Non Functional Unilateral Adrenal Myelolipoma, A Case Report
Anita B Sajjanar1, Vidisha S. Athanikar2, U S Dinesh3, Bhuvnesh Nanjappa4, Preetam B. Patil4
1Assistant Professor, Department of Pathology, SDM College of Medical Sciences & Hospital, Dharwad, Karnataka, India.
2Professor, Department of Pathology, SDM College of Medical Sciences & Hospital, Dharwad, Karnataka, India.
3Professor, Department of Pathology, SDM College of Medical Sciences & Hospital, Dharwad, Karnataka, India.
4Associate Professor, Department of Urology, SDM College of Medical Sciences & Hospital, Dharwad, Karnataka, India.
5Associate Professor, Department of Radiology, SDM College of Medical Sciences & Hospital, Dharwad, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anita B Sajjanar, 211, Shreyas Block, SDM Staff quarters, Sattur, Dharwad-580009, Karnataka, India.
E-mail: anitavijay28@gmail.com
Adrenal myelolipoma is characterized by presence within the adrenal gland of mature adipose tissue and active bone marrow elements. Owing to their non functional nature most cases are incidental, either at autopsy or through computer tomography scan. Occasionally the lesions attain a large size to become clinically apparent. We present a case of a 58-year-old female with mass per abdomen. Preoperative computer tomography scan of abdomen, hormonal and urine analysis showed features of non functional adrenal myelolipoma. Gross specimen consists of unilateral ovoid mass, external surface having capsule with adherent fat and areas of congestion. Microscopic examination showed well encapsulated tumour tissue composed of mature adipose tissue with major blood forming elements like myeloid, erythroid and megakaryocytic series. The diagnosis was confirmed by histopathological examination of right sided adrenalectomy specimen.
Adrenal gland, Adrenalectomy, CT scan
Case Report
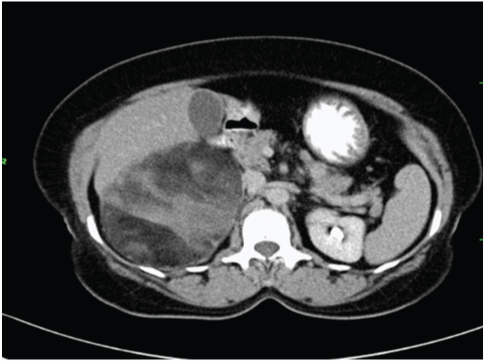
A 58-year-old female patient presented at the Department of Urology, SDM College of Medical Sciences & Hospital with the complaints of mass per abdomen and dragging type of pain in right lower abdomen since past one year. The gradually progressing mass was accompanied by insidious onset pain since past six months. Ultrasonography of the abdomen showed evidence of well-defined homogenously hyperechoic mass lesion in the suprarenal portion. A multi dimensional computed tomography (CT) scan revealed a large, well defined, oval shaped, solid mass in the right supra-renal region [Table/Fig-1]. It was containing both soft tissue and fat component. The dimensions of the mass on CT scan were as follows, 15cm (cranio-caudal) x 9cm (antero-posterior) x 12cm (medio-lateral).
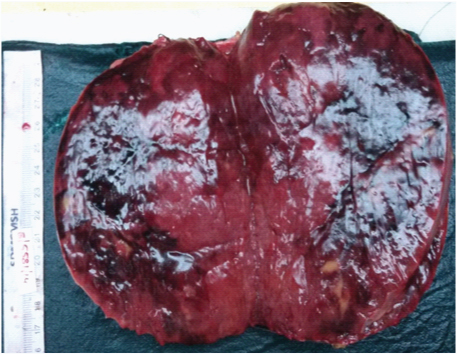
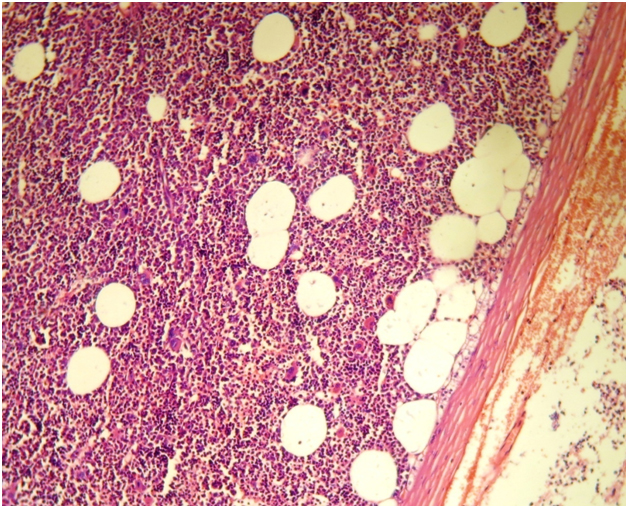
The hormonal and urinary analyses of the patient were unremarkable and are shown in the [Table/Fig-2,3] respectively. Patient underwent a planned laparotomy for right adrenalectomy. The specimen was received for histopathological examination. The gross specimen [Table/Fig-4] consists of ovoid mass weighing 586 grams, measuring 14 x 11 x 5.5cm. External surface showed capsule with adherent fat and areas of congestion. Cut section [Table/Fig-5] showed grey brown, yellowish areas with areas of haemorrhage. Microscopic examination [Table/Fig-6a&6b] revealed well encapsulated tumour tissue composed of mature adipose tissue with major blood forming elements like myeloid, erythroid and megakaryocytic series which further confirmed it as adrenal myelolipoma.
