a secondary health care institution [16]. Similarly the present study was aimed to detect the role of microflora other than S. mutans in caries as not much research has been done on the other cultivable microorganisms present in dental caries. Staphylococci was the predominant strain, which was in conjunction with previous studies. The exact role of staphylococcus in caries is still not clear, but it is believed to play an important role in caries initiation and progression.
Dental caries has been treated by removal of diseased tooth structure or faulty restorations prior to placement of materials to restore form and function. The underlying thought for this approach must be that surgical removal of the nidus of infection will inhibit the disease processes. However, the flaw in this method is that the removal of the demineralized/diseased tooth structure does not result in complete elimination of the causative infection because if foci of infection persist it will result in recurrence, so the next step is to treat the remaining infection with effective antimicrobial agents [3]. It has been reported that the introduction of antimicrobials in the prophylactic treatment has reduced the infection, but the long term use of these antibiotics could be compromised by emergence of resistant strains [3].
The utilization of antimicrobials in treating dental caries has gained much attention worldwide. But the widespread concern is emerging drug resistance among the pathogenic population has worsened the treatment regimens in dentistry. The developing resistance of bacteria to these common antimicrobial agents is a cause of concern for the dentist [3]. The resistance developed to antimicrobial agents can arise from the selection of resistant strains among naturally susceptible species or from the ingress of newer strains of naturally resistant species. Greater use of a single antimicrobial agent in a given environment directly dictates the rate of resistance among the different microbial populations [17].
A potential post antibiotic era is threatening present and future of medical advances in treating dentinal caries [18]. Overuse and abuse of antibiotics are the main factors responsible for the development of resistance against antibiotics. Bacteria such as Staphylococcus aureus, S. mutans, Pseudomonas aeruginosa, Klebsilla are few among the antibiotic resistant bacteria [19].
Amongst all these caries pathogens, development of resistance to antimicrobial agents by Staphylococci is a major concern primarily because they are still frequently associated with hospital and community – acquired infections. These organisms exhibit remarkable versatility in their behaviour towards antibiotics, with some strains becoming resistant to commonly used drugs like pencillin, erythromycin, etc [20]. Therefore, in context to lowering down the antimicrobial resistance rate; it is imperative to consider routine susceptibility testing. Such tests could be useful in improving the efficacy of treatment.
In this study, three generation of antibiotics, along with newer antibiotics were used to assess the changing pattern of resistance to antibiotics in bacteria isolated from carious lesions. Antibiotics used in the present study have shown to be effective against Staphylococcus and Pseudomonas, which was in conjunction with previous studies. The rationale of using different spectrum of antibiotics was to determine their efficacy against these microorganisms and also to assess the resistant strains developed against the known antibiotics. Both broad spectrum antibiotics (tetracycline, amoxyclav) and narrow spectrum antibiotics (ciprofloxacin, cefazolin, carbenicillin, vancomycin etc) were used in the present study, which were proven to effective against the bacteria to be tested.
Staphylococcus were found to be most predominant out of which 20% were found to be resistant to penicillin and 1% were found to be resistant to erythromycin. These values were significantly less when compared to a previous studies done by Uwaezuoke et al., and Dwivedi et al., in which they found 95.8% and 48% samples resistant to penicillin respectively [17,21]. Second most predominant bacteria isolated was pseudomonas, most of its samples were found to be resistant to fluoroquinolones, which is in conjunction with a previous study done by Mac Dougall et al., [20]. When comparing the various generations of antibiotics 80% of the staphylococci were sensitive to all lines of antibiotics and only 10 % were found resistant to antibiotics in present study. 70% of pseudomonas was found to be resistant to first three lines of antibiotics although 73% samples exhibited sensitivity to the newer antibiotics.
Selection of an antibiotic regimen should always be based on knowledge of the efficacy of an antibiotic for the bacteria. It should also be remembered that dental caries represent an ecosystem of bacteria in which by-product of one species of bacteria may be nutrient of other bacteria. Thus, an antibiotic that is effective against a few species of bacteria in polymicrobial infection, may indirectly affect all or some of these bacteria in that ecosystem. Therefore, the study results depict that the growing resistance among pathogenic bacteria against the commonly prescribed antibiotics will be eliminated by the usage of newer antibiotics [22].
