An Unusual Case of Foreign Body Aspiration Masquerading as Pulmonary Eosinophilia
Nageswara Rao Gopathi1, Venu Mandava2, Prabahkar Rao P.3, Lakshmaikanth Kolaparthy4
1Assistant Professor, Department of Pulmonology, Katuri Medical College, Guntur, Andhra Pradesh, India.
2Assistant Professor, Department of Pulmonology, Katuri Medical College, Guntur, Andhra Pradesh, India.
3Professor, Department of Pulmonology, Katuri Medical College, Guntur, Andhra Pradesh, India.
4Assistant Professor, Department of Peridontics, Sibar Institute of Dental Sciences, Guntur, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nageswara Rao Gopathi, 6-4-96, LIC quarters, 4/2 Arundelpeta, Guntur, Andhra Pradesh-522 002, India.
E-mail: nityanageswar@gmail.com
Foreign body aspiration into the airways is a common occurrence in inebriated conditions, paediatric age group and or loss of cough reflex. Acute symptoms, often times are recognized and medical assistance is sought. Subtle aspirations, unrecognized and stationed for longer time in the abode of airways pose variegated clinical picture. The authors present herewith an unsuspected case of Areca nut in a middle-aged woman mimicking eosinophilic pneumonia.
Areca nut, Foreign body aspiration, Fibreoptic bronchoscopy, RB-rigid bronchoscopy, Oral submucosal fibrosis
Case Report
A 35-year-old female agricultural labour presented to the Pulmonology department, Katuri medical college & hospital, Guntur, India with one year history of shortness of breath, low grade fever, dry cough in the early morning and wheezy chest.
