Nasal Foreign Body, Dislodged and Lost – Can the Adenoids Help?
Arijit Jotdar1, Mainak Dutta2, Subrataataata Mukhopadhyay3
1Junior Resident, Department of Otorhinolaryngology and Head-Neck Surgery, Medical College and Hospital, Kolkata, India.
2RMO-Cum-Clinical Tutor, Department of Otorhinolaryngology and Head-Neck Surgery, Medical College and Hospital, Kolkata, India.
3Professor, Department of Otorhinolaryngology and Head-Neck Surgery, Medical College and Hospital, Kolkata, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mainak Dutta, Tutor, Department of Otorhinolaryngology and Head-Neck Surgery, Medical College and Hospital, Kolkata 88, College Street, Kolkata - 700073, West Bengal, India.
E-mail: duttamainak@yahoo.com
Foreign body in the nasal cavity is one of the most common paediatric otolaryngology emergencies and needs to be promptly addressed. The incidence of nasal foreign body getting dislodged secondary to unsuccessful attempts to take it out is quite high and can be potentially dangerous as it might cause fatal airway compromise. The chances of it getting impacted and retained in the nasopharynx are practical, although such cases are seldom encountered for primarily nasal foreign bodies. Nevertheless, the nasopharynx should always be looked for as a site of impaction of hidden foreign objects. Presence of enlarged adenoids could be of help as it may prevent accidental lodgement of displaced foreign body in the airway, but might also result in difficulty in locating and retrieving the foreign body because it acts as an anchor-pad with its grooves and crevasses. This report presents a rare, interesting case of a child with enlarged adenoids anchoring a metallic ring and describes the clinical presentations and relevant management of a nasal foreign body dislodged and lost in the nasopharynx.
Inhaled, Metallic ring, Nasopharynx, Otolaryngology
Case Report
A 3-year-old boy was brought to the otolaryngology emergency of Medical College and Hospital, Kolkata, by his parents with history of insertion of a metallic nose-ring in his left nasal cavity the previous day. Following the incident he had one episode of epistaxis which stopped spontaneously.The child was taken to the local doctor where few unsuccessful attempts were made to remove the foreign body, and subsequently he was referred to the tertiary level hospital. At presentation, the child was anxious but was not dyspnoeic, and was able to take food and drinks without difficulty. There was no history of any sudden bout of cough or sudden-onset dyspnoea. It was known from his mother that he had history of insertion of foreign bodies in his nose twice before which were removed by the local physicians.
In the present instance however, anterior rhinoscopy could not reveal the ring; there was only scanty discharge with few blood-clots. Oral cavity and oropharynx were unremarkable. There was no evidence of any active orificial bleed. Vesicular breath sounds were audible without any added sound. A retained foreign body of the left nasal cavity dislodged from its initial site of impaction was suspected. To confirm, skiagram of the soft-tissue of nose and nasopharynx was done which revealed a radio-opaque shadow of a ring-like object embedded within the adenoid mass at the level of the oropharyngeal isthmus [Table/Fig-1]. We suspected it to be the missing metallic ring.
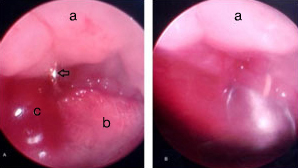
Endoscopic removal of the foreign body was planned, and the child was admitted and put on intravenous antibiotics. Following orotracheal intubation, the ring was searched for with a 2.7 mm 0 degree naso-endoscope. However, the choana was almost occluded with enlarged adenoid tissue, and no foreign body could be located; blind search with a ball-probe only resulted in brisk bleeding. A soft rubber catheter was then inserted cautiously in the right nasal cavity under endoscopic guidance and its leading end was taken out through the oral cavity. Gentle pulling of the catheter retracted the soft palate anteriorly, which also opened up the oropharyngeal isthmus. Further endoscopic examination through the left nasal cavity revealed the metallic ring with its open ends embedded within the adenoid mass at the level of the oropharyngeal isthmus [Table/Fig-2a]. It was taken out through the oral cavity with the help of a pair of upturned Blakesley forceps [Table/Fig-2b].
