The restoration of masticatory function and aesthetics is an important aim in dentistry mainly when patients present with extensive tooth loss. The loss of tooth in elderly patients not only impairs the stomatognathic system but also their psychological status and quality of life [1,2]. The important criteria’s for the success of dentures are patient’s expectations and the ability of the denture to replace the lost masticatory efficiency. For long polymethyl methacrylate (PMMA) has dominated the field of denture base materials but today flexible dentures have emerged as a major competitor to PMMA dentures. Flexible dentures, also known as nylon dentures, are considered perfect alternatives to conventional and partial acrylic dentures. Flexible dentures made of thermoplastic material, are resistant to breakage and very comfortable for the edentulous patients. These dentures are easy to wear and very pleasant for patients as they are much thinner, stay firmly in place and more retentive when compared to conventional dentures. They do not cause any allergic reactions, are light in weight and take minimum space in the oral cavity. Further studies have proved that these flexible dentures have less solubility and sorption values than heat cure PMMA [3,4].
Though widely used for partial dentures the flexible material is not usually used for complete dentures. The criteria of better masticatory performance and masticatory efficiency of dentures may change the future prospective of denture base materials. Thus, it is of utmost importance to study the masticatory performance and masticatory efficiency in cases of rehabilitation with the flexible dentures for elderly individual for detailed diagnosis and prognosis, which will improve their quality of life.
The null hypothesis to be tested in this study was that there was no difference in masticatory performance and masticatory efficiency of patients treated with complete dentures made with high impact PMMA resins and flexible thermoplastic material.
This study aimed to evaluate and compare differences in masticatory efficiency of patients treated with complete dentures made with high impact resins and flexible resins.
Materials and Methods
This cross-sectional, prospective study was conducted at Peoples College of Dental Sciences and Research Centre, Bhopal in 2013. The study group comprised of randomly selected 10 completely edentulous patients (6 males & 4 females) reported to the Department of Prosthodontics. The inclusion and exclusion criteria’s were as follows:
Inclusion Criteria
Only healthy edentulous patients and denture wearers for the first time were included in the study. Patient’s ages were between 45-65 years. Patients were advised orthopantomographs to rule out hard tissue abnormalities and Temporomandibular Joint (TMJ) dysfunctions. The nature of the study was explained and an informed consent was taken from the patient.
Exclusion Criteria
Patients with history of temporomandibular disorders such as Myofacial Pain Dysfunction Syndrome (MPDS), trismus, trauma, dislocation, ankylosis and with poor control of systemic diseases such as haematological, cardiovascular and renal disorders, autoimmune/endocrinological disorders, compromised oral conditions, local lesions, resorbed or flabby ridges and edentulous period less than three months.
Selection bias was removed by selecting various subjects randomly who fulfilled the inclusion and exclusion criteria’s and with same systemic conditions. After consultation from statistician the sample size was taken as ten subjects for the pilot study. The informed consent was obtained from the subjects participating in the study, and ethical clearance was obtained from Institutional Ethical Committee to carry out the study. The study was carried over a period of eight months.