She was not a diabetic and hypertensive. Clinical examination showed pallor, poor oral hygiene, stained teeth and bald tongue. Vitals were stable. Chest examination revealed fixed monophonus rhonchus over right infrascapular area. Other clinical systemic examination was normal. Complete blood picture shows haemoglobin of 7.2 g/dl, leucocyte count of 17,400 cells/ mm3 with 68% neutrophils, 18% lymphocytes and 14% eosinophils. Absolute eosinophil count was 2,430 cells/mm3. She was non reactive for viral markers. Her sputum was negative for acid-fast bacilli and fungal elements. Further Gram’s staining showed plenty of diplococci with pus cells.
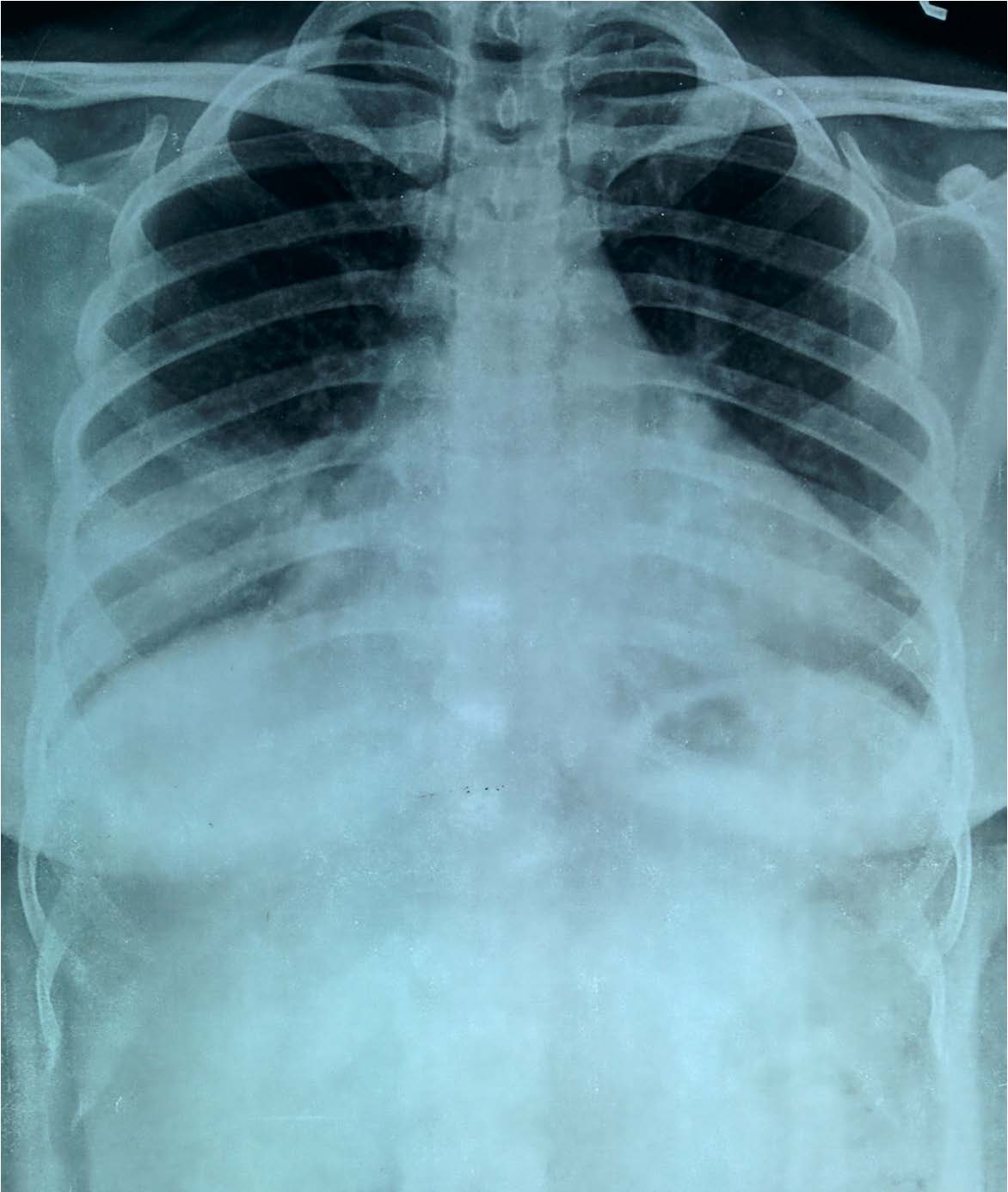
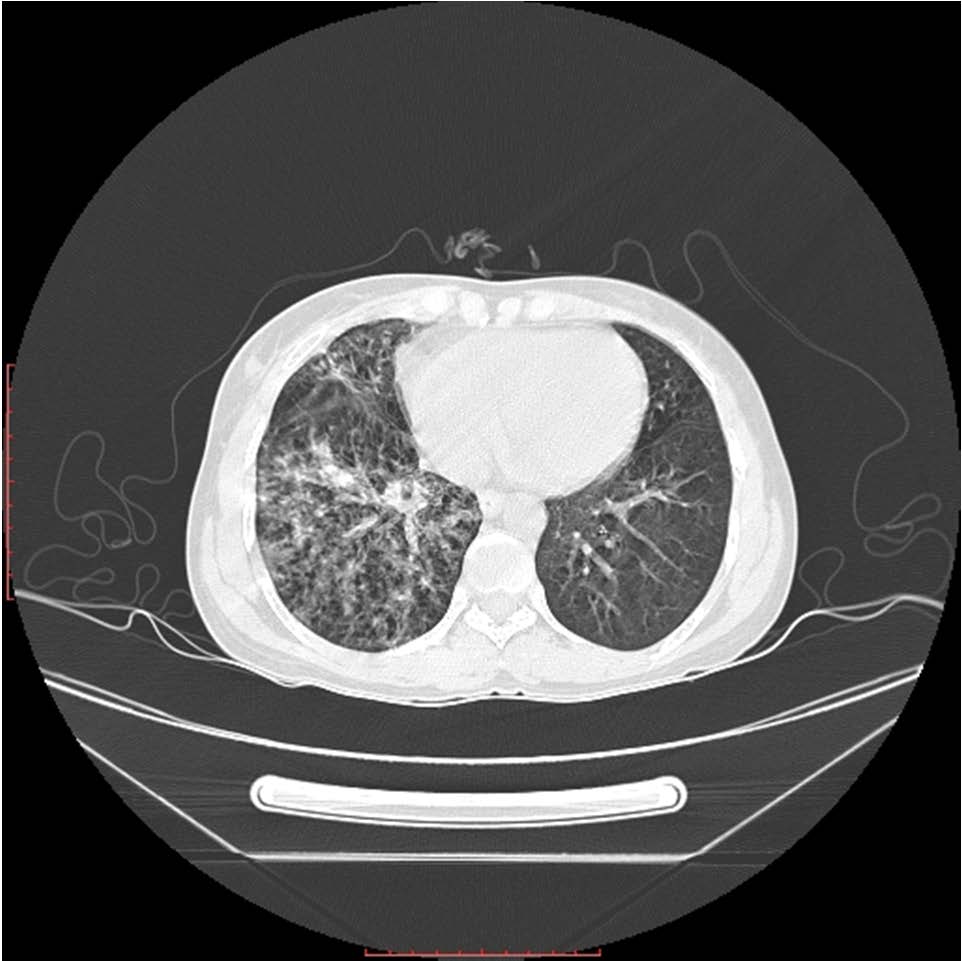
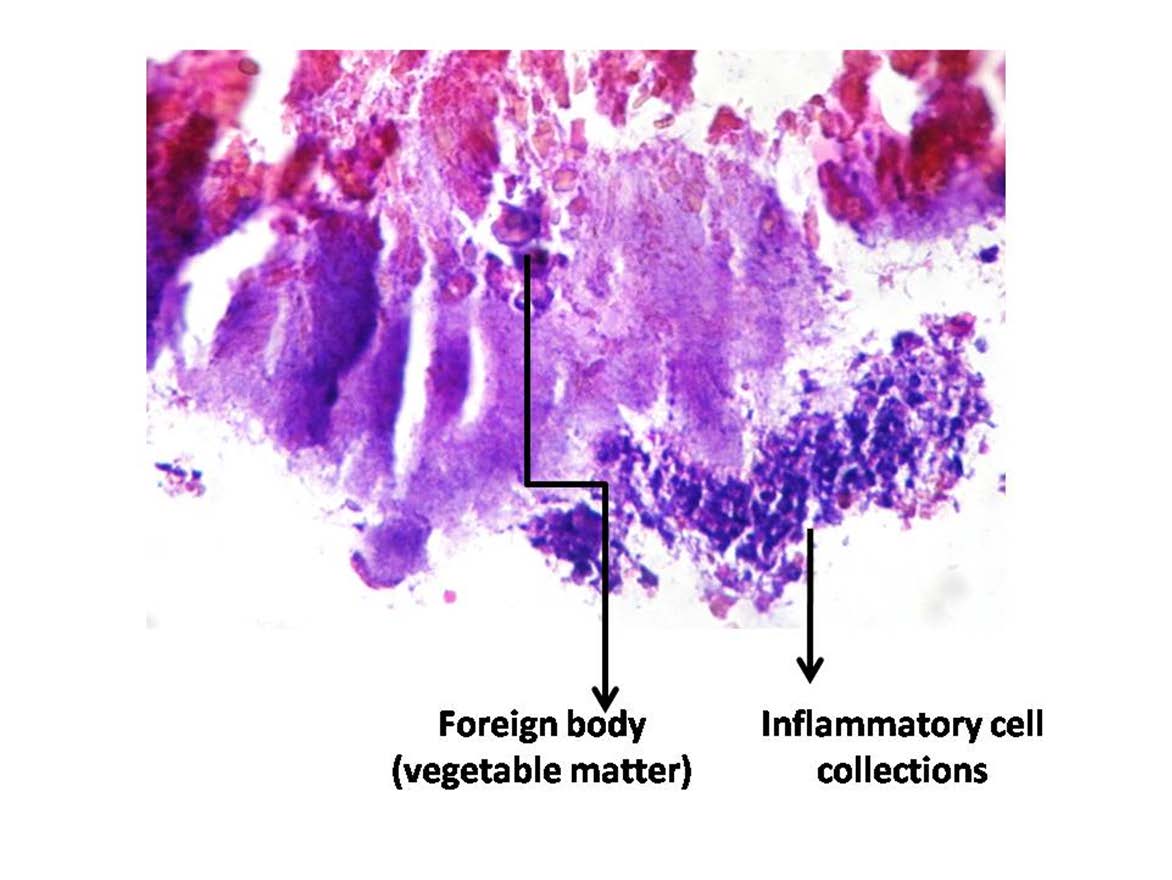
Chest skiagram revealed confluent opacities in the right middle and lower lung zones [Table/Fig-1]. Computed tomography of thorax showed a homogeneous opacity of size 1.5 cm in right lower lobe bronchus with diffuse airspace infiltrates in the right lower lobe suggestive of infection [Table/Fig-2]. The possibilities of super added fungal infection or foreign body aspiration are entertained, as it is a common site for the later. Skin prick test with Aspergillous and Candida species was negative. As the clinical picture was also suggestive of associated bacterial infection, she was treated with a course of cepodoxime-clavulanate. After obtaining written consent, she underwent Fibreoptic bronchoscopy (FOB). The bronchoscopy revealed a brownish, glistening, fixed mass which was covered with thick mucopus in the right