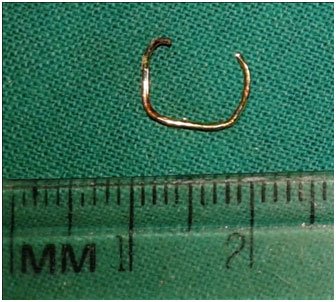
The offending foreign body was a thin steel ring about 1 cm in diameter [Table/Fig-3]. Postoperatively, the child recuperated well without any complications.
Discussion
Self-inserted foreign bodies in the upper aero-digestive tract are common in children because they are habitually inquisitive for their natural body orifices [1,2]. As we have seen in our child, past history of similar episodes can often be elicited from the parents [3]. However, retained foreign body of the nasopharynx is not encountered too often [4-6]; it is a hidden site that is least suspected to harbour a lost foreign body, accounting for the late presentation in most cases. A variety of objects has been reported to be lodged in the nasopharynx, like safety-pins [7], gold rings [4], hooked iron rod [5], metallic bolt [6], metal nut [8] and coin [9]. However, in almost all instances either proper history could not be elicited regarding the time of insertion of foreign body and the nature of it, or it got lost in the nasopharynx following attempts to remove it through the mouth. In most cases, such foreign bodies were primarily lodged in the oral cavity. In fact, it is quite unusual for an object inserted in the nose to get displaced into the nasopharynx [6]. A thorough search in the PubMed/MEDLINE® database using the given keywords revealed only few such cases in the English-language literature [6,7].
The metallic ring in the present instance got dislodged from the nasal cavity and remained anchored in the bulky adenoid tissue. This can be explained by the inadvertent posterior migration of the ring during the improper, amateurish manipulations to remove it. In most instances however, primary nasal foreign bodies dislodged posteriorly are swallowed. The chance of it remaining anchored in the nasopharyngeal soft-tissue seems theoretically obscure. Our child incidentally had large adenoids that encroached the choana and almost occluded the oropharyngeal isthmus, resulting in lodgement of the ring within the soft-tissue mass in such a way that it could not be delineated on naso-endoscopy and blunt probing.
It would be interesting to observe whether adenoids could complicate the trajectory of a nasal foreign body when it dislodges into the nasopharynx. The peak age of adenoid hypertrophy (about six-toeight years) coincides with that of foreign body insertion by children in the natural orifices of head and neck, so the question would not be irrelevant. For obvious reasons, enlarged adenoids would pose difficulty to remove a nasopharyngeal foreign body as it might hinder the surgeon’s view, whereas its exaggerated vertical furrows can act as hidden pockets for lodgement. Blind attempts to locate such foreign bodies might injure the nasopharyngeal soft-tissue causing troublesome bleed, further complicating the search. However on the other hand, had not there been the adenoids, inhaled objects inadvertently displaced into the nasopharynx could enter the luminal structures below, like oesophagus and the tracheo-bronchial tree. Accidental entry of such foreign bodies in the airway might lead to dreadful complications, including death [8]. This is of concern especially in neonates and infants, albeit theoretically, who have poorly developed cough reflex and exaggerated apnoeic response [10]. It is true that not always foreign objects displaced into the nasopharynx enter the respiratory tract in a conscious child, neither that it always gets anchored to the soft-tissue even if there are enlarged adenoids. Yet presence of adenoids, especially when large enough, can be looked upon as a sentinel which can complicate retrieval of an inhaled foreign body as well as can be life-saving by preventing it from going down into the laryngo-tracheal complex.
The key step is therefore to prevent inadvertent posterior displacement of foreign bodies lodged primarily in the nasal cavity. This is of importance especially for vegetative and radiolucent objects which, if displaced, would be impossible to locate by skiagrams. Foreign body lodged in the nasal cavity should be considered as an emergency that mandates prompt removal. Moreover, the nasopharynx should be suspected as the secret attic of upper airway often harbouring displaced oral or nasal foreign bodies. Proper history should be elicited from the parents regarding any previous attempts at removal, and specific directed search should be made by the clinicians in the nasopharynx for dislodged nasal foreign objects. Else, it may result in delayed presentation with symptoms of retained foreign body, like fetid nasal discharge and epistaxis [11]. Adenoids can further complicate the matter, as we have seen in our child. At the same time, awareness should be raised among the parents and general practitioners that blind, inefficient attempts to remove a foreign body impacted in the upper aero-digestive tract can only complicate the situation further. Such should always be done by an otolaryngologist, preferably under endoscopic or microscopic guidance.
Skiagram of soft-tissue neck (lateral view) shows a radio-opaque ring-like object anchored in the adenoid mass

Endoscopic view through the left nasal cavity (A) showing the metallic foreign body (arrow) embedded in the adenoid mass (a). NNote the pharyngeal pack (b) that could be seen through the oropharynx, and the bleeding (c) following prior manipulation with endoscopic ball-probe. The metallic ring is being taken out through per-oral route by an upturned Blakesley forceps (B)
The metallic ring, after retrieval
Conclusion
Inhaled foreign bodies can rarely get impacted in the nasopharynx and is generally iatrogenic. Enlarged adenoids can be the seat for anchorage of sharp objects which may often be difficult to locate. However, it also protects the child from accidental aspiration. A nasal foreign body dislodged due to naïve manipulations can therefore be potentially dangerous, and timely referral should be made by the primary care physicians for expert intervention. Above all, a high index of suspicion should be maintained and the nasopharynx and adenoids should always be inspected and examined as potential sites of displaced and hidden nasal foreign bodies.
[1]. M Dutta, S Ghatak, G Biswas, Chronic discharging ear in a child: are we missing something?Med J Malaysia 2013 68(4):368-71. [Google Scholar]
[2]. L Ray, P Chatterjee, SN Bandyopadhyay, S Das, R Sinha, TK Nandy, An unusual foreign body (Big Metallic Nut) in the nasopharynx of an infantIndian J Otolaryngol Head Neck Surg 2004 56(4):309-10. [Google Scholar]
[3]. A Mukherjee, D Haldar, S Dutta, M Dutta, J Saha, R Sinha, Ear, nose and throat foreign bodies in children: A search for socio-demographic correlatesInter J PediatrOtorhinolaryngol 2011 75(4):510-12. [Google Scholar]
[4]. F Ogut, M Bereketoglu, C Bilgen, S Totan, A metal ring that had been lodged in a child's nasopharynx for 4 yearsEar Nose Throat J 2001 80(8):520-22. [Google Scholar]
[5]. ES Diom, R Diouf, HM Diopel, Unusual nasopharyngeal foreign body: a hooked iron rodEar Nose Throat J 2012 91(7):E13-14. [Google Scholar]
[6]. S Kumar, DB Singh, AB Singh, An unusual nasopharyngeal foreign body with unusual presentation as nasal regurgitation and change in voiceBMJ Case Rep 2013 July 24.doi: 10.1136/bcr-2013-010005 [Google Scholar]
[7]. KS Dasgupta, KY Lanjewar, SV Joshi, Safety pin-The unsafe foreign body of air passageIndian J Otolaryngol Head Neck Surg. 2006 58(4):387-88. [Google Scholar]
[8]. JKAG Sunkum, Nasopharyngeal foreign body in an young childIndian J Otolaryngol Head Neck Surg 2011 63(3):285-86. [Google Scholar]
[9]. ZM Raahat, Coin in the nasopharynx in a young childJ Coll Physicians Surg Pak 2003 13(4):235-36. [Google Scholar]
[10]. BT Thach, Maturation of cough and other reflexes that protect the fetal and neonatal airwayPulmPharmacolTher 2007 20(4):365-70. [Google Scholar]
[11]. HA Cohen, E Goldberg, Z Horev, Removal of nasal foreign bodies in childrenClin Pediatr (Phila) 1993 32(3):192 [Google Scholar]