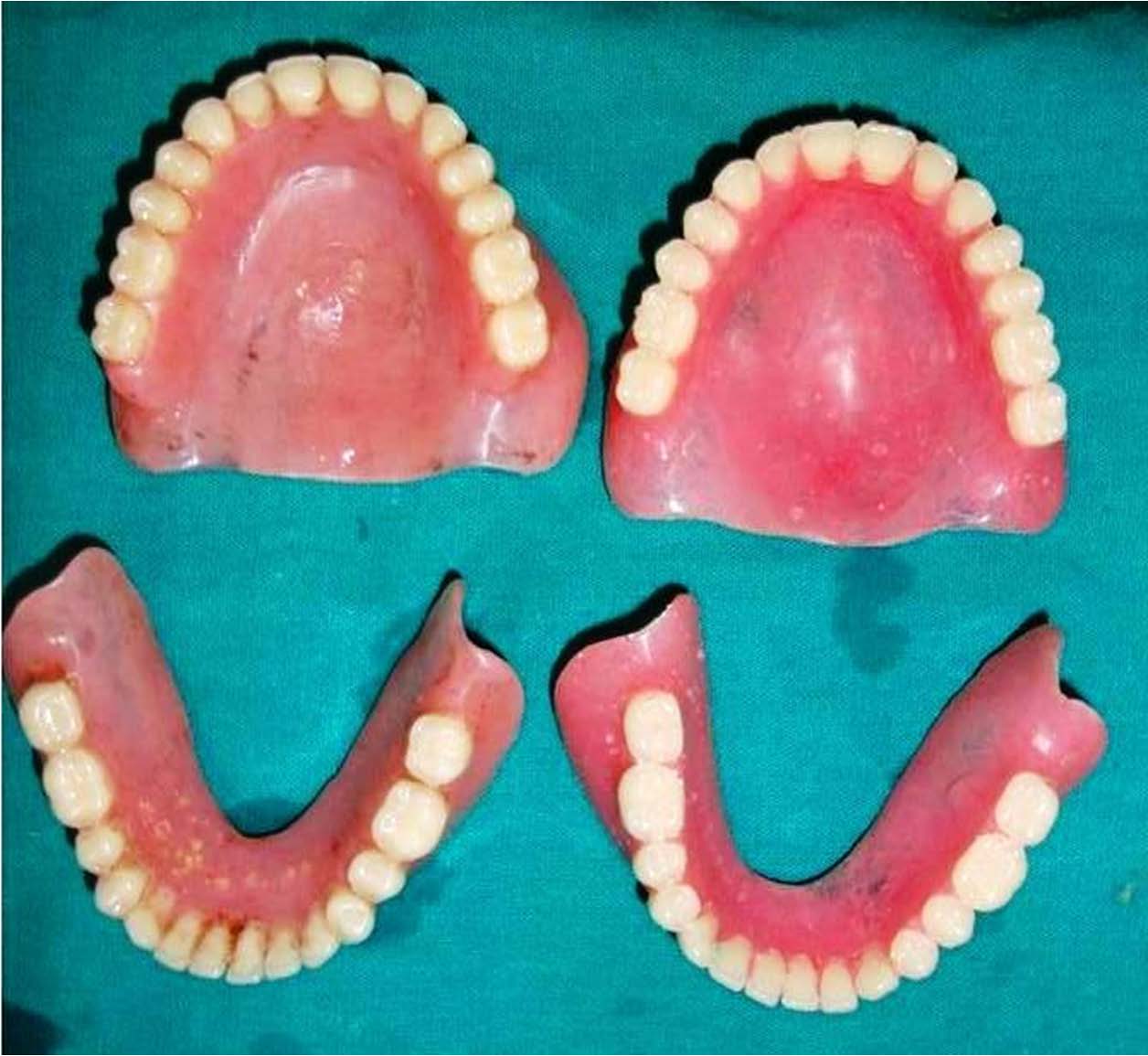
For each patient two sets of complete denture were fabricated. Initially all the subjects were given Conventional High Impact dentures (Group-1) for three months and there masticatory performance was evaluated. Later the conventional high impact dentures were withdrawn and all the subjects were given Flexible denture (Group-2) for three months and there masticatory performance was again evaluated.
The first set of denture was made by conventional method following the standardized denture fabrication protocol. The second set of denture was made by duplication of master cast and jaw relation as follows. Using condensation silicone of putty consistency (Zermack putty, Zetaplus, Badia Polesine, Rovigo, Italy) and Hanau flasks the master casts of each patient were duplicated, and poured in Type III Dental stone (Gyprock, Rajkot, India).Face bow transfer was made using Hanau Springbow and jaw relations were recorded. Extra oral tracing was done to verify the tentative centric jaw relation. Interocclusal plaster records, for centric and protrusive relation were made for programming the articulator (Hanau H2). With the help of putty indexes and plaster indexes the duplicated casts and occlusal rims were mounted in the same spatial relationship as they were mounted on the articulator after gothic arch tracing for the first set of denture. Three putty indexes were made. First and second indexes were made for the duplication of the maxillary and mandibular occlusal rims and third index for the entire frontal surface of the maxillary and mandibular occlusal rims to duplicate the over jet and overbite relation. Next, using mounting jig of the articulator two plaster indexes were made with three acrylic stops [Table/Fig-1] to mount the duplicated maxillary and mandibular cast in the same spatial relationship as the original maxillary and mandibular casts were mounted. Teeth arrangement for both the set of dentures was done using Acry Rock teeth sets (Ruthinium Dental Products (P) Ltd, Italy) in balanced occlusion. Try in of the waxed up dentures was done. High Impact Polymethyl Methacrylate resin (Trevalon Hi, Dentsply India Pvt. Ltd Haryana, India) was used to fabricate the conventional dentures using conventional flasking and compression molding technique. Denture insertion of the conventional denture was done. First patient recall was done after 24 hours. Patients were recalled after three months for masticatory efficiency estimation. After withdrawal of conventional dentures, the second set of flexible dentures were fabricated using co-polyamide nylon resin (Lucitone FRS Dental Resin, Dentsply India Pvt. Ltd, Haryana, India) using success injection molding system (Dentsply, Milford, USA) and given to patients after one week and patient was recalled after three months for masticatory efficiency estimation.