superior segment bronchus-B6 [Table/Fig-3]. Rigid bronchoscope was planned at a latter day under general anaesthesia. The foreign body was removed carefully in piece meal from right superior segmental bronchus [Table/Fig-4], haemostasis secured and bronchial toilet was done. Repeat bronchoscopy on the next day showed clearance of obstruction. Gross appearance revealed it as Areca nut. The histopathological examination showed vegetable matter with fibrin deposition and mixed inflammatory cells [Table/Fig-5]. On retrospective history, we noted that she was a habitual betel quid chewer and sleeps with it. Her oral examination too revealed stained teeth, blanched buccal mucosa and depapillised, leathery tongue. She was diagnosed with grade 1-mild oral submucosal fibrosis. She was discharged home with a short course oral steroids, two weeks antibiotics course and haematinics. On follow-up visits, a follow-up chest X-ray and HRCT thorax shows clearing of infiltrates, with subsidence of her symptoms and normalization of eosinophil count.
Discussion
Although foreign body aspiration is uncommon in adults, clinicians must be aware of their likelihood. History of aspiration seems to be the most common predisposing factor [1]. Extra hazard components incorporate injury with loss of cognizance, hidden aspiratory infection, endotracheal intubation, dental surgical methods, psychiatric sickness and narcotic or liquor abuse [1]. The symptoms of FBA can be very vague, ranging from chronic cough, wheeze and dyspnoea to haemoptysis. In cases of long standing and neglected foreign bodies one has to be careful, because of the possibility of complications like pulmonary infections, lung collapse, lung abscesses and malignant transformation [2].
