Rare Case of Spindle Cell Haemangioma
Sunanda Chavva1, M. Hima Priya2, Komali Garlapati3, G. Siva Prasad Reddy4, Ashalata Gannepalli5
1 Professor, Department of Oral Medicine and Radiology, Panineeya Institute of Dental Sciences, Road No. 5, Kamala Nagar, Dilsukhnagar, Hyderabad, Andhra Pradesh, India.
2 Post Graduate Student, Department of Oral Medicine and Radiology, Panineeya Institute of Dental Sciences, Road No. 5, Kamala Nagar, Dilsukhnagar, Hyderabad, Andhra Pradesh, India.
3 Professor, Department of Oral Medicine and Radiology, Panineeya Institute of Dental Sciences, Road No. 5, Kamala Nagar, Dilsukhnagar, Hyderabad, Andhra Pradesh, India.
4 Professor, Department of Oral & Maxillofacial Surgery, Panineeya Institute of Dental Sciences, Road No. 5, Kamala Nagar, Dilsukhnagar, Hyderabad, Andhra Pradesh, India.
5 Professor, Department of Oral & Maxillofacial Pathology, Panineeya Institute of Dental Sciences, Road No. 5, Kamala Nagar, Dilsukhnagar, Hyderabad, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. M Hima Priya, Post Graduate Student, Department of Oral & Maxillofacial Radiology, Panineeya Institute of Dental Sciences, Road No. 5, Kamala Nagar, Dilsukhnagar, Hyderabad, Andhra Pradesh-500060, India. E-mail : mhimapriya@gmail.com
Spindle cell haemangioma (SCH) is a benign vascular lesion which usually occurs on distal extremities. It was previously regarded as haemangioendothelioma and was initially perceived to be low grade angiosarcoma.They are characterized by cavernous blood vessels and spindle cell proliferation. It is now considered as a reactive lesion and conservative surgical excision is preferred treatment. Intraoral occurrence is rare; hence we present a case of SCH in a 33-year-old male that presented as a swelling below the tongue. Histopathology showed well circumscribed proliferating spindle cells attached to vessel walls, dilated vascular spaces. The lesion was positive for CD31 and CD34 markers suggesting it to be of endothelial cell origin.
Cavernous spaces (CS), Diffuse weighted image (DWI), Endothelial cells (EC), Spindle cell haemangioma (SCH), Vascular lesion (VL)
Case Report
A 33-year-old male patient reported with a chief complaint of swelling below tongue since 8 months. The swelling started as a small nodule and gradually increased to present size. There was history of pain since 2 months, which aggravated on lifting tongue and on swallowing.The medical history was noncontributory and there was no history of trauma, tooth pain or preceding inflammation and no constitutional symptoms like fever, weight loss.
Extraoral examination was unremarkable and on intraoral examination, a solitary well circumscribed swelling was present on anterior floor of mouth and lingual to lower anteriors. The size of swelling was 1 x 1.5 cm [Table/Fig-1]. The surface was smooth with no visible pulsations and no secondary changes. It was firm in consistency, tender, non-fluctuant, non-compressible, non-reducible and mobile. The oral hygiene status was good with no evidence of stains, calculus, carious lesions and apparently normal gingivo-periodontal status. The mandibular anterior teeth on percussion and palpation were normal and were vital. A provisional diagnosis of minor salivary gland tumour was made, with differential diagnosis of mucous retention cyst, ranula, lymphangioma, haemangioma, lipoma, and ectopic lymphnode.
Intraoral swelling in floor of mouth

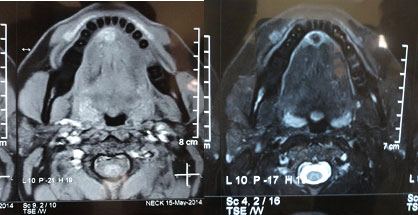
Diascopy test was not done because of anatomy and FNAC did not yield any aspirate. Intraoral periapical radiograph with respect to mandibular anterior teeth and mandibular topographical occlusal view showed no abnormality [Table/Fig-2]. MRI revealed patchy area of signal abnormality in floor of mouth, infero-medial to attachment of geniohyoid muscle. Mildly hypointense on T1 and T2 image was appreciated with an impression of malignancy from minor salivary gland [Table/Fig-3]. Mild diffuse restriction was noted on Diffuse weighted image (DWI). Complete surgical profile was advised in which no abnormality was detected. Correlating clinical, radiographic and MRI findings, odontogenic lesion was ruled out and working diagnosis of minor salivary gland tumour was arrived. Excisional biopsy of the lesion was performed under local anaesthesia [Table/Fig-4] and the specimen was subjected to histopathological examination.
Mandibular occlusal view was noncontributory

T1 & T2 weighted images showing- iso to hyperintense area in anterior floor of the mouth
Intra operative view showing reflected mucosal flap and biopsy specimen

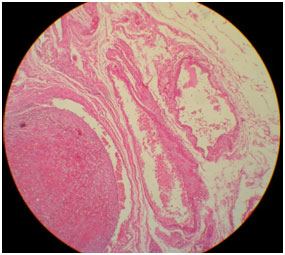
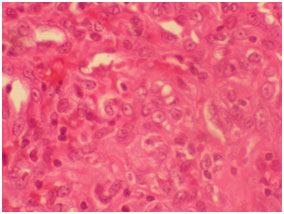
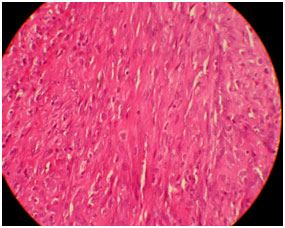
On microscopic examination, there were cavernous vascular spaces, solid spindle cells attached to vessel walls and vacuolated epitheloidendothelial cells [Table/Fig-5,6]. The lesion was well circumscribed, highly cellular with vascular proliferation and slit like spaces [Table/Fig-5,7]. There were few lymphocytes and eosinophils. Larger thin walled vessels with RBCs and areas of hemorrhage were also appreciated. The lesion did not show any cellular atypia and was well circumscribed without infiltration to surrounding structures. Histopathological diagnosis of vascular lesion i.e., spindle cell haemangioma was given. Immunohistochemistry (IHC) was done for the markers CD- 34 and CD- 31 for evaluation of origin of these spindle cells which were triple positive. Pericytes with surrounding blood vessels, split like vascular spaces lined by endothelial cells were positive for CD-34 and cells in vascular channels near endothelial lining were positive for CD 31 [Table/Fig-8] [1].
H&E 4X Histopathology slide showing dilated vascular spaces adjacent to solid spindle cell areas
H&E 40X Histopathology showing epitheloid enodethelial cells with vacuolations
H&E (10X) Histopathology slide showing spindle to epitheloid endothelial cells with slit like spaces within proliferations
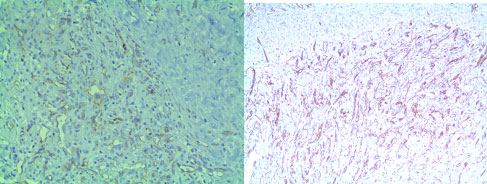
IHC (10X) CD-31,CD-34 Immunohistochemical markers showing positivity inspindle cells and cells lining vascular channels
The patient was followed up for 6 months and there was no recurrence [Table/Fig-9].
Follow up picture after 6 months

Discussion
Spindle cell haemangioma (SCH) was originally described as spindle cell haemangioendothelioma in 1986 by Weiss and Enzinger and whose behaviour fell between benign haemangioma and malignant angiosarcoma [2]. WHO in 1996 renamed it as spindle cell haemangioma when further data suggested a benign clinical course [3] They occur as solitary nodule or give rise to multiple lesions and 50% of patients have multiple lesions, usually in the same anatomic region [4,5]. Approximately one-half of cases are intravascular and such intravascular growth appears to be the mechanism for multiple lesions in the same general area [5].
Approximately 10% of cases are associated with other developmental anomalies or syndromes, including early onset varicose veins, lymphedema, Klippel-Trenaunay-Weber syndrome, Maffucci’s syndrome, epithelioid haemangioendothelioma, and superficial cutaneous lymphatic malformations [6,7]. The tumours are most common on the distal extremities, but may occur in a variety of anatomic sites, including the chest wall, genital area, head and neck, and oral cavity [1,4]. It has been rarely reported in oral cavity [1,8].
Rarely, they may arise in deep soft tissue or exceptionally at visceral sites. The tumours are multinodular within the dermis or subcutaneous tissue. The three classic histologic features, found in variable proportions in any given case, are widely dilated vascular spaces, solid spindle cell areas, and plump, rounded, or polygonal endothelial cells, with clear, often vacuolated cytoplasm [4]. The cavernous vascular spaces often contain thrombi, phleboliths, or endothelial-lined fibrous papillae (in contrast to the hyaline papillae of intravascular papillary endothelial hyperplasia, which may also be found associated with organizing thrombi) [2,4]. The solid areas are composed of spindle cells in a haphazard or short fascicular pattern surrounding partially collapsed or poorly formed, slit-like vascular channels. Small numbers of plump endothelial cells with intracytoplasmic vacuoles are found in the solid areas, either in clusters or lining the compressed vascular channels; when numerous, the vacuolated endothelial cells may mimic lipoblasts [4,7].
Depending on whether angiomatous areas or solid areas predo-minate the low-power appearance of SCH may resemble a cavernous haemangioma or, conversely, nodular Kaposi sarcoma. Advances in immunohistochemistry help in identifying the origin of spindle cells which are reactive for CD 31 and CD 34 and strong nuclear immunoreactivity of HHV 8 is noted in Kaposi sarcoma [4].
Decorin is a small extracellular chondroitin/dermatan sulfate proteoglycan which is involved in the angiogenesis-like behaviour of endothelial cells (ECs) has played diagnostic importance with Kaposi sarcoma and angiosarcoma where in both the malignant vascular neoplasms completely lack the immunoreactivity for decorin and benign vascular tumours namely haemangiomas express decorin in readily detectable amounts [9,10].
Conclusion
Although SCH are rarely present in oral cavity or probably under reported, it has to be considered under differential diagnosis of vascular tumours and should be differentiated from malignant lesions to avoid unnecessary aggressive therapy. Conservative therapy is to be of choice in SCH. Radiation therapy is contraindicated due to danger of malignant transformation.
[1]. Sheehan M, Sheila O, Roumpf. Spindle cell haemangioma: Report of a case presenting in the oral cavityJ Cutan Pathol 2007 34(10):797-800. [Google Scholar]
[2]. Weiss SW, Enzinger FM, Spindle cell haemangioendothelioma: A low-grade angiosarcoma resembling a cavernous haemangioma and Kaposi's sarcomaAm J Surg Pathol 1986 10:521-30. [Google Scholar]
[3]. Philip P, Sharon W, Spindle Cell Haemangioendothelioma: An Analysis of 78 Cases with Reassessment of Its Pathogenesis and Biologic BehaviourAm J SurgPathol 1996 20:1196-204. [Google Scholar]
[4]. Hornick JL, Practical soft tissue pathology: A diagnostic approach:323-35. [Google Scholar]
[5]. Enzinger and Weiss's Soft Tissue Tumours6:667-68. [Google Scholar]
[6]. Shafer Hine Levy Shafers textbook of oral pathology 7 :687-88. [Google Scholar]
[7]. Requena L, Kutzner H, Haemangioendotheliomaseminars in Diagnostic Pathology 2013 30(1):29-44. [Google Scholar]
[8]. Tosios K, Koutlas IG, Kapranos N, Spindle-cell haemangioendothelioma of the oral cavity.A case reportJ Oral Pathol Med 1995 24:379-82. [Google Scholar]
[9]. Järveläinen H, Juvonen V, Pelliniemi TT, Decorin Is Produced by Capillary Endothelial Cells in Inflammation-Associated AngiogenesisAmerican Journal of Pathology 2001 158(2):345-53. [Google Scholar]
[10]. Salomaki HH, Sainio AO, Soderström M, Pakkanen S, Laine J, Jarvelainen HT, Differential Expression of Decorin by Human Malignant and Benign Vascular TumoursJournal of Histochemistry and Cytochemistry 2008 56(7):639-46. [Google Scholar]