Introduction
Overt abnormalities in thyroid function affect 9-15 % of individuals [1]. Minor abnormalities in thyroid function which includes subclinical hypothyroidism and hyperthyroidism is more common [2].
Thyroid hormone exerts numerous effects on the cardiovascular system and is therefore not surprisingly, associated with several adverse consequences on it [3]. Overt and subclinical hypothyroidism, with its accompanying hypercholesterolemia and hypertension, has been found to be associated with cardiovascular disease [4]. Variations of free T3 have been linked to coronary artery disease. Several studies have shown an association between overt and subtle thyroid function abnormalities and atherosclerosis. It remains a matter of speculation that variation of thyroid function within the normal range can lead to adverse outcome with respect to coronary artery disease (CAD) [5].
With this background, we conducted a study to observe whether there is a relationship between the variation of the serum thyroid hormone levels {Thyroid stimulating hormone (TSH), Free T3 (FT3)and free thyroxine (FT4)} within the normal range and the presence and severity of CAD. The severity of CAD was assessed using the Gensini coronary artery disease scoring system in the euthyroid patients.
Materials and Methods
A total of 100 consecutive euthyroid patients with stable angina who underwent coronary angiography at the Kasturba Medical College, Manipal between June 2012 to June 2013 were enrolled in the study. Patients with acute coronary syndrome, HIV positive, hepatic diseases, renal failure, acute infectious diseases, patients operated for thyroid disease, pregnant women and patients using Rau4antithyroid drugs/thyroxine supplements, lithium, amiodarone and glucocorticoids were excluded from the study.
Informed consent was obtained from all participants after the approval of the institutional ethics committee. Patients were interviewed about clinical characteristics and conventional risk factors for CAD such as hypertension, hypercholesterolemia, diabetes mellitus (DM), history of smoking and family history of coronary artery disease.
Laboratory Tests
Blood sampling was performed in 8 h fasting state before the coronary angiography for measuring the levels of glucose, glycosylated Hb, creatinine, total cholesterol, triglycerides, low-density lipoprotein (LDL) cholesterol and high-density lipoprotein (HDL) cholesterol. Serum TSH, FT3 and FT4 levels were measured by the chemiluminescence method using the COBAS 6000 and ELECYSIS 2010 Analysers (Roche, Mannheim, Germany). The inter-assay coefficients of variation were below 3.0%.
The reference ranges are as follows: FT3 = 2 to 4.4 pg/mL; and FT4 = 0.9 to 1.7 ng/dL.
Coronary Angiography
Coronary angiography was performed through the femoral/radial artery and the angiograms were visually evaluated by interventional cardiologists who were blinded to the study plan and to each other. A thorough analysis of each coronary angiography established the lesion location and the percentage of stenosis. Coronary artery disease was defined as >50% stenosis in the luminal diameter in at least one major epicardial coronary artery [6]. According to arteriography, the patients were divided into two groups as those with CAD and non CAD i.e. those with normal coronaries or minimal atherosclerotic lesions.
The Gensini scoring system was used to define the severity of the CAD. This method grades the narrowing in the lumen of the coronary arteries as 1 for 1-25% stenosis, 2 for 26-50%, 4 for 51-75%, 8 for 76-90%, 16 for 91-99%, and 32 for total occlusion. The score is then multiplied by a factor illustrating the importance of the lesion’s location. For the location scores, 5 points are assigned for left main lesion; 2.5 for left circumflex (LCX) artery and proximal left anterior descending (LAD); 1.5 for the mid-segment LAD and LCX; 1 for the distal segment of LAD and LCX, first diagonal branch, first obtuse marginal branch, right coronary artery, posterior descending artery, and intermediate artery; and 0.5 for the second diagonal and second obtuse marginal branches [7].
Gensini Score Calculation:severity score × segment location multiplying factor X collateral adjustment factor.
Lesions were also categorized according to number of vessels involved. Grade 0 was given smooth epicardial arteries, Grade 0.5 to plaquing <50 % diameter stenosis, Grade 1to single vessel disease, Grade 2 to double vessel disease and Grade 3 to triple vessel disease.