First mounting jig with three acrylic stops for duplication of orientation jaw relation

The objective and subjective evaluation of masticatory function was done by chewing tests and questionnaire [Table/Fig-2] respectively. In order to eliminate experimental bias stratified randomization was carried out. In order to avoid inter examiner variability data were collected by a single examiner who participated in the calibration process, which was done by theoretical discussions and practical activities.
Patient’s satisfaction Questionaire.
| Grading Criteria for denture satisfaction- 1 to 3 (1-Poor , 2-Average, 3 -Good) Assessment by the Doctor: |
|---|
| Question | Group1 | Group2 |
|---|
| Esthetics | | |
| Retention of maxillary dentures | | |
| Retention of mandibular dentures | | |
| Speech | | |
| Assessment by the Patient: |
|---|
| Question | Group1 | Group2 |
|---|
| Esthetics | | |
| Retention of maxillary dentures | | |
| Retention of mandibular dentures | | |
| Speech | | |
| Chewing efficiency with soft food | | |
| Chewing efficiency with medium food | | |
| Chewing efficiency with hard food | | |
| Comfort of maxillary denture | | |
| Comfort of mandibular denture | | |
| Overall satisfaction | | |
Group 1-Polymethyl Methacrylate Dentures, Group 2- Flexible Dentures
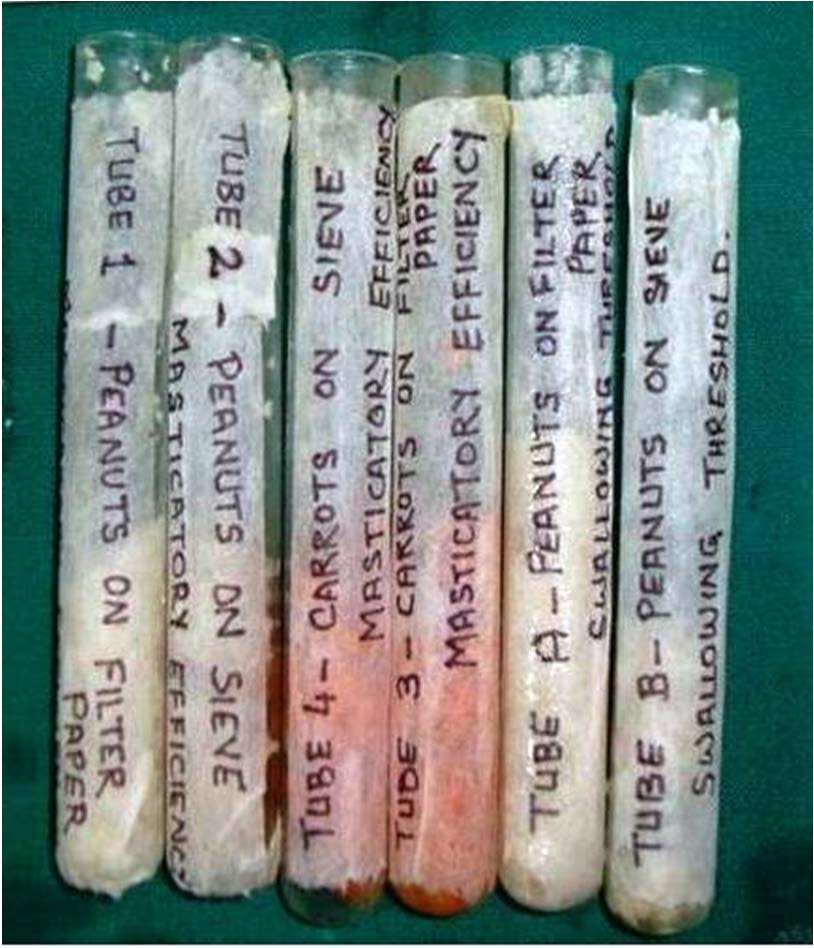
For chewing tests, each subject were instructed to chew the portion of test food, twenty strokes for peanuts and forty strokes for raw carrots [5]. For estimating the masticatory performance three grams of nuts and five grams of carrots were used. After the specified number of chewing strokes, the chewed food was collected in a disposable cup. The subjects were instructed to rinse their mouth twice and the rinse obtained was also added to the same disposable cup. After stirring the chewed food with a glass rod it was poured on a brass sieve. To measure the swallowing threshold, each subject was instructed to chew a test portion of food (3gms of peanuts) until it was ready for swallowing, without specifying side or number of chewing strokes. When the subject considered the food sufficiently chewed for swallowing, the food was expectorated into a cup and the mouth rinsed twice with water to recover the entire test sample. The recovered chewed food was subjected to the sieve analysis