Areca nut is considered to be the fourth most commonly used psychoactive substance after tobacco, alcohol and caffeine and more than 10% of the World’s population chew it regularly more commonly in Asian countries [3]. This widespread habit was associated with aggressive marketing strategies, easy availability and illiteracy. The major constituents of the nut are carbohydrates, fats, proteins, crude fiber, polyphenols, alkaloids and mineral matter [4]. Polyphenols (flavonols, tannins) are responsible for the euphoria and astringent taste of the nut. Alkaloids are the most important biologically active ingredients. There are six identifiable alkaloids viz arecoline, arecaidine, guvacine, guvacoline, nicotine and piperidine. Areca nut extracts enhances the production of tumor necrosis factor-alpha (TNF-α) and interleukin-1, 4 (IL-1, IL-4) in peripheral blood [5]. Arecoline in presence of TNF-α and IL-4, stimulates the production of a chemokine Eotoxin-1 which attracts the Th2 lymphocytes and eosinophils and plays a major role in allergy and asthma [6]. This mechanism may be responsible for the peripheral eosinophilia as seen in this case and is normalized after removal of beetel nut. Areca nut also contains large amounts of copper which is fibrogenic and mutagenic. It is a potent inducer of transforming growth factor-beta (TGF-β) which plays a key role in development of oral submucosal fibrosis [7].