Statistical Analysis
Data analysis and interpretation was done with IBM SPSS Statistics v16.0. Results for normally distributed continuous variables were expressed as mean (± standard deviation {SD}) and analysed by Student T-test and ANOVA test. Skewed data was analysed using Mann Whitney U-test and Kruskal–Wallis test. Categorical variables were expressed in number and percentage and were analysed using Chi-square test. The relationships between the variables were examined with the help of Spearman’s correlation coefficients. The cut-off value of FT3 for predicting the presence and severity of CAD with corresponding sensitivity and specificity was estimated through the receiver operating characteristic (ROC) curve analysis. A binary logistic regression analysis was performed to evaluate the independent predictive values of the potential variables for the presence and severity of CAD. p<0.05 was taken as significant.
Results
The baseline characteristics of the patients are illustrated in [Table/Fig-1]. In the present study 45% did not have significant narrowing of coronary arteries, 23% had single vessel disease, 15% had double vessel disease and 17% had triple vessel coronary artery disease. The two groups were comparable with respect to age and gender. Patients with diabetes mellitus and hypertension were significantly higher in CAD group when compared to non CAD group.
Biochemical parameters of patients like Total cholesterol, LDL, Triglycerides, HDL, were also comparable between groups. There was no statistical difference in the TSH levels in the Non CAD and CAD groups (2.54+1.32 vs. 2.47+1.38micIU/ml) (p=0.07). Though the free T4 levels were lower in CAD group (1.16+0.153 ng/dl) when compared to non CAD group (1.19+0.18 ng/dl), the difference was statistically non significant (p= 0.37). Free T3 levels were significantly lower in CAD group (2.84+0.49 pg/ml) as compared to non CAD group (3.05+0.42 pg/ml) (p=0.025).
Thyroid function test was further analysed in the grades of coronary artery disease by Annova Test (freeT3 and freeT4) and Kruskalwallis test (for TSH). Free T3 level was significantly lower in severe CAD (p=0.010). The post-hoc test (by Tukey method) showed that normal coronary group had significantly higher mean values than triple vessel disease (p=0.004). There was no other significant difference between the groups with respect to TSH and free T4.
Thyroid function was correlated with Gensini score. TSH levels did not have a significant correlation with Gensini score (p=0.55). Free T3 levels showed an inverse relation with Gensini score (Pearson’s correlation =-0.30) which was statistically significant (p =0.002). Free T4 levels also showed an inverse relation with Gensini score (Pearson’s correlation =-0.08), however it was statistically not significant (p =0.39).
Predictors of CAD
In the present study presence of CAD was associated with diabetes, hypertension and male gender. However, FT3 was not significant as predictor for presence following regression analysis. FT3 remained a significant predictor of the severity of CAD (OR: 0.08, 95% CI: 0.0183-0.42, p=0.003) [Table/Fig-2,3].
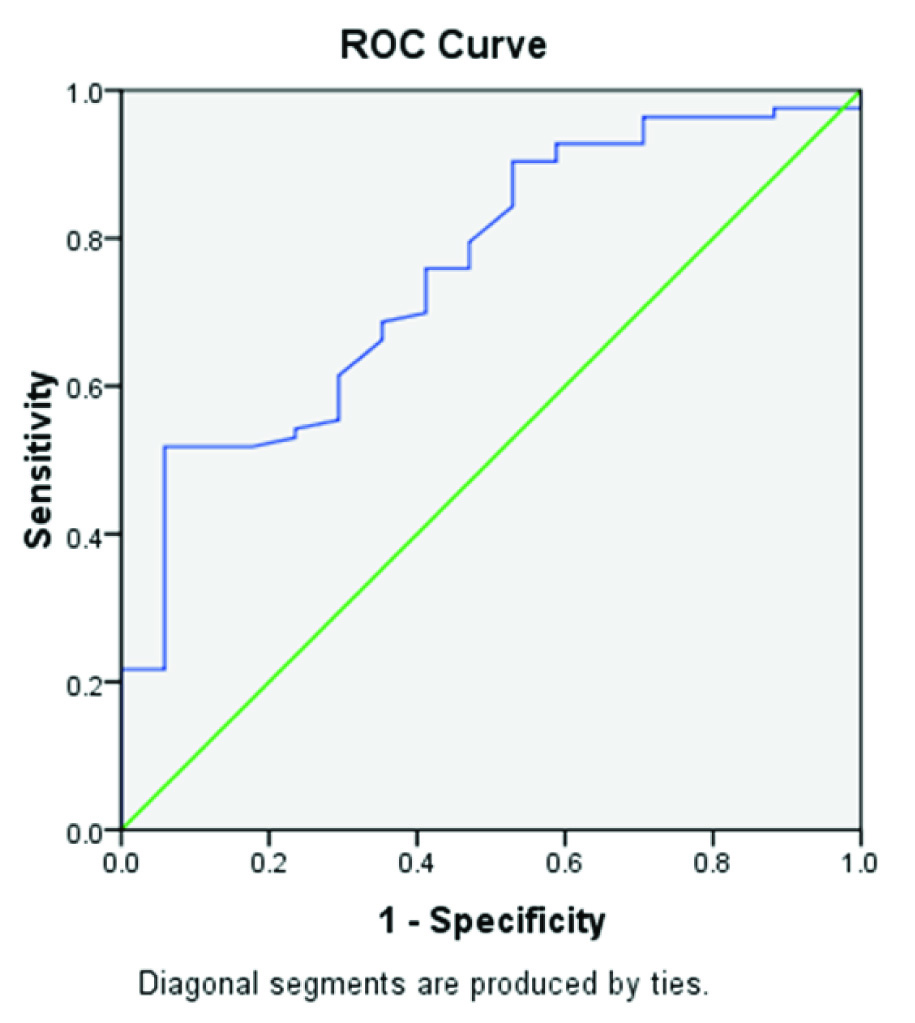
Receiver operating characterstic (ROC) analysis
In the present study by the ROC analysis [Table/Fig-4], a level of FT3 ≤ 2.7 predicted the severity of CAD with a 70% sensitivity and 60% specificity {(area under curve (AUC): 0.755, p=0.001)}.
Discussion