described above, and masticatory performance ratios were calculated. This test helps to determine the qualitative estimation of the chewed food before swallowing. The filtered food particles on the filter paper and on the sieve were collected in borosilicate glass test tubes (Borosil, Mumbai, India) [Table/Fig-3] and the tubes were centrifuged (Centrifuge-5804-R, Eppendorf, Germany) for 3 minutes at 1,500 rpm [Table/Fig-4]. The weight of the test material (sediment) in each tube was recorded using digital weighing machine (Axis, AGN 204-PO, Max-200g, d-0.0001g, India). Masticatory performance in this study has been quantitated in the method suggested by Yurkstas and Manly [6]. Performance was evaluated for any particle size (sieve size) by dividing the weight of test food passing through a sieve (of a given mesh) by the total weight of test food recovered. This fraction was then expressed as percent. First wet weight was calculated. The test specimens were placed in a desiccator (Concentrator Plus, Eppendorf, Germany) for 2 hours [Table/Fig-5] and again the dry weights were measured. This test was carried out for both the sets of denture after an adjustment period of three month [Table/Fig-6].
Test tubes with test specimen

Vacuum concentrator (Dessicator)

Vacuum concentrator (Dessicator)
To compare the masticatory efficiency of both the sets of dentures the time and number of masticatory strokes were calculated. The set of denture requiring less time and less number of masticatory strokes for complete mastication of food had a better masticatory efficiency. The patient’s satisfaction such as retention, stability, comfort, and aesthetics were assessed by means of a questionnaire.
Statistical Analysis
Data were analysed using a statistical package program, SPSS version 18.0 (IBM, India, trial version). The statistical analyses were performed using Z-test of Proportion to find out patient satisfaction with both group of dentures and Paired t-Test to determine the differences between the mean values of both the groups of dentures.
Chewing efficiency using carrots and peanuts can be calculated from the formula
Where P is performance ratio, 103 is constant, and 1.2 the slope of the norm. The chewing efficiencies for various performance ratios for peanuts, was read directly from table by Manley RS [6].
Results
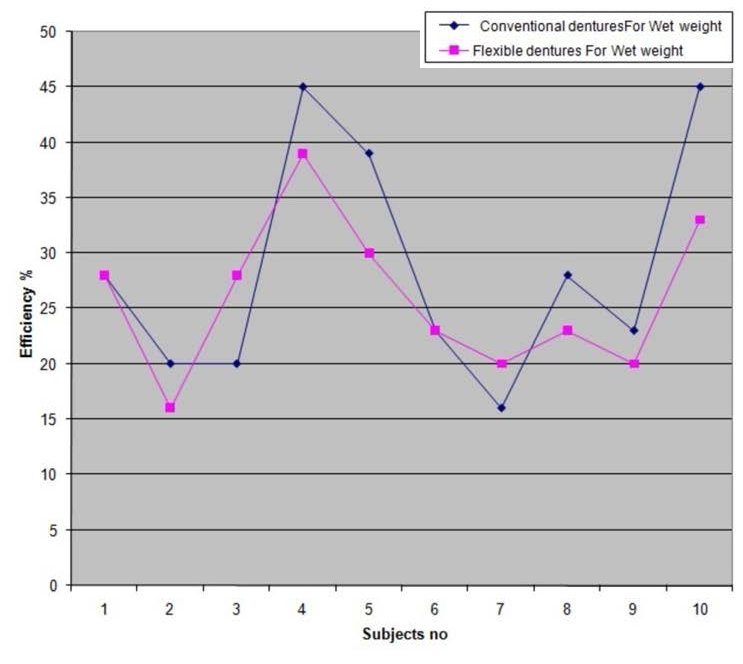
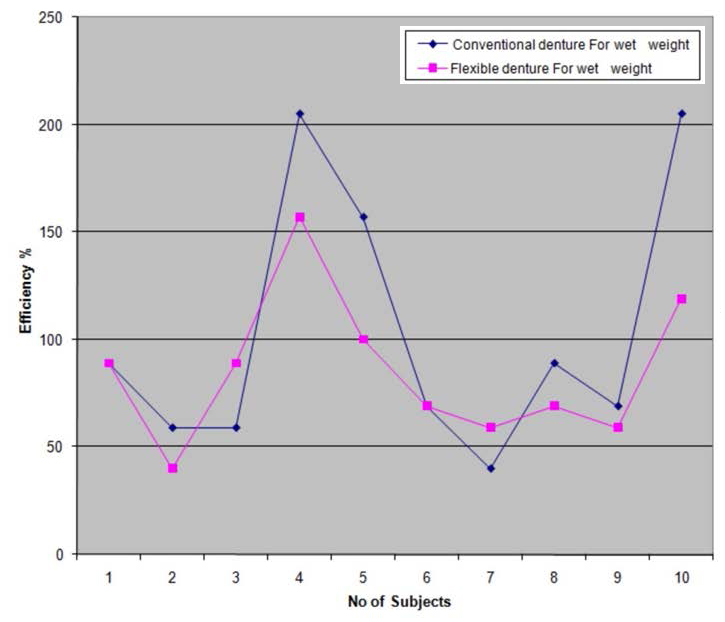
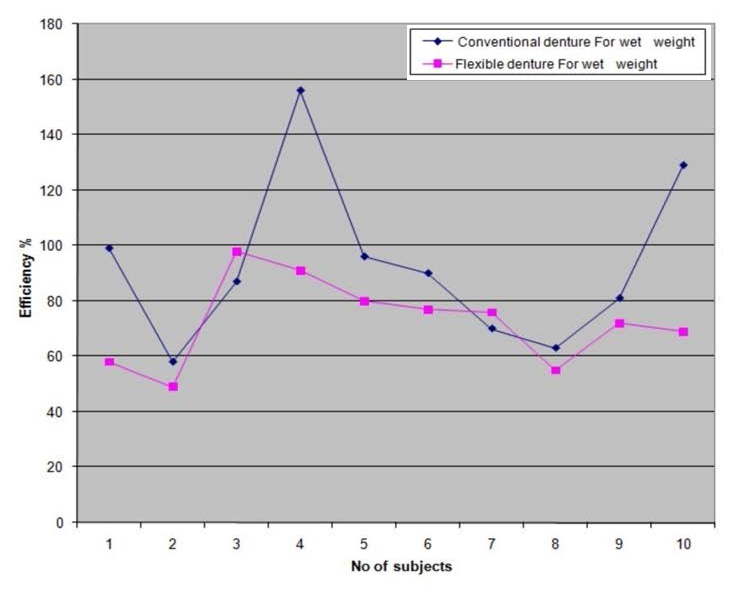
According to the results of our study [Table/Fig-7], the mean values of wet weights for soft food, for conventional dentures was 0.39842 and for flexible dentures was 0.37559.The t-value was 1.1705 and p-value was 0.2719. There was no significant difference between both groups at 5% level of significance. Mean values for masticatory performance of wet weights for hard food, for conventional dentures was 0.47661 and for flexible dentures was 0.36345.The t-value was 3.17 and p-value was 0.0112. There was significant difference between both groups at 5% level of significance. Mean values of dry weights for soft food for conventional dentures were 0.36389 and for flexible dentures were 0.35021.The t-value was 0.6669 and p-value was 0.5216. There was no significant difference between both groups at 5% level of significance. The mean values of dry weights for hard food for conventional dentures were 0.43789 and for flexible dentures were 0.32453.The t-value was 2.5610 and p-value was 0.0306. There was significant difference between both groups at 5% level of significance. The test group showed no statistically significant difference for masticatory performance calculated by swallowing threshold of peanuts between the two groups in wet weight (t-value0.3709, p-value 0.7193) and dry weight (t-value 0.5533, p-value 0.5936).Further the test groups showed no statistically significant difference in time, total number of masticatory strokes and the rate of masticatory cycles. Following the denture and dentition norms, for peanuts, the line diagrams showed a trend towards higher masticatory efficiency for conventional high impact dentures [Table/Fig-8,9]. According to denture norms for carrots, the line diagram showed a higher masticatory efficiency values for conventional high impact dentures [Table/Fig-10]. The questionnaire was analysed using the z-test of proportion. It was found that the aesthetics and retention of the mandibular dentures was significantly more for the flexible dentures. Patient experienced aesthetics, comfort, retention of mandibular dentures and overall satisfaction with the dentures more for flexible dentures. Factor such as chewing efficiency with hard food was more for conventional denture [Table/Fig-11].