Recently, newer advances like hard tissue lasers, chemomechanical methods etc. have been introduced for conservatively removing carious lesions while simultaneously nanotechnology in dentistry has been developed as a drug delivery system for control of biofilm dependent oral diseases. Such advances will be helpful in successful management of these diseases which will certainly open a new avenue to overcome diseases like dental caries [23-25]. Dental caries, a disease of great antiquity, is not a disease of past since it is reappearing in many countries as a public health crisis. It is therefore, important that public health be caught on prevention, early recognition and reporting to dental offices for proper prognosis. This underscores the need of early diagnosis, to rule out the antimicrobial resistance against the microorganisms for proper management and increasing the efficacy of treatment.
10mg of carious dentin in 1ml of normal saline
Various generations of antibiotics used
| Generations of antibiotics | Names of Antibiotics used |
|---|
| First line of antibiotics | Pencillin (500mg), tetracycline (500mg), ciprofloxacin (500mg), ofloxacin (500mg) |
| Second line of antibiotics | Cefixime (500mg), Levofloxacin (500mg) Vancomycin (500mg), azithromycin (500mg) |
| Third line of antibiotics | Cefepime (1000 mg), Meropenem (500mg) Tobramycin (1200mg) |
| Newer antibiotics (beta lactam) | Cefazolin (500mg), Amoxyclav (625mg) Carbenicillin (764mg) |
Bacterial distribution according to gender
| Bacteria | Gender | Total |
|---|
| Male | Female |
|---|
| Staphylococcus aureus | 24 | 10 | 34 |
| Pseudomonas sp. | 19 | 5 | 24 |
| Klebsiella | 1 | 3 | 4 |
| Yeasts | 1 | 4 | 5 |
| No Microrganism | 5 | 3 | 8 |
| Total | 50 | 25 | 75 |
Graph showing antibiotic efficacy against staphylococcus and pseudomonas strains
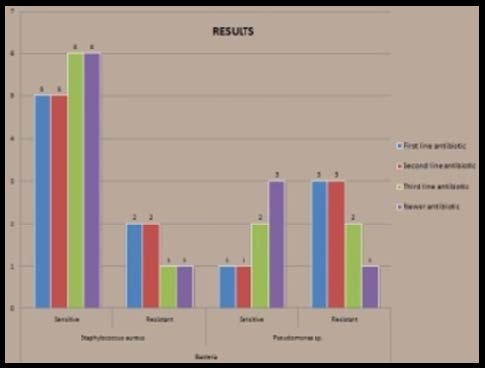
Chart showing p-value calculated in both bacterial strains
| Staphylococcus aureus | Results |
|---|
| t- test | df | p <.05 |
|---|
| First line antibiotics | 16.316 | 6 | .001 |
| Second line Antibiotics | 16.316 | 6 | .001 |
| Third line Antibiotics | 17.728 | 6 | .001 |
| Newer antibiotics | 17.728 | 6 | .0005 |
| Pseudomonas aeruginosa | Results |
| t- test | Df | p <.05 |
| First line antibiotics | 16.734 | 3 | .006 |
| Second line Antibiotics | 12.969 | 3 | .006 |
| Third line Antibiotics | 12.170 | 3 | .014 |
| Newer antibiotics | 12.170 | 3 | .015 |
Conclusion
There are different ways of accomplishing the removal of the pathogens by developing targeted antimicrobials and is part of the continuing evolution of the treatment of oral infection that produces the clinical manifestations of dental caries. As a profession, we are slowly moving away from the purely surgical approach to treating this disease. Regardless of which of these or other strategies emerges as a winner in the war on caries, it is most interesting that these technologies will serve whole other areas of health care as well.
[1]. J Moses, BN Rangeeth, D Gurunathan, Prevelance of dental caries, socioeconomic status and treatment needs among 5-15 year old school going children of ChidambaramJ Clin Diagn Res 2011 5:146-51. [Google Scholar]
[2]. RR Russell, Changing concepts in caries microbiologyAm J Dent 2009 22:304-08. [Google Scholar]
[3]. MH Anderson, A probiotic approach to caries managementPediatr Dent 2006 2:151-53. [Google Scholar]
[4]. M Maltz, EF Oliveira, V Fontanella, R Bianchi, A clinical, microbiologic and radiographic study of deep caries lesions after incomplete caries removalQuintessence Int 2002 33:151-59. [Google Scholar]
[5]. PW Caufield, AP Dasanayke, Y Li, The antimicrobial approach to caries managementJ Dent Educ 2001 65:1091-95. [Google Scholar]
[6]. N Kianoush, CJ Adler, AT Nguyen, GV Browne, M Simonian, N Hunter, Bacterial Profile of Dentine Caries and the Impact of pH on Bacterial Population DiversityPLOS ONE 2014 9(3):e92940 [Google Scholar]
[7]. GA Smiline, SK Pandi, P Hariprasad, R Raguraman, A preliminary study on the screening of emerging drug resistance among the caries pathogens isolated from carious dentineIndian J Dent Res 2012 23(1):26-30. [Google Scholar]
[8]. AW Bauer, WM Kirby, JC Sherris, M Turck, Antibiotic susceptibility testing by standardized single disk methodAm J Clin Pathol 1986 45:493-96. [Google Scholar]
[9]. C Usha, R Sathyanarayanan, Dental caries - A complete changeoverJ Conserv Dent 2009 12(Suppl 2):46-54. [Google Scholar]
[10]. P Gupta, N Gupta, AP Pawar, SS Birajdar, AS Natt, HP Singh, Role of Sugar and Sugar Substitutes in Dental Caries: A ReviewISRN Dentistry 2013 2013:519421 [Google Scholar]
[11]. B Sakeenabi, SS Hiremath, Dental caries experience and salivary Streptococcus mutans, lactobacilli scores, salivary flow rate, and salivary buffering capacity among 6-year-old Indian school childrenJ Int Soc Prev Community Dent 2011 1:45-51. [Google Scholar]
[12]. M Jason, D Tanzer, L Livingston, M Angela, BS Thompson, The microbiology of primary dental caries in humansJ Dent Educ 2001 65(10):1028-37. [Google Scholar]
[13]. V Bueris, FC Pimenta, IY Ito, JM Marin, Oral incidence of staphylococcus aureus and antimicrobials agents resistanceBraz j Oral Sci 2005 4:676-78. [Google Scholar]
[14]. AI Cuesta, V Jewtuchowicz, MI Brusca, ML Nastri, AC RosaAlicia, V Jewtuchowicz, Prevalence of staphylococcus spp in the oral cavity and periodontal pockets of periodontal disease patientsActa Odontol Latinoam 2010 23:20-26. [Google Scholar]
[15]. BB Oluremi, MO Osungunna, OA Idowu, OO Adebolu, Evalutation of anticaries activity of selected mouthwash marketed in NigeriaTropical journal of pharmaceutical research 2010 9(6):581-86. [Google Scholar]
[16]. SY Daniyan, ME Abalaka, Prevalance and susceptibility pattern of bacterial isolates of dental caries in a secondary health care institution NigeriaShiraz E Med J 2011 12:1-7. [Google Scholar]
[17]. JC Uwaezuoke, LE Aririatu, A survey of antibiotic resistant staphylococcus aureus strains from clinical sources in OwerriJournal of Applied Sciences & Environmental Management 2004 8(1):67-69. [Google Scholar]
[18]. O Cars, P Nordberg, Antibiotic resistance- The faceless threatInt J Risk Saf Med 2005 17:103-10. [Google Scholar]
[19]. TJ Pallasch, Antibiotic resistanceDent Clin N Am 2003 47:623-39. [Google Scholar]
[20]. C Macdougall, SE Harpe, JP Powell, CK Johnson, MB Edmond, RE Polk, Staphylococcus aureus, Pseudomonas aeruginosa flouroquinolone useEmerg Infect Dis 2005 11(8):1197-210. [Google Scholar]
[21]. D Dwivedi, T Kushwah, M Kushwah, V Singh, Antibiotic susceptibility pattern against pathogenic bacteria causing Dental CariesSouth Asian Journal of Experimental Biology 2011 1(1):31-35. [Google Scholar]
[22]. ED Coelho, JP Arrais, J Matos, C Pereira, N Rosa, MJ Correia, Computational prediction of the human-microbial oral interactomeBMC Systems Biology 2014 8:24-16. [Google Scholar]
[23]. AC Jorge, A Cassoni, PM Freitas, AF Reis, A Brugnera Junior, JA Rodrigues, Influence of cavity preparation with Er,Cr:YSGG laser and restorative materials on in situ secondary caries developmentPhotomed Laser Surg 2015 [Google Scholar]
[24]. MM Ammari, LF Moliterno, R Hirata Junior, MC Sellos, VM Soviero, WP Coutinho Filho, Efficacy of chemomechanical caries removal in reducing cariogenic microbiota: a randomized clinical trialBraz Oral Res 2014 28(1):1-6. [Google Scholar]
[25]. FF de Sousa, C Ferraz, LK Rodrigues, S Nojosa Jde, M Yamauti, Nanotechnology in dentistry; drug delivery systems for the control of biofilm-dependent oral diseases.Curr Drug Deliv 2014 11(11):719-28. [Google Scholar]