The principal finding of the present study was that, in the absence of primary thyroid disease and acute coronary syndrome, the occurrence of CAD is associated with lower serum levels of FT3. This was observed within the range of physiological values of FT3. In contrast to FT3, thyroid stimulating hormone and FT4 were not observed to be associated with the presence and/or severity of CAD. Moreover, serum FT3 concentrations are also correlated with the Gensini score and independently predict the severity of CAD in euthyroid stable angina patients.
Hypothyroidism, both overt and subclinical, is a well-known risk factor for CAD. But the effect of borderline abnormalities in thyroid function on the coronary circulation remains a matter of debate. Various mechanisms have been postulated for cardiovascular risks in hypothyroidism like impaired cardiac contractility and diastolic function, increased systemic vascular resistance, hypercholesterolemia, C-reactive protein, homocysteine and decreased endothelial-derived relaxation factor. The hypothesis that variation of thyroxine concentrations within the statistical normal range may influence disease and outcome is not entirely new [8]. Bunevicius et al., could demonstrate that tri-iodothyronine administration may improve psychological wellbeing while maintaining thyroid function broadly within the reference range [9].
There have been many studies which have shown a variable relationship between the thyroid function and coronary artery disease. A study by Peters et al., examined thyroid functions in a total of 1049 patients immediately following emergency medical admission [10]. Their study concluded that an elevation in serum FT3 levels at the time of hospital admission was associated with a 2.6-fold greater likelihood of the presence of a coronary event. An elevated FT3 level at admission was associated with a 3-fold higher risk of developing a subsequent coronary event during the next three years. Auer et al., analysed 100 patients referred for coronary angiography and had found that a variation of the thyroid function even within the normal range may influence the presence and severity of coronary atherosclerosis. They reported that lower levels of serum FT4 and higher levels of TSH were associated with severe coronary atherosclerosis; however they did not use Gensini scoring system [11]. Jung et a., who studied 192 patients showed that elevated serum FT4 levels even within normal range could be a risk factor for CAD. However we did not find an association between FT4 and CAD [12]. Coceani et al., studied 1047 clinically and biochemically euthyroid patients reported that serum FT3 levels were inversely correlated with the presence of CAD and the low T3 syndrome conferred an adverse prognosis, even after adjusting for the traditional coronary risk factors [13]. Coceani et al., conducted a study on 2344 patients and have recently advanced the hypothesis that low T3 exerts an adverse impact on prognosis in LV function, which is not influenced by concomitant amiodarone therapy [14]. Tatar et al., conducted a study on 137 patients and showed that serum FT3 levels were inversely correlated with carotid atherosclerosis and surrogates of arterial stiffness in nondiabetics [15]. In the study done by Ertas F et al., on 119 patients, the TSH and FT4 were not found to be linked to the presence and severity of the CAD, on the other hand free T3 levels are inversely correlated to 12the presence of CAD and that low T3 syndrome confers an adverse prognosis [7].