Discussion
Myelolipoma is a rare benign tumour found in adrenal gland. The tumour was initially described by Giercke in 1905 and later the term” myelolipoma” was coined by Oberling in 1929 [1]. The incidence of adrenal myelolipoma is 0 .08 to 0.4% at autopsy [2]. The non functional nature of these masses renders them clinically obscure unless they grow in size significantly. It is characterized by presence within the adrenal gland of mature adipose tissue and active bone marrow elements [3]. The bone marrow component usually shows normal trilineage haematopoiesis, but, with markedly increased number of megakaryocytes [4].
Most of the cases are found either at autopsy or while CT scan of the abdomen as Incidentaloma [5]. The tumour usually does not show any sex predilection [6]. Very rarely they affect both the adrenal glands [7]. Present day practice of inclusion for non invasive investigation like ultra-sonography or CT scan as a routine test for pain in abdomen has led to increased chances of detection of adrenal myelolipoma.
Several theories regarding the aetiology of adrenal myelolipoma have been studied. The most widely accepted amongst all of them is that due to metaplastic change in the reticuloendothelial cells of blood capillaries in response to stimuli including necrosis, infection or stress [8]. Prolonged stimulation with high level of adrenocoticotropic hormone or adrenal androgen also has been sought as cause of this benign lesion.
Bennett BD et al., reported occurrence of myelolipoma with Cushing syndrome, congenital adrenal hyperplasia, and adrenal ganglioneuroma [9]. In our case the tumour was non functional as preoperative hormonal and urinary analysis were normal. Diagnostic techniques such as ultra-sonography, computed tomography, and magnetic resonance imaging are effective in detecting more than 90% of adrenal myelolipoma. Computed tomography on the basis of identification of fat is the most sensitive amongst all the radiological investigative modalities. Presence of fat on CT clinched the diagnosis of myelolipoma in the present case.
The presacral region being the commonest site of extra adrenal site of myelolipoma [10]. Hunter SB et al.,, reported two cases of extra adrenal myelolipoma, of the two one was multifocal involving lungs and retroperitoneal site. Both these patients were treated by steroid as against surgery possibly considering uncertain aetiology [11].
The differential diagnosis in such a lesion includes renal angiomyolipoma, retroperitoneal lipoma, and liposarcoma. However, microscopic features like mature adipose tissue with major blood forming elements like myeloid, erythroid and megakaryocytic series are confirmatory of adrenal myelolipoma on histopathological grounds. Occasionally the lesions attain such a large size to become clinically apparent at its presentation itself [12]. Although, great number of incidentally discovered lesions is small and asymptomatic, reports are infrequent for cases of large symptomatic lesions. The well-recognized complication of large adrenal myelolipoma (>10 cm) may present with spontaneous retroperitoneal haemorrhage or abscess [13]. Therefore, a symptomatic tumour seems to be treated surgically.
With improved surgical techniques and perioperative care excision of these masses has become possible without any increase in surgically derived morbidity or hospital stay [14]. Gagner et al., introduced laparoscopic adrenalectomy for the treatment of both functioning and non-functioning adrenal tumours [15]. Usually lesions which are asymptomatic and measure <5cm are monitored over a period of 1 to 2 years with imaging [8].
