Treadmill test is often employed in clinical practice to unmask symptoms and signs of cardiac ischemia exposing the heart to stress of exercise [1]. However, its value as a screening test in healthy populations is not established. Nevertheless, exercise testing in treadmill is an accepted practice to evaluate physical work capacity and endurance [2,3]. Endurance may be considered as the ability of the body to withstand the stress induced by prolonged activity. Limits of endurance are evaluated based on symptom-limited point of exhaustion by several subjective criteria or by objective means whichever is earlier for reasons of safety. These include reported subjective experience of exhaustion and/or by objective estimates of rise in heart rate, blood pressure, ECG changes, stage and duration of exercise reached and corresponding equivalent distance covered, Maximal Peak exercise O2 consumption (VO2Max). According to McKiman et al., [4], magnitude of O2 uptake correlates well with intensity of exercise and is a measure of functional aerobic capacity. Endurance testing on treadmill exercise is done by permitting graded increments in treadmill speed and grade at intervals of time. Among several protocols developed for exercise testing on treadmill, Bruce multistage exercise protocol is widely accepted format [5,6].
While the physiological causes of fatigue and stress are well documented, the role of motivation and psychological perception of stress in limiting exercise is not widely explored. Lack of motivation and perceived sense of tiredness due to dull repetitive nature of exercise protocol is likely to conceal the actual physical ability to prolong work. Removal of these constraints according to Wilmore [7] yielded greater work output. Borg pointed out that perceived exertion is the single best indicator of physical endurance [8]. Against this backdrop, the present study is undertaken in a group of 30 healthy young male medical students, to investigate the quantitative contribution of psychological perceptual modification on Treadmill exercise test results as indicators of endurance level.
Materials and Methods
Subjects: A total of 30 healthy male volunteers between the ages of 18 to 21 years were recruited from 1st year medical students with the objective of comparing endurance profiles on treadmill exercise, with and without modification of stress perception. They constituted a homogenous group within a height range of 165 to 175 cm and weight range of 60 to 68 kg. As these students did not have any regular athletic background, they were ideally suited for better comparison of exercise capacity. The purpose of the study and procedure of treadmill exercise test were explained and a demonstration arranged for familiarization.Written informed consent was obtained from the participants while making it clear that participation was purely voluntary, can withdraw at anytime and that confidentiality will be maintained. Detailed medical history was taken to exclude habituation to smoking, alcohol, anxiety disorders or any other illness. Physical examination of all the volunteers was carried out to exclude respiratory and cardiovascular disorders.
The study period was spread over three months when the ambient room temperature was at a comfortable zone of 25° to 27° C. The test procedure was fixed before noon-3 hours after breakfast and nothing thereafter till the exercise test was concluded. The entire test procedure was carried out under two modes; one without any subjective intervention referred to as Mode A and the other with individualized exposure to music of choice through earphones of pocket-tucked record player, known as Mode B. Before initiating the exercise protocol, resting values of systolic and diastolic blood pressure and ECG were recorded in supine position for each participant. From ECG, levels of S-T segments and heart rate (beats/minute) were recorded which form objective reference points to detect the extent of cardiac stress during the treadmill exercise and to terminate it if necessary.
The treadmill test system employed was “Nasan ST=, Version 6.0 computerized model”. The treadmill speed, elevation and other test functions was calibrated using the software programme in accordance with Bruce multistage Protocol which permits graded increments in treadmill speed and grade at regular intervals of time; usually 3 minutes. It also records cumulative total exercise time and corresponding values of METs [9,10]. The term MET is the unit often employed to express O2 uptake in multiples of resting requirement. One MET is equivalent to a resting O2 usage of 3.5ml of O2/kg body weight/min [11]. Used as an index of work intensity in lieu of direct means of estimating exercise O2 consumption and VO2 max.
The endpoint that limits the test was usually a symptom or sign. For each volunteer a time gap of one week was allowed to lapse between the first test session in Mode A and the second in Mode B to avoid the benefit of practice induced facilitation in the immediate aftermath.
Test Parameters: During the exercise modes for each volunteer test parameters such as ECG, heart rate, change in the level of S-T segment, systolic and diastolic blood pressure were monitored; and the values were recorded at the end of each stage of the protocol (3 minutes). The test was terminated either by subjective symptoms (perceived sense of exhaustion, shortness of breath, chest pain, etc.) or by objective signs of distress (excessive rise or fall in blood pressure, cyanosis, pallor, attaining t90 [11,12], appearance of ECG changes like ectopic beats, conduction defects, > 2mm depression or elevation of ST segment etc.) whichever was earlier.
Guided by the above criteria, each volunteer was permitted to continue exercise till his upper limit was reached. At the termination of the test, when peak exercise limit was reached in each mode cardiovascular parameters and Rate-Pressure (R-P) product were recorded. R-P product is taken as index of cardiac stress [13,14]. In addition, the cumulative time or total exercise time, distance covered and METs were also recorded for comparative evaluation between the two modes.
Statistical Analysis
Difference between the modes of employed exercise protocol were analyzed for each parameter through paired t-test with α = 0.05.
Results
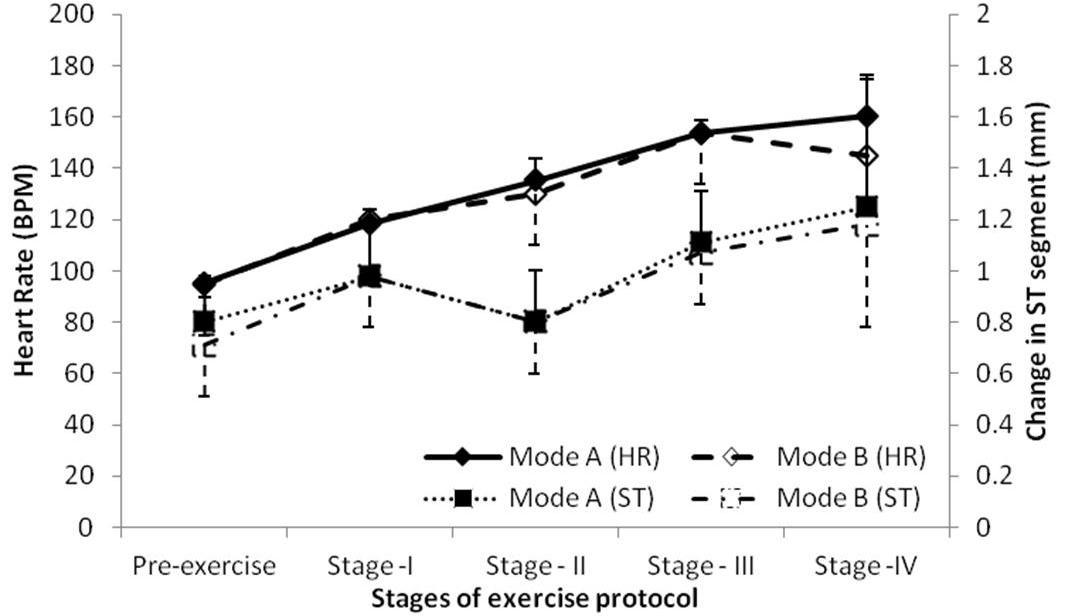
As depicted in [Table/Fig-1], there was no statistically significant difference between the modes of exercises in terms of cardiovascular parameter before and at the end of exercise. However, statistically insignificant differences between modes were only observed in case of heart rate at different stages of exercise protocol [Table/Fig-2]. In this study ECG did not reveal any S-T segment changes warranting undue cardiac stress [Table/Fig-2]. The volunteers terminated the test based only on subjective perception of stress before any objective signs appeared. For both modes of exercise protocol, all the volunteers could complete the stages I and II. Stage III exercise could be completed by 83% of participants in Mode A, while that 90% in Mode B. Similarly, noticeable higher completion ratio (26%) was observed for Stage IV exercise in Mode B as compared to that of 16% in case of Mode A.
Cardiovascular parameters for pre-exercise conditions in both Mode A and Mode B of exercise protocol
| Parameters | Pre-exercise | Peak-exercise |
|---|
| Mode-A | Mode-B | Mode-A | Mode-B |
|---|
| Heart Rate (BPM) | 95.06 ± 28 | 94.80 ± 3.04 | 170.0 ± 6.44 | 166.48 ± 21.35 |
| Blood Pressure (mmHg) | Systolic | 120.00 ± 1.71 | 116.64 ± 2.12 | 145.00 ± 1.80 | 146.00 ±10.70 |
| Diastolic | 86.32 ±2.38 | 81.12 ± 1.29 | 72.00 ± 9.35 | 73.00 ± 9.94 |
| ST Segment (mm) | 0.80 ± 0.09 | 0.71 ± 0.20 | 1.35 ± 0.12 | 1.50 ± 0.33 |
| Rate Pressure product (x103) | 14.18 ± 2.04 | 11.62 ± 1.82 | 24.27 ± 3.85 | 23.44 ± 4.33 |
Each value is expressed as Mean ± Standard Deviation of 30 observations
Changes in heart rate (HR) and level of ST segment (ST) in different stages of exercise in two modes of experimental setup. Each point represents Mean ± Standard Deviation
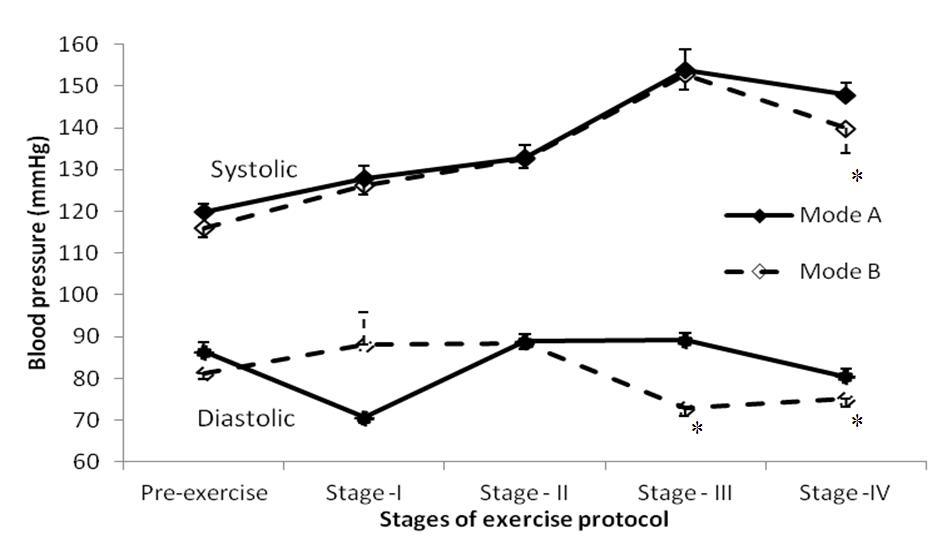
Considering the subjects who could complete the stage III, the Mode B regime had significantly lower diastolic blood pressure while the differences in systolic blood pressure between two modes were statistically insignificant [Table/Fig-3]. Interestingly, by the end of stage IV, both systolic and diastolic blood pressure was significantly low in Mode B experimental setup [Table/Fig-3]. Statistical evaluation found significantly higher values for METs, total distance covered and the total duration of exercise in Mode B regime of exercise [Table/Fig 4].
Changes in systolic and diastolic blood pressure in different stages of exercise in two modes of experimental setup. Each point represents Mean ± Standard Deviation. *Indicates significance (p<0.05) between the modes
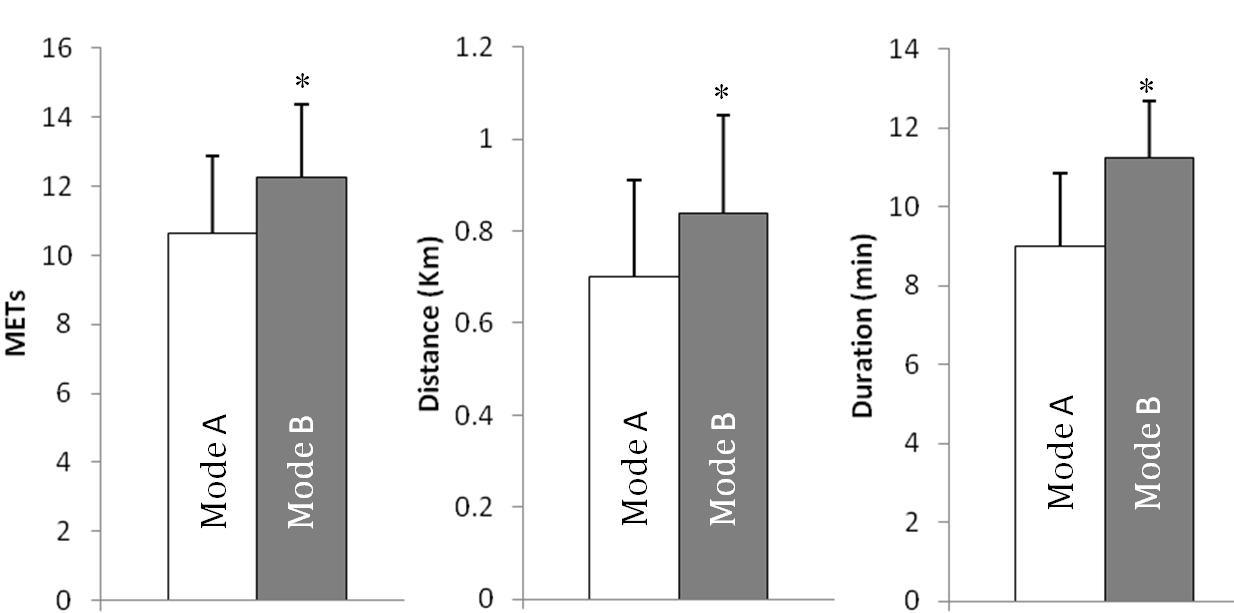
Difference between two modes of experimental setup in terms of METs, cumulative distance and cumulative duration at the end of exercise protocol. Each point represents Mean+Standard Deviation. *Indicates significance (p<0.05) between the modes
Discussion
Treadmill exercise test is an invaluable diagnostic tool often employed to uncover latent myocardial ischemic changes that may appear in ECG, when functional limits of endurance are reached. The decisive factor in test termination and hence the functional limit of endurance is the first onset of either perceived stress or objective signs referred earlier. Results of the present study focus on the role of music induced subjective Rating of Perceived Exertion (RPE) on cardiovascular functional parameters at all stages of test procedure and other measures of endurance.
A cursory glance at [Table/Fig-1] leaves an impression of some favourable decline in even basal resting HR and BP values as well as ST segment levels, in Mode B, negligible though. The rationale is based on the fact that limbic cortex and hypothalamus mediated emotional influences on medullary cardiovascular centres. Besides activation of corticohypothalamic cholinergic sympathetic vasodilator system in the skeletal muscle blood vessels may also account for somewhat lower blood pressure under music induced pleasant psychic experience [15,16].
The notable feature that the present study reveals is the effect of perceived stress modification in Mode B on the number of subjects enduring longer and graded increase in stress levels when compared to Mode A. The treadmill speed, grade and elevation were increased at 3 min intervals as per Bruce protocol. While all the 30 volunteers could pass through the first two stages of 6 min period under both modes, relatively more numbers could endure longer and greater degrees of stress under mode B.