The present study lends support to the theory advanced by Auer et al., Coceani et al., and Ertas F et al., as FT3 represents the biologically active form of thyroid hormone, an isolated reduction in its levels could constitute a model of abnormal thyroid hormone metabolism acting as a risk factor for CAD in a similar fashion to overt or subclinical hypothyroidism. For example, the prevalence of risk factors, such as dyslipidemia and arterial hypertension, is greater in patients affected by hypothyroidism. Hypothyroidism may also lead to endothelial dysfunction, hypercoagulability, impaired fibrinolysis, hyperhomocysteinemia, systemic inflammation, and platelet abnormalities [4]. Importantly, many of the aforementioned alterations are reversible upon normalization of thyroid function [16] and may be observed even in patients with physiological variations of TSH [17] and FT4 [18]. Whether these same notions hold true for FT3 as well has not been established, but in our population the prevalence of hypercholesterolemia and arterial hypertension did not vary according to FT3 levels. However, we did look into the other risk factors for coronary artery disease and, consequently, we cannot rule out their potential influence on our findings. Interestingly, after multivariate analysis, FT3 emerged as an important risk factor in addition to male gender, arterial hypertension and diabetes, thus pointing to the potential existence of its diverse mechanisms of action.
Baseline clinical and biochemical parameters.
| NON CAD n=45 | CAD n=55 | p-value |
|---|
| Age,yrs | 55.51±9.5 | 58.20±9.1 | 0.15 |
| Male n,% | 22(49) | 41 (75) | 0.08 |
| Diabetes n,% | 12 (26.6) | 34(61.8) | <0.001 |
| Hypertension n,% | 18 (40) | 36(65.4) | 0.009 |
| Smoking n,% | 12 (26.6) | 22 (40) | 0.117 |
| Family history n,% | 3 (6) | 3(5.5) | 0561 |
| Total cholesterol,* mg/dl\ | 166.3±40.5 | 164.15±45.9 | 0.801 |
| LDL,* mg/dl | 102.4±33.5 | 95.6±39.24 | 0.362 |
| TG,† mg/dl | 140.0±110.7 | 144.3±56.1 | 0.802 |
| HDL,* mg/dl | 38.4±10.2 | 37.5±9.6 | 0.632 |
| FT3,* (pg/ml) | 3.05±0.42 | 2.84±0.49 | 0.025 |
| FT4,* (ng/dl) | 1.19±0.18 | 1.16±0.153 | 0.379 |
| TSH,†(uIU/mL) | 2.54±1.32 | 2.47±1.38 | 0.07 |
*Student T-Test was applied to compare mean TC, LDL, HDL, FT3 and FT4 level in CAD and Non CAD group
†Mann-Whitney U-Test was applied to compare mean TG (triglyceride) and TSH levels in CAD and Non CAD group
Predictors of presence of CAD by logistic regression analysis
| Variable | p-value | Odds ratio | 95.0% C.I Lower | 95.0% C.I Upper |
|---|
| Diabetes | <0.001 | 0.13 | 0.047 | 0.388 |
| Hypertension | 0.017 | 0.300 | 0.112 | 0.806 |
| FT3(Pg/Ml) | 0.083 | 0.413 | 0.152 | 1.122 |
| Male Gender | 0.002 | 0.184 | 0.06 | 0.52 |
Predictors of severe CAD by logistic regression analysis
| Variable | p-value | Odds ratio | 95.0% C.I Lower | 95.0% C.I Upper |
|---|
| Diabetes | 0.035 | 3.77 | 1.106 | 12.85 |
| Hypertension | 0.78 | 1.182 | 0.34 | 4.08 |
| FT3(Pg/Ml) | 0.003 | 0.088 | 0.018 | 0.42 |
| Male Gender | 0.46 | 1.477 | 0.42 | 5.1 |
ROC Curve for predicting the severity of CAD
Limitations
This study has few limitations. Firstly, being a crossectional study, there is no prospective arm in the study to establish a causal role. Thus any conclusion from this study could be best considered as suggestion for association rather than hypothesis proving. The other limitation is a small sample size and inhomogenous cohort. Thirdly, coronary angiography being a luminogram is not the ideal technique to quantify atherosclerosis.
