Osteoporosis is a systemic skeletal disease characterized by low bone mass and micro architectural deterioration with consequent increase in bone fragility and susceptibility to bone fracture. Osteoporosis is often called as a “Silent disease” because bone loss occurs without causing symptoms [1]. In humans, bone decreases in density and increases in porosity with ageing [2].
Periodontitis is a common, complex inflammatory disease characterized by destruction of tooth supporting soft and hard tissues of the periodontium. It is the main factor for tooth loss in adult population throughout the world [3]. As periodontal disease progresses, the collagen fibers and connective tissue attachment of the tooth are destroyed. The junctional epithelial cells proliferate apically along the root surface, and these structural changes are reflected clinically as attachment loss or increased probing pocket depth. Periodontal inflammation affects homeostasis of bone tissue by triggering the resorptive process that represents the main characteristic of destructive periodontal disease [3].
Periodontal disease and osteoporosis affects millions of people worldwide. Both the diseases lead to a significant morbidity, mortality and expenses. Periodontitis is a local disease, while osteoporosis is a systemic disease and bone loss is a common feature of both diseases. The evaluation of the relationship between osteoporosis and periodontitis is complicated as both the diseases are multifactorial in aetiology. Multiple systemic factors influence the onset and progression of osteoporosis including age, race, genetic factors, diet, gender, hormone therapy, tobacco use, sedate lifestyle and obesity. Several of these factors also increase the risk for periodontal tissue destruction. Furthermore local factors such as bacterial plaque and calculus, may also mask the effect of osteoporosis on periodontal tissue destruction [4].
Previous studies conducted to correlate osteoporosis and periodontitis have shown a positive correlation [4,5], while other studies have shown negative correlation [6,7]. Hence, there is a need to study the relationship between periodontitis and osteoporosis that has practical significance in the diagnosis, prevention and treatment of both the diseases.
The present study was designed to assess and Correlate the severity of osteoporosis and periodontal disease by using variables like probing pocket depth, clinical attachment loss, plaque index, body mass index and bone mineral density, in selected population of Maharashtra.
Materials and Methods
This descriptive cross-sectional study was conducted on 65 subjects randomly selected by purposive sampling technique, from outpatient section of Department of Periodontology. The research protocol was submitted to the Institutional Ethical committee and ethical committee clearance was obtained before commencing the study. The study was conducted during the period from January 2014 to June 2014.
Inclusion criteria’s: Subjects aged between 45-75 years suffering from periodontitis, with at least 15 natural teeth. Subjects who were willing to participate in the study and gave an informed consent.
Exclusion criteria’s: Subjects receiving long term calcium supplements, systemic steroids and hormonal replacement therapy. Subjects with history of parathyroid disease, metabolic bone disease and malignancy. Subjects who used tobacco in smoked or smokeless form were excluded from the study.
Out of 75 subjects enrolled only 65 were recruited for the study, as ten subjects did not fulfill the inclusion criteria’s. The personal, medical, dental and osteoporosis history were recorded on predesigned proforma. Body mass index (BMI) of all the subjects was calculated by dividing weight in kilograms by height in meters squared and tabulated.
Periodontal Examination: The clinical parameters like plaque index (PI), probing pocket depth (PPD) and clinical attachment loss (CAL) were recorded by junior researcher and the values were validated and confirmed by senior periodontist to minimize the observer bias. A disclosing agent (Alphaplac, DPI, Wallace Street, Mumbai) was used to disclose the plaque during the examination. Plaque index was measured using Turskey-Gilmore-Glickman Modification of the Quigley Hein Plaque Index, 1970. An index for entire mouth was determined by dividing the total score by the number of surfaces examined, Score 0 or 1 is considered as low and score 2 or more was considered high [8].
The level of periodontitis was assessed using parameters PPD and CAL, with a periodontal probe (UNC-15, Hu-friedy, Chicago, IL). The periodontal probe was inserted parallel to the vertical axis of the tooth and walked circumferentially around each tooth with standardized constant probing force. The measurements were recorded on four sites per tooth (mesiobuccal, distobuccal, midbuccal and midlingual) of all the teeth, except third molars. Probing pocket depth was measured from gingival margin to the base of gingival sulcus. Clinical attachment loss was measured from cementoenamel junction (CEJ) to base of gingival sulcus. The participants were classified as having chronic periodontitis based on 1999 consensus classification of periodontal disease [9]. Based on the average CAL all chronic periodontitis subjects were categorized into three categories: slight (1 to 2mm CAL), Moderate (3 to 4mm) and Severe (≥5mm CAL).