It is obvious from [Table/Fig-2] that the heart rate increased with the progression of exercise almost to similar degree through stage I under both modes but the margin of difference was more profound in Mode B only in stage IV. With increasing degrees of exercise stress heart rate rise was of lesser magnitude with perceptual intervention. Of particular significance is the degree of heart rate rise which is said to be a major determinant of increased cardiac output and exercise capacity particularly at higher levels [17]. Increased circulating levels of catecholamines, body temperature and changes in blood chemistry, like acidemia, hypoxia and hypercapnia also increases the heart rate during exercise.
Systolic blood pressure expectedly increased with progression of exercise [Table/Fig-3] due to the associated cardiac chronotropic and inotropic effects. The contribution of inotropic response according to Fagraeus and Linnarsson is predominantly neurogenic being a result of decreased vagal outflow and later increased sympathetic activity [18]. But the progression of rise is obviously traced on the lower side in Mode B suggesting lesser vascular stress. Diastolic blood pressure except in stage I, showed a lower value in mode B particularly with increasing stress of exercise in later stages of III and IV. This may perhaps be due to greater degree of vasodilatation in exercising muscles and corresponding decline in peripheral resistance. It is likely that under states of reduced psychological stress perception there may be better muscle blood flow and hence better endurance to exercise.
A comparison of indicators of endurance profiles in mean values between the two modes is made at a point of peak exertion limit when the individual could no longer sustain the exercise based on perceived sense of exhaustion [Table/Fig-4]. There is no objective evidence of any cardiac ischemia at any stage of graded exercise stress, the ST segment levels being within normal limits in both modes ranging between 0.70 to 1.58 mm [Table/Fig-1]. Therefore the termination of exercise was solely based on the individual’s perceived sense of exhaustion before the objective ECG signs evolved. According to Borg [8], who made extensive studies on psycho physiological basis of exertion, perceived stress is the single best indicator of degree of physical strain.
The important indices of exertional stress such as (a) total exercise duration, (b) total distance covered and (c) energy cost in terms of METs showed significant improvement in Mode B [Table/Fig-4], while the Rate-Pressure product in fact declined though not significantly [Table/Fig-1] when volunteers were exposed to music of their choice.
The Rate-Pressure (R-P) product is also taken as indicator of myocardial stress. According to Fletcher and Schlant [19], the values of R-P product range between 25000 to 40000 and are said to be proportional to cardiac work involved and related myocardial O2 consumption. Lesser R-P product value in Mode B can be viewed as a favourable sign of lesser degree of cardiac stress and lesser O2 demand for a given work load. It is apparent from the table that at peak exercise limit, the rise in heart rate was comparatively less though it was not statistically significant. Likewise the rise in systolic and diastolic blood pressure and ST segment levels under both modes were not significant, implying better exercise performance with lesser cardiovascular stress. Endurance to severity of exercise notably is a function of ability of the body to supply O2 [20] which in this study is reflected by a significant increase in METs in Mode B.
The comparative improvement in the first three mentioned parameters (a) total exercise duration, (b) total distance covered and (c) energy cost in terms of METs is made visually obvious in [Table/Fig-4]. Morehouse and Miller [21] defined endurance as the ability of the body to withstand the stresses by prolonged activity. Viewed from this point the longer duration of run on the treadmill the total distance covered and METs point to improved endurance with perceived stress modification in Mode B.
Conclusion
Present study has conclusively demonstrated that subjects enjoying music (Mode B) could withstand greater degrees of exercise stress without proportionate increase in cardiac stress parameters compared with their earlier performances on same exercise protocol exposing them only to perception of stress. Therefore, favourable modulation of stress perception may motivate and improve physical performances in day-to-day life.
Each value is expressed as Mean ± Standard Deviation of 30 observations