Areca is supposed to be one of the causes of inflammatory and neoplastic conditions of oral mucosa [8], besides being the culprit cause of systemic conditions like obesity, hypertension, diabetes mellitus, metabolic syndrome [3]. Additionally, areca nut chewing assembles the peril of cardiovascular afflictions and finally extends all-reason mortality independent of routine risk factors [9].
Chest X-ray (PA view) showing the right mid and lower zone infiltrates
Computed tomography demonstrating dense airspace consolidation in right lower lobe
Bronchoscopic picture of a betel nut in the right superior segment bronchus (B6) covered with mucopus

Areca nut removed in piece meal on rigid bronchoscopy

Histopathological examination of foreign body revealing it as areca nut (H&E Stain,x100 times)
Conclusion
The case report stresses the importance of history taking. One of the redeeming features of this case is; she did not receive any treatment for pulmonary eosinophilia. Her eosinophilia was an allergic reaction to the Areca nut swallowed into the lungs during sleep. This was removed with Rigid bronchoscopy after relevant investigations.
[1]. F Veyckemans, C Francisn, Tracheo bronchial foreign bodies: presentation and management in children and adultsChest 1999 115:1357-62. [Google Scholar]
[2]. PD Vithalani, H Maniyar, An Overlooked Bronchial Foreign Body in AdultIndian Journal of Otolaryngology and Head, Neck Surgery 2005 57(4):335-37. [Google Scholar]
[3]. Shafique Areca nut chewing and systemic inflammation: evidence of a common pathway for systemic diseasesJournal of Inflammation 2012 9:22 [Google Scholar]
[4]. A Khandelwal, V Khandelwal, MK Saha, S Khandelwal, S Prasad, SG Saha, Prevalence of areca nut chewing in the middle school-going children of Indore, India Contemporary Clinical Dentistry 2012 3(2):155-57.doi:10.4103/0976-237X.96817 [Google Scholar]
[5]. HC Wan, YL Lai, YF Kuo, TY Liu, YT Chen, Areca nut extracts increased expression of inflammatory cytokines, tumor necrosis factor-alpha, interleukin- 1beta, interleukin-6 and interleukin-8, in peripheral blood mononuclear cellsJ Periodontal Res 2009 44:175-83. [Google Scholar]
[6]. T-N Wang, M-S Huang, M-C Lin, T-H Duh, C-H Lee, C-C Wang, Betel Chewing and Arecoline Affects Eotaxin-1, Asthma and Lung FunctionPLoS ONE 2014 9(3):e91889doi:10.1371/journal.pone.0091889 [Google Scholar]
[7]. IARC. Betel-quid and areca-nut chewingIARC Monogr Eval Carcinog Risk Chem Hum 1985 37:145-46. [Google Scholar]
[8]. B Secretan, K Straif, R Baan, Y Grosse, GF El, V Bouvard, A review of human carcinogens–Part E: tobacco, areca nut, alcohol, coal smoke, and salted fishLancet Oncology 2009 10:1033-34. [Google Scholar]
[9]. WY Lin, TY Chiu, LT Lee, CC Lin, CY Huang, KC Huang, Betel nut chewing is associated with increased risk of cardiovascular disease and all-cause mortality in Taiwanese menAm J Clin Nutr 2008 87:1204-11. [Google Scholar]