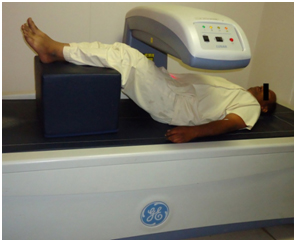
Bone mineral density (BMD) Investigation: BMD of the subjects was measured using dual energy x-ray absorptiometry (DXA) with Prodigy system (GE, Prodigy health care system, Madison WI, encore version 12.30). The BMD of lumbar vertebrae was measured in anteroposterior view of lumbar vertebrae one to four (L1 to L4) [Table/Fig-1]. All DXA scans were performed by a single calibrated examiner, who was blinded to the periodontal status of the patients.
Anteroposterior view of lumbar vertebrae one to four (L1 to L4) by DXA scans
The DXA value or ‘T’ score is a comparison of patients BMD to that of a healthy 30-year-old adult with peak bone mass. The World health organization defines osteoporosis and osteopenia by measures of standard deviation (SD) as compared to that of normal healthy young adult [1]. According to WHO guideline it is graded as follows [10] [Table/Fig-2].
World health organization criteria for defining osteoporosis and osteopenia [10]
| Condition | Description |
|---|
| Normal | BMD ≤ 1 SD below the mean for a young healthy adult |
| Osteopenia | BMD > 1 but < 2.5 SD below the mean for young healthy adult |
| Osteoporosis | BMD ≥ 2.5 SD below the mean for a young healthy adult |
The obtained data was entered in MS excel sheet and subjected to statistical analysis and correlated.
Statistical Analysis
Statistical analysis was performed using Statistical package for the social science software (SPSS Inc. Released 2007. SPSS for Windows, Version 16.0. Chicago). Descriptive statistics like frequency and percentage were calculated for all the variables. Chi-square test was performed to assess the association between study variables. Association was said to be significant if p ≤ 0.05.
Results
Gender and osteoporosis distribution: Out of 65 subjects 41 were males and 24 were females. Out of 41 male subjects, 22 had normal BMD value, 14 were osteopenic and five were osteoporotic. Out of 24 female subjects, 11 had normal BMD value, five were osteopenic and eight were osteoporotic. The findings suggest that, females had higher level of osteoporosis as compared to males [Table/Fig-3].
Gender wise distribution of osteoporosis
| Parameter | Males | Females |
|---|
| n | % | n | % |
|---|
| Normal | 22 | 53.65% | 11 | 45.83% |
| Osteopenia | 14 | 34.14% | 5 | 20.83% |
| Osteoporosis | 5 | 12.19% | 8 | 33.33% |
| Total | 41 | 100% | 24 | 100% |
Association between periodontitis and osteoporosis: Slight periodontitis was observed in eight subjects and their BMD values were normal. Moderate periodontitis was observed in 24 subjects, out of whom 17 had normal BMD values and seven were osteopenic. Severe periodontitis was observed in 33 subjects, out of whom eight had normal BMD values, 12 were osteopenic and 13 subjects suffered from osteoporosis. There was significant association between periodontitis and osteoporosis (P= 0.0001). The results suggest that, as the severity of periodontitis increased the level of osteoporosis also increased [Table/Fig-4].
Correlation between periodontitis and osteoporosis
| Periodontitis | Normal | Osteopenia | Osteoporosis | Chi-square value | p-value |
|---|
| n | % | n | % | n | % |
|---|
| Slight | 8 | 24.24% | 0 | 0% | 0 | 0% | 25.81 | 0.0001* |
| Moderate | 17 | 51.51% | 7 | 36.84% | 0 | 0% |
| Severe | 8 | 24.24% | 12 | 63.15% | 13 | 100% |
| Total | 33 | 100% | 19 | 100% | 13 | 100% |
* Correlation was statistically significant (p ≤ 0.05)
Association between periodontitis and PI: Slight periodontitis was observed in eight subjects and all had high plaque index score. Moderate periodontitis was observed in 24 subjects, of which nine had low plaque score and 15 had high plaque score. Thirty three subjects had severe periodontitis, of which five had low plaque score and 28 had high PI score. As the PI score increased, periodontitis also increased from slight to severe. There was statistically significant association between periodontitis and PI score (p=0.036) [Table/Fig-5].
Correlation between periodontitis and PI score
| Parameter | Plaque index | Plaque Index | Chi-square value | p-value |
|---|
| Low | High |
|---|
| n | % | n | % |
|---|
| Slight | 0 | 0% | 8 | 15.68% | 6.611 | 0.036* |
| Moderate | 9 | 64.28% | 15 | 29.41% |
| Severe | 5 | 35.71% | 28 | 54.90% |
| Total | 14 | 100% | 51 | 100% |
* Correlation was statistically significant (p ≤ 0.05)
Association of PI score and osteoporosis: Thirty three subjects had normal BMD value, of which seven had low plaque score and 26 had high plaque score. Osteopenia was observed in 19 subjects of which, five subjects had low plaque score and 14 had high plaque score. Osteoporosis was observed in 13 subjects, and all the subjects had high plaque score. There was no significant correlation between PI score and osteoporosis [Table/Fig-6].
Correlation between osteoporosis and PI score
| Osteoporosis | Plaque index | Plaque Index | Chi-square value | p-value |
|---|
| Low | High |
|---|
| n | % | n | % |
|---|
| Normal | 7 | 58.33% | 26 | 49.05% | 3.888 | 0.1431¶ |
| Osteopenia | 5 | 41.66% | 14 | 26.41% |
| Osteoporosis | 0 | 0% | 13 | 24.52% |
| Total | 12 | 100% | 53 | 100% |
¶ Correlation was not statistically significant (p≥ 0.05)
Association between osteoporosis and BMI: Thirty three subjects had normal bone mineral density (Healthy) of which five had normal body mass index, 17 subjects were overweight and 11 were obese. Osteopenia was observed in 19 subjects of whom four had normal BMI, nine subjects were overweight and six were obese. Osteoporosis was observed in 13 subjects, of which one subject was underweight, four subjects had normal BMI, five subjects were overweight and three subjects were obese. Correlation of BMI with osteoporosis did not show any statistical significance [Table/Fig-7].
Correlation between level of osteoporosis and BMI
| Parameter | Underweight | Normal | Overweight | Obese | Chi-square value | p-value |
|---|
| n | % | n | % | n | % | n | % |
|---|
| Normal | 0 | 0% | 5 | 30.46% | 17 | 54.83% | 11 | 55% | 7.64 | 0.2655¶ |
| Osteopenia | 0 | 0% | 4 | 30.76% | 9 | 29.03% | 6 | 30% |
| Osteoporosis | 1 | 100% | 4 | 30.76% | 5 | 16.12% | 3 | 15% |
| Total | 1 | 100% | 13 | 100% | 31 | 100% | 20 | 100% |
¶ Correlation was not statistically significant (p≥ 0.05)
Association of periodontitis and BMI: Slight periodontitis was observed in eight subjects of whom one subject had normal BMI, six were overweight and one was obese. Moderate periodontitis was observed in 24 subjects of whom three had normal BMI, 13 were overweight and eight were obese. Severe periodontitis was observed in 33 subjects of whom one was underweight, nine had normal BMI, 12 were overweight and 11 were obese. Correlation between BMI and periodontitis showed no statistical significance [Table/Fig-8].
Correlation between periodontitis and BMI
| Parameter | Underweight | Normal | Overweight | Obese | Chi-square value | p-value |
|---|
| n | % | n | % | n | % | n | % |
|---|
| Slight | 0 | 0% | 1 | 7.69% | 6 | 19.35% | 1 | 5.00% | 3.935 | 0.685¶ |
| Moderate | 0 | 0% | 3 | 23.07% | 13 | 41.93% | 8 | 40% |
| Severe | 1 | 100% | 9 | 69.23% | 12 | 38.70% | 11 | 55% |
| Total | 1 | 100% | 13 | 100% | 31 | 100% | 20 | 100% |
¶ Correlation was not statistically significant (p≥ 0.05)
Discussion
Osteopenia and osteoporosis are characterized by reduction in bone mass and may lead to skeletal fragility and fracture. Osteoporosis may be a primary disorder or secondary to other diseases. Primary osteoporosis includes idiopathic and involution form: Idiopathic form of osteoporosis is rare and affects men and women equally. Involutional osteoporosis includes two patterns, type 1: postmenopausal osteoporosis and type 2: age related osteoporosis. Accelerated rate of cortical bone loss occurs in type 1 and is related to estrogen deficiency. Age related osteoporosis type 2 affects virtually the entire population of aging men and women [11].
Periodontitis is an inflammatory disease characterized by loss of connective tissue and alveolar bone [9]. The aetiological agent in periodontitis is pathogenic bacteria plaque, in a susceptible patient. Periodontitis and osteoporosis have several risk factors in common. They include an increased prevalence with age, tobacco use and influence of disease or medication that may interfere with healing [11].
The possible mechanism by which osteoporosis leads to increased alveolar bone destruction, may be due to reduced alveolar bone per unit volume in osteoporosis patients. Patients who have systemic bone loss may react to periodontitis with increased production of cytokines and inflammatory mediators. The elevated levels of Interleukin -1, 6 and Tumour necrosis factor in osteoporosis patients leads to increased osteoclastic activity, further leading to alveolar bone loss in patients with periodontitis.
In the present study dual energy X-ray absorptiometry (DXA) was used to assess BMD in lumbar spine (L1-L4) which is similar to the previous studies [9,12,13]. DXA measurements are good predictors of fracture risk because the vertebrae is least affected by artifacts and earlier detection of change in bone mineral content is possible [11].
Among 65 patients in this study, 33 subjects (50.76%) had normal BMD value, 19 (29.23%) were identified as having osteopenia and 13 (20%) suffered from osteoporosis. Among 33 subjects who had normal BMD values 22 were males and 11 were females. Out of 19 osteopenic patients, five were females and 14 were males. Out of 13 osteoporotic patients, eight were females and five were males indicating that more members of females suffered from, osteoporosis as compared to males. This could be due to estrogen withdrawal following menopause leading to increased osteoclast number and enhanced osteoclast formation.
Slight periodontitis was observed in eight subjects and the BMD values were normal. Moderate periodontitis was observed in 24 subjects, of whom 17 had normal BMD values and seven were osteopenic. Severe periodontitis was observed in 33 subjects, out of whom eight had normal BMD values, 12 were osteopenic and 13 subjects suffered from osteoporosis. The results suggest that, as the severity of periodontitis increased the level of osteoporosis also increased. The findings of present study are similar to the studies conducted by Habashneh et al., Reinhardt et al., Aspalli et al., [4,14,15]. The results were contradictory to studies conducted by Pilgram et al., Elders et al., Weyant et al., and Lundstrom et al., [6,7,16,17] who showed that there is no definite association between clinical attachment level and BMD. The differences observed in the present study may be attributed to inclusion of younger age group in previous studies.
In the current study, slight periodontitis was observed in eight subjects and all had high plaque index score. Moderate periodontitis was observed in 24 subjects, of which nine had low plaque score and 15 had high plaque score. Thirty three subjects had severe periodontitis, of which five had low plaque score and 28 had high plaque index score. As the PI score increased, periodontitis also increased from slight to severe, indicating significant association between plaque index and periodontitis. The results of present study are concurrent with the studies done by various authors [8,18,19].
In the present study, 33 subjects had normal BMD value, of which seven had low plaque score and 26 had high plaque score. Osteopenia was observed in 19 subjects of which, five subjects had low plaque score and 14 had high plaque score. Osteoporosis was observed in 13 subjects, and all the subjects had high plaque score. There was no statistical significant association between plaque scores and BMD levels. The results are in accordance with Suresh S et al., who did not find any correlation between osteoporosis and PI [11].
Thirty three subjects had normal BMD value of which five had normal BMI, 17 subjects were overweight and eleven were obese. Osteopenia was observed in 19 subjects of whom four had normal BMI, nine subjects were overweight and six were obese. Osteoporosis was observed in thirteen subjects, of which one subject was underweight, four subjects had normal BMI, five subjects were overweight and three subjects were obese. There was no significant association between BMI and osteoporosis, in the present study. The results of present study were contradictory to studies done by Felson et al., and Nguyen et al., who stated that overweight and obese females were more likely to have osteoporosis and osteopenia [20,21]. The differences observed may be because in the current study sample included both the genders whereas previous studies considered only female subjects.
Slight periodontitis was observed in eight subjects of whom one subject had normal BMI, six were overweight and one was obese. Moderate periodontitis was observed in twenty four subjects of whom three had normal BMI, 13 were overweight and eight were obese. Severe periodontitis was observed in 33 subjects of whom one was underweight, 9 had normal BMI, 12 were overweight and 11 were obese. BMI did not correlate with periodontitis; this finding is in accordance with the study conducted by Snophia S et al., Kim et al., [11,22]. The findings were contradictory to the studies conducted by various other authors [20,23,24], these differences may be due to younger age group of subjects considered in the previous studies.
Limitation of the Study
The limitation of the present study is that we considered less sample size and did not include participants from all age groups.
Conclusion
The findings of our study revealed that the severity of osteoporosis increased with increasing severity of periodontitis. Within the limitations of this study, we can thus conclude that periodontitis may be a risk indicator for osteoporosis.
Furthermore, longitudinal studies would be valuable to establish the temporal association between systemic and oral bone loss. Therefore, future research should continue to evaluate specific association between osteoporosis and periodontitis and include subpopulations that are at higher risk. This knowledge may form the basis for targeting preventive and therapeutic measures for individuals who are at greatest risk for both the diseases. Physicians should understand the potential relationship between systemic BMD and periodontal status, so as to educate patients about their oral disease risk factors and reinforce the benefits of healthy lifestyle.
* Correlation was statistically significant (p ≤ 0.05)
* Correlation was statistically significant (p ≤ 0.05)
¶ Correlation was not statistically significant (p≥ 0.05)
¶ Correlation was not statistically significant (p≥ 0.05)
¶ Correlation was not statistically significant (p≥ 0.05)