| Component | Mean±Standard Deviation | N¦ | t –value | df** | p- value (5% Level) | Confidence interval (95% level) |
|---|
| Masticatory performance [wet weight] | *Group-1 Peanuts | 0.39842±0.108021 | 10 | 1.1705 | 9 | 0.2719§ | -0.0212 to 0.0669 |
| †Group-2 Peanuts | 0.37559±0.071501 | 10 |
| *Group-1 Carrots | 0.47661±0.10911 | 10 | 3.1774 | 9 | 0.0112‡ | 0.0325 to 0.1937 |
| †Group-2 Carrots | 0.36345±0.11708 | 10 |
| Swallowing threshold [wet weight] | *Group-1 Peanuts | 0.67738±0.124438 | 10 | 0.3709 | 9 | 0.7193 § | -0.0645 to 0.0898 |
| †Group-2 Peanuts | 0.66472±0.127126 | 10 |
| Masticatory performance [dry weight] | *Group-1 Peanuts | 0.36389±0.10030 | 10 | 0.6669 | 9 | 0.5216 § | -0.0327 to 0.0600 |
| †Group-2 Peanuts | 0.35021±0.07785 | 10 |
| *Group-1 Carrots | 0.43789±0.12623 | 10 | 2.5610 | 9 | 0.0306 ‡ | 0.0132 to 0.2134 |
| †Group-2 Carrots | 0.32453±0.11239 | 10 |
| Swallowing threshold [dry weight] | *Group-1 Peanuts | 0.66214±0.13257 | 10 | 0.5533 | 9 | 0.5936 § | -0.0789 to 0.1300 |
| †Group-2 Peanuts | 0.63659±0.10326 | 10 |
| Time in seconds for complete mastication of test food[3gms of peanuts] | *Group-1 | 63.4±11.98 | 10 | 0.6347 | 9 | 0.5414 § | -12.78 to 7.18 |
| †Group-2 | 66.2±13.55 | 10 |
| No of masticatory strokes for complete mastication of test food[3gms of peanuts] | *Group-1 | 70.7±13.86 | 10 | 1.8196 | 9 | 0.1022 § | 12.56 to 1.36 |
| †Group-2 | 76.3±17 | 10 |
| Rate of masticatory cycles for complete mastication of test food[3gms of peanuts] | * Group-1 | 0.90±0.126068 | 10 | 0.9329 | 9 | 0.3752 § | -0.0457 to 0.1100 |
| †Group-2 | 0.87±0.093044 | 10 |
‡p>0.05 there was no significant difference between groups § p<0.05 there was significant difference between groups
* Group1- Conventional High Impact Polymethyl Methacrylate dentures; †Group2-Flexible dentures; ‡Significant difference; § No significant difference; ¦ Number of patients; **degree of freedom
Masticatory efficiency according to dentition norms for wet peanuts
+Masticatory efficiency according to denture norms for wet peanuts
Masticatory efficiency according to denture norms for wet carrots
Z-test of proportion for patient satisfaction (subjective evaluation).
| Satisfaction Factors | Group | Satisfaction response as poor by number of subjects | Satisfaction response as Average by number of subjects | Satisfaction response as Good by number of subjects |
|---|
| Esthetics | Group-1 | 3 | 5* | 2 |
| Group-2 | 0 | 3 | 7* |
| Retention of maxillary dentures | Group-1 | 0 | 3 | 7* |
| Group-2 | 0 | 1 | 9* |
| Retention of mandibular dentures | Group-1 | 3 | 4 | 3 |
| Group-2 | 1 | 3 | 6* |
| Speech | Group-1 | 0 | 9* | 1 |
| Group-2 | 0 | 7* | 3 |
| Chewing efficiency with soft food | Group-1 | 0 | 2 | 8* |
| Group-2 | 0 | 4 | 6* |
| Chewing efficiency with medium food | Group-1 | 1 | 4 | 5 |
| Group-2 | 3 | 4 | 3 |
| Chewing efficiency with hard food | Group-1 | 1 | 3 | 6* |
| Group-2 | 3 | 5* | 2 |
| Comfort of maxillary denture | Group-1 | 0 | 4 | 6* |
| Group-2 | 0 | 1 | 9* |
| Comfort of mandibular denture | Group-1 | 0 | 7* | 3 |
| Group-2 | 0 | 2 | 8* |
| Overall satisfaction | Group-1 | 0 | 6* | 4 |
| Group-2 | 0 | 3 | 7* |
Group-1= Conventional High Impact dentures; Group-2= Flexible denture
*Indicates higher response by subjects in that group
As there was a statistically significant difference in masticatory performance for hard food between the two groups the null hypothesis was rejected.
Discussion
The majority of the tests developed so far for measuring masticatory performance and efficiency of dentures depend on the fractional sieving of the chewed food [7,8]. In our study we have also used the single volumetric sieving method. Single sieve method is certainly a convenient and reliable method to be used clinically. For the estimation of chewing performance with peanuts (soft food) a mesh sieve of 10 numbers (U.S. standard sieves) and for carrots (hard food) 5 number mesh sieve was used [9–11]. The better the food chewed before swallowing more will be the filtered particles, and more will be the masticatory efficiency [12–14]. There was no distinction of sex in our study, as studies prove that no gender differences in bite force and masticatory performance were found among complete denture wearers [1]. In this study the adjustment period for each denture were taken as three months. This time period is considered sufficient for denture adaptation by the patient [15].
A statistically significant number of patients found the flexible dentures to be more satisfying and comfortable than the conventional dentures. These results were in accordance with the study conducted by Dhiman RK [16]. These findings may again be attributed to the basic nature of the denture base materials. The same was suggested by Marcelo Coelho Goiato et al., in their study [17].
Al-Jammali ZMJ [18] in their study found that the flexible partial denture provide better chewing efficiency than heat cure acrylic partial denture, the masticatory performance was higher for flexible partial denture than heat cure acrylic partial denture but contradictory to the above study the results of our study showed that conventional dentures were more efficient for mastication with hard test food in comparison to the flexible dentures. These results can be attributed to the basic nature of the two denture base materials. The conventional dentures provide a firm denture base, deform and flex minimum during function and provide hard surfaces for the grinding of food [19,20]. The result was in accordance with study by Shah J et al., [4] were flexible resin demonstrated lower hardness values and also possessed lower amounts of cross-linking agents, which may affect surface hardness. As there was no statistically significant difference for masticatory performance of soft food between the conventional and flexible dentures, these flexible dentures with diet modification can be a better alternative to conventional dentures in patients with repeated midline fracture of denture, allergic to PMMA and denture sore mouth [3,16].
Clinical Implications
The flexible dentures are much thinner than conventional dentures, are more aesthetically pleasing and easily acceptable to the patient. They can be given as a substitute to patients allergic to PMMA. As they are lightweight and flexible they can be successfully given to patients with bony undercuts. The flexibility of the material provided a certain degree of stress-breaking effect and there was no denture sore-mouth [21–23].
Conclusion
Based on the study conducted it may be concluded that there was statistically significant difference for masticatory performance in wet and dry weight values of hard food, but there was no statistically significant difference for masticatory performance in wet and dry weight values of soft food between the conventional and flexible dentures. The subjective evaluation pointed towards better aesthetics, comfort, retention and overall satisfaction for flexible dentures.
‡p>0.05 there was no significant difference between groups § p<0.05 there was significant difference between groups
* Group1- Conventional High Impact Polymethyl Methacrylate dentures; †Group2-Flexible dentures; ‡Significant difference; § No significant difference; ¦ Number of patients; **degree of freedom
Group-1= Conventional High Impact dentures; Group-2= Flexible denture
*Indicates higher response by subjects in that group