Conclusion
Serum FT3 concentration is inversely correlated with the severity of CAD in euthyroid patients referred for coronary angiography. Serum FT3 concentrations also correlate with the Gensini score and independently predict the severity of CAD. Thus, FT3 and not the FT4 and TSH levels may be used as an indicator of increased risk for severe CAD. The low T3 state could be at first interpreted as just a biological risk factor of severe coronary artery disease and not as a direct causal factor. Further studies on a larger number of patients are needed to confirm the relationship between the thyroid function and CAD. Mild forms of thyroid disease and even variations of thyroid hormone within the physiological range have been linked to adverse cardiovascular prognosis, hence thyroid hormones should be examined as continuous variable.
*Student T-Test was applied to compare mean TC, LDL, HDL, FT3 and FT4 level in CAD and Non CAD group†Mann-Whitney U-Test was applied to compare mean TG (triglyceride) and TSH levels in CAD and Non CAD group
[1]. GJ Canaris, NR Manowitz, G Mayor, EC Ridgway, The Colorado thyroid disease prevalence studyArchives of internal medicine. [Research Support, Non-U.S. Gov’t] 2000 160(4):526-34. [Google Scholar]
[2]. AE Jarlov, B Nygaard, L Hegedus, SG Hartling, JM Hansen, Observer variation in the clinical and laboratory evaluation of patients with thyroid dysfunction and goiterThyroid : official journal of the American Thyroid Association 1998 8(5):393-98. [Google Scholar]
[3]. LE Braverman, D Cooper, Werner & Ingbar’s The Thyroid: A Fundamental and Clinical Text 2012 7th EditionWolters Kluwer Health [Google Scholar]
[4]. AR Cappola, PW Ladenson, Hypothyroidism and atherosclerosisJ Clin Endocrinol Metab 2003 88(6):2438-44. [Google Scholar]
[5]. PN Taylor, S Razvi, SH Pearce, CM Dayan, Clinical review: a review of the clinical consequences of variation in thyroid function within the reference rangeJ Clin Endocrinol Metab 2013 98:3562-71. [Google Scholar]
[6]. GG Gensini, A more meaningful scoring system for determining the severity of coronary heart diseaseThe American journal of cardiology 1983 51(3):606 [Google Scholar]
[7]. F Ertas, H Kaya, MS Soydinc, Low serum free triiodothyronine levels are associated with the presence and severity of coronary artery disease in the euthyroid patients: an observational studyAnadolu kardiyoloji dergisi : AKD = the Anatolian journal of cardiology 2012 12(7):591-6. [Google Scholar]
[8]. G Michalopoulou, M Alevizaki, G Piperingos, D Mitsibounas, E Adamopoulos, High serum cholesterol levels in persons with ‘high-normal’ TSH levels: should one extend the definition of subclinical hypothyroidism?EuropeanJournal of Endocrinology / European Federation of Endocrine Societies 1998 138(2):141-45. [Google Scholar]
[9]. R Bunevicius, G Kazanavicius, R Zalinkevicius, AJ Prange, Effects of thyroxine as compared with thyroxine plus triiodothyronine in patients with hypothyroidismThe New England journal of medicine 1999 340(6):424-29. [Google Scholar]
[10]. A Peters, M Ehlers, B Blank, D Exler, C Falk, T Kohlmann, Excess triiodothyronine as a risk factor of coronary eventsArch Intern Med 2000 160(13):1993-99. [Google Scholar]
[11]. J Auer, R Berent, T Weber, E Lassnig, B Eber, Thyroid function is associated with presence and severity of coronary atherosclerosisClin Cardiol 2003 26(12):569-73. [Google Scholar]
[12]. CH Jung, EJ Rhee, HS Shin, SK Jo, JC Won, CY Park, Higher serum free thyroxine levels are associated with coronary artery diseaseEndocrine journal 2008 55(5):819-26. [Google Scholar]
[13]. M Coceani, G Iervasi, A Pingitore, C Carpeggiani, A L’Abbate, Thyroid hormone and coronary artery disease: from clinical correlations to prognostic implicationsClinical cardiology 2009 32(7):380-85. [Google Scholar]
[14]. M Coceani, S Molinaro, M Scalese, P Landi, C Carpeggiani, A L’Abbate, Thyