A Unique Bonding Technique for Immediate Orthognathic Surgery
Biswas Palikunnu Padmaprabha1, Hariprasad Ayinipully2, Rosaline Tina Paul3, Shaji Aboobacker Ponnambathayil4, Althaf Thanimoottil Rasheed5
1 Professor and Head, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India
2 Reader, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
3 Post Graduate Student, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
4 Reader, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
5 Post Graduate Student, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Biswas Palikunnu Padmaprabha, Professor and Head, Department of Orthodontics, Royal Dental College, Palakkad, Kerala, India.
E-mail: biswas_pp@yahoo.co.in
Introduction
A challenge in orthodontics is achieving ideal bracket position which determines treatment results and finishing. A new bonding method is done indirectly on the cast and bonded directly on the teeth, but it does not require conventional trays to carry the brackets to the teeth.
Materials and Methods
Heavy sized archwires like 0.019″x0.025″ or 0.018″ SS are bent to the malocclusion to generate a template which comprises of an Bracket -Archwire Assembly (BAA). This assembly is transferred onto the teeth using the molar bands with tubes which serves as a jig for proper orientation of the BAA, then the adhesive is cured at one shot to complete the bonding procedure.
Results
Two surgical cases successfully bonded with this technique is presented in this article.
Conclusion
This bonding method finds specific advantages in surgical orthodontics – when the surgeon decides on a surgery-first treatment objective, management of single or a couple of periodontally extruded teeth, management of impacted teeth and in patients needing fixed functional appliance immediately before the completion of growth spurt.
Anterior maxillary osteotomy, Bracket archwire assembly, Direct bonding technique, Fixed- functional appliance, Indirect bonding technique, Jigs, Surgery-first treatment option
Introduction
Orthodontic treatment with fixed appliances requires the proverbial “handle on the teeth” to enable a force system to be applied on to the teeth. An accurately positioned bracket minimizes future archwire bends and the need for bracket repositioning.
In 1972, Silverman et al., were the first to publish an article on indirect bonding (IDB) technique [1]. Indirect bonding is defined as a technique in which the brackets are attached to the teeth on the patient's models, transferred to the mouth with some sort of tray into which the brackets become incorporated, and then bonded onto the teeth [2]. Most of the IDB trays described in the literature use vacuum-formed thermoplastics, silicone impression materials, or a combination of both [3].The other method of bonding being the direct bonding technique in which the bracket is directly bonded to the tooth. Both these methods have advantages and disadvantages [4–6].
A new method of bonding is described were heavy sized archwires like 0.019″x0.025″ Stainless Steel (SS) or 0.018″ SS are bent to the malocclusion with the brackets engaged on it. The archwire with the brackets serve as templates for the intraoral direct bonding method. The stepwise bonding technique will be described in detail.
Aim of the Study
To elaborate a stepwise procedure of a new bonding technique. The routine format of bonding and placing the surgical wires, would take a period of 6-8 months, a new method of bonding was designed to enable us to post a surgical patient immediately for surgery.
Materials and Method
Laboratory procedure
A well adapted molar band was transferred onto an alginate impression which is poured immediately [Table/Fig-1].
Vertical and horizontal orientation lines were drawn on the study models to help in accurate bracket positioning [Table/Fig-2].
Initially, a 0.019″x0.025″or a 0.018″ stainless steel wire was gradually bent into the archform with an incisor bracket engaged onto the archwire with an elastic module.
Successively, appropriate 1st and 2nd order bends were made on the archwire and gradually all the brackets were fixed onto the archwire with elastic modules. The brackets along with the archwire remained passively on the labial surface of the teeth on the model as the archwire was bent to the malocclusion of the dental arch. The archwire with brackets were then inserted into the tubes on the molar bands [Table/Fig-3].
The tubes act as jigs for the accurate positioning of the bracket with archwire assembly on the labial surface of the model.
The archwire with brackets and the molar bands were carefully removed from the model and was ready for fixing intraorally [Table/Fig-4].

Vertical and horizontal orientation lines

Bracket-archwire assembly fabrication (0.018″ss)

Upper and lower 0.018″ SS archwires bent to the malocclusion ready for bonding

Chair –side procedure
After proper oral prophylaxis, the bands were cemented on the molars. The tubes on the molars now acted as a guide for the proper orientation of the archwire and bracket assembly on the tooth surface.
Teeth are etched and primer applied.
Adhesive was placed on the base of the brackets.
The archwire and the brackets with composite was inserted into the tubes on the molar bands. After verifying the correct positioning, excess flash was removed and cured [Table/Fig-5].
A similar procedure is performed in the mandibular arch.
The patient is then posted for surgery.
Archwire and brackets with adhesive in position

Here are two case reports where this new bonding method which was employed.
Case I: (0.018″ SS)
A 25-year-old male patient having a skeletal bimaxillary protrusion with a gummy smile and an increased lower anterior facial height was to undergo an anterior maxillary osteotomy with a superior repositioning and a posterior set back, combined with mandibular subapical setback. As per the surgeons preference it was decided to strap up with this innovative bonding technique and an 0.018″ SS wire with minimal bends in the buccal sections in the upper and lower arches so that the archwire would guide the surgeon to set back the anterior segments by sliding back the wire through the tube posteriorly [Table/Fig-3,4,5,6,7,8].
Pre-surgical bonding completed (Note the first bicuspids were not bonded as they were indicated for extraction on the table)

Immediate postoperative–precise set-back of anterior segments after sliding the archwires through the bicuspid bracket and the molar tubes

Sliding the wire through the tubes during setback
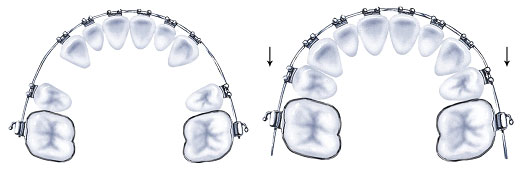
During surgery, the upper and lower anterior segments were repositioned posteriorly by sliding the wire through the second bicuspid bracket and molar tubes and the distal ends were cut and cinched back. This prevented lateral canting and antero- posterior tipping of the anterior segment with precise repositioning three dimensionally. The patient was followed up after the surgery, was put on aligning wires initially and routine MBT mechanics was followed till finishing and detailing was completed [Table/Fig-7].
Case II: (0.019″x0.025″SS)
A 21-year-old female with a gummy smile of 8mm, increased lower anterior facial height by 14mm, having a prognathic maxilla and a retrognathic mandible was to undergo a Le Forte I superior repositioning and an advancement genioplasty. It was decided to post the patient immediately for surgery without any dental decompensation on a surgery first basis. So the above mentioned procedure for bonding was followed with 0.019″x0.025″ stainless steel archwires that was bent to the malocclusion, and the patient was posted for surgery immediately [Table/Fig-9,10]. The patient was followed up with regular post-surgical orthodontics using the MBT mechanics.
Upper and lower 0.019″x0.025″ stainless steel arch wires which are bent to the malocclusion with brackets fixed with elastic modules

Indirect bonding done using (0.019″ x 0.025″) stainless steel posted archwires

Discussion
Branden et al., conducted a study which suggested that indirect-bonding provide similar bond strength in vitro as direct bonding [1]. Klocke et al., conducted a study on indirect bonding method using custom-made brackets and proved that the bond strength was superior to bonding with conventional brackets [2]. Our bonding technique did not require indirect bonding trays or custom-brackets and so involves only a simple lab procedure. Precise and well adapted positioning of the brackets was accomplished as the bracket positioning was done extra-orally. Moreover, voids were not entrapped beneath the bracket base, as finger pressure was applied onto the brackets directly.
It is a standard procedure to carry out the dental decompensation with fixed orthodontics before any orthognathic surgery. To add, the fixed orthodontic appliance present at the time of surgery, helps the surgeon in the application of elastics postoperatively to attain a good occlusion. However, the process of decompensation, depending on the malocclusion, is time consuming and would extend for a period of 6 months to 1 year as the case may be. In orthognathic surgery, the trend these days is “surgery first” implying that orthodontic corrections could be performed post surgically. But even in these situations the surgeon usually prefers the orthodontic appliance on, the only other alternative being arch bars. Needless to say, arch bars have their own disadvantages and are cumbersome to handle. Moreover, if tooth movement is required immediately after surgery, appliance placement is not possible due to restricted mouth opening and perioral oedema [3].
Even, when the surgeon decides for a “surgery first” option, the orthodontic treatment would take a minimum of 4-6 months to get into heavy sized (0.019″x0.025″SS) surgical archwires required for the surgery [3]. This waiting period is eliminated when this unique technique of bonding is adopted. Thus, it has the greatest advantage of posting the patient instantly for orthognathic surgery with heavy sized surgical archwires in place.
Other advantages of this bonding technique are that it does not require indirect bonding trays and so involves only a simple lab procedure, excess flash is easily removed and the bracket placement is precise and well adapted to the surface of the tooth. Finally, as the teeth are not being moved and since the heavy sized archwires are passive, the patient is relieved of the pain that usually occurs during the initial phase of active orthodontic therapy with initial aligning archwires.
In a condition where a single tooth is extruded and is periodontally compromised, according to Berte Melson applying an intrusive force using nitinol wires would be hazardous, since along with an intrusive force on the extruded tooth, the adjacent teeth subsequently experience an extrusive effect. Even if continuous archwires has to be used for intrusion of the extruded tooth, a series of archwires has to be changed taking a reasonable period of time. This method of bonding helps us to instantly generate the desired intrusive force without the undesirable extrusive forces on the adjacent teeth. This could be done by placing heavy 0.019″x0.025″ stainless steel archwires with an elastomeric engaged onto the extruded tooth [4].
When teeth are impacted and there is adequate space for its eruption, according to Nanda, immediate placement of a heavy-sized archwire by using this technique would enable us to considerably save treatment time, by eliminating the aligning phase of fixed orthodontic therapy. Moreover, by using heavy- sized arch-wires, the tipping tendency of the adjacent teeth which would lead to a lateral open bite is nullified [5].
While treating an adolescent patient needing growth modification using any of the fixed functional appliances demands a heavy archwire to anchor the functional appliance. According to McNamara, the growth modification should be done at the pubertal growth spurt. Advocating this method of bonding is beneficial since immediate placement of the functional appliance is facilitated. Thus, no time is lost in initial aligning wires, and the precious growth spurt period is made use of [6,7]. Usually a torqued wire is used in fixed functional appliance therapy to prevent proclination of anterior teeth. While employing this bonding method, a torque wire cannot be placed, as it would not be possible to fabricate the Bracket Archwire Assembly. To avoid proclining, a 0.021″x0.025″ stainless steel wire could be used in a 0.022″ slot when this method of bonding is used for fixed functional appliance.
Conclusion
This new method of indirect bonding involves a simple lab procedure. Precision and dexterity of the operator to bend wires determines the accuracy in bracket positioning. This method permits the orthognathic patient to be posted immediately for surgery.
[1]. Brandon James Linna, David W, Berzinsb; Virendra B. Dhuruc; Thomas Gerard BradleydA Comparison of Bond Strength Between Direct- andIndirect-bonding MethodsAngle Orthod 2006 76:289-94. [Google Scholar]
[2]. Klocke A, Shi J, Kahl-Nieke B, Bismayer U, Bond strengthwith custom base indirect bonding techniquesAngle Orthod 2003 73:176-80. [Google Scholar]
[3]. Proffit WR, White RP, Sarver DM, Combining surgeryandorthognathics: Who does what, when?In: Contemporary Melson B. Chapter 7- Appliance design. Adult Orthodontics 2012 1st editionUKBlackwell Publishing Ltd:112-15. [Google Scholar]
[4]. Melson B, Chapter 7- Appliance design. Adult Orthodontics 2012 1st editionUKBlackwell Publishing Ltd:112-15. [Google Scholar]
[5]. Nanda R, Biomechanics in clinical orthodontics..Chapter 6- Canine impaction: Diagnosis, treatment plan and clinical managementPennsylvaniaW.B. Saunders Company:102 [Google Scholar]
[6]. McNamara JA, Jr, Bookstein FL, Shaughnessy TG, Skeletal and dental changes following functional regulator therapy on Class IIpatientsAm J Orthod 1985 88:91-110. [Google Scholar]
[7]. Tiziano B, Lorenzo F, Linda RT, James AM, Treatment timing for twin-block therapyAm J Orthod 2000 118:159-70. [Google Scholar]