Axial section of computed tomogram showing mass in right supra renal gland
| Hormonal Assay | Patient value | Reference range |
|---|
| Adrenocoticotropic hormone (ACTH) | 21.90 pg/ml | 10-46 pg/ml |
| Estradiol | 11.8o pg/ml | 0-30 pg/ml |
| Dehydroepiandrosterone | 2.34 ng/ml | 1-12 ng/ml |
| Adrenaline | 5.46 μg /day | 4-20 μg /day |
| Nor- Adrenaline | 63.60 μg /day | 20-105 μg /day |
| Patient value | Reference range |
|---|
| Urine cortisol 24 hours urine volume (2000 ml) | 179.6 μg/day | 58-403 μg /day |
| 24 hours urine VMA | 5.6 mg/24hrs | 1.6-7.3 mg/24hrs |
Gross appearance of adrenal myelolipoma

Cut section showing grey brown, yellowish areas with areas of haemorrhage
Microscopy showing matured adipose tissue, bone marrow elements, adjoining adrenal tissue and capsule. (H&E - 100X)
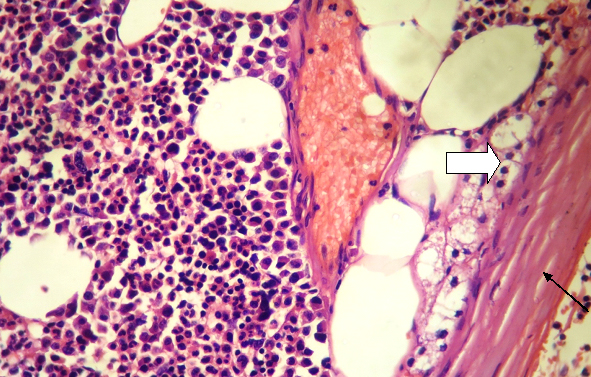
Microscopy showing matured adipose tissue, bone marrow elements and adjoining adrenal tissue (Thick arrow), Capsule (Thin arrow). (H&E - 400X)
Conclusion
Our case report highlights the rare occurrence of non functional, unilateral adrenal myelolipoma. The non secretory nature keeps them undiagnosed till they increase in size significantly. In correlation with radiological findings presence of mature adipose tissue with major blood forming elements like myeloid, erythroid and megakaryocytic series are clue to the histopathological diagnosis.
[1]. PJ Kenney, BJ Wagner, P Rao, CS Heffess, Myelolipoma: CT and pathologic featuresRadiology 1998 208(1):87-95. [Google Scholar]
[2]. CA Olsson, RJ Kran, RC Klugo, SM Selikowitz, Adrenal myelolipomaSurgery 1973 73(5):665-70. [Google Scholar]
[3]. DP O’Malley, Benign extramedullary myeloid proliferationMod Pathol 2007 20(4):405-15. [Google Scholar]
[4]. E Bishop, JN Eble, L Cheng, M Wang, DR Chase, A Orazi, Adrenal myelolipoma show non random X-chromosome inactivation in haematopoietic elements and fat: support for a clonal origin of myelolipomasAm J SurgPathol 2006 30(7):838-43. [Google Scholar]
[5]. Y Aso, Y Homma, A survey on incidental adrenal tumours in JapanJ Urol 1992 247(6):1478-81. [Google Scholar]
[6]. M Han, AL Burnett, EK Fishman, FF Marshall, The natural history and treatment of adrenal myelolipomaJ Urol 1997 157(4):1213-16. [Google Scholar]
[7]. JL Kraimps, R Marechaud, P Levillain, JF Lacour, J Barbier, Bilateral symptomatic adrenal myelolipomaSurgery 1992 111(1):114-17. [Google Scholar]
[8]. SI Tyritzis, I Adamakis, V Migdalis, D Vlachodimitropoulos, CA Constantinides, Giant adrenal myelolipoma,a rare urological issue with increasing incidence: case reportCases J 2009 2:8863 doi: 10.4076/1757-1626-2-8863 [Google Scholar]
[9]. BD Bennett, TJ McKenna, AJ Hough, R Dean, DL Page, AdrenalMyelolipoma associated with Cushing’s diseaseAm J Clin Pathol 1980 73(3):443-47. [Google Scholar]
[10]. V Varone, G Ciancia, U Bracale, G Merola, A Vetrani, G Pettinato, Multidisciplinary diagnostic approach combining fine needle aspiration, core needle biopsy and imaging features of a presacral myelolipoma in a patient with concurrent breast cancerPathol Res Pract 2015 211(3):261-63.doi: 10.1016/j.prp.2014.12.004. Epub 2014 Dec 23 [Google Scholar]
[11]. SB Hunter, EH Schaemankewitz, C Patterson, VA Varma, Extra adrenal myelolipoma. A report of two casesAm J ClinPathol 1992 97(3):402-04. [Google Scholar]
[12]. JL Wilhelmus, GR Schrodt, MT Alberhasky, MO Alcorn, Giant adrenal myelolipoma: case report and review of the literature Arch Pathol Lab Med 1981 105(10):532-35. [Google Scholar]
[13]. S Kumar, K Jayant, S Prasad, S Agrawal, KM Parma, R Roat, Rare adrenal gland emergencies: a case series of giant myelolipoma presenting with massive hemorrhage and abscessNephrourol Mon 2015 7(1):e22671-79.doi: 10.5812/numonthly.22671.e Collection 2015 [Google Scholar]
[14]. YW Novitsky, DR Czerniach, KW Kercher, RA Perugini, JJ Kelly, DE Litwin, Feasibility of laparoscopic adrenalectomy for large adrenal massesSurg Laparosc Endosc Percutan Tech 2003 13(2):106-10. [Google Scholar]
[15]. M Gagner, A Lacroix, E Bolté, Laparoscopic adrenalectomy in Cushing's syndrome and pheochromocytomaN Engl J Med 1992 327(14):1033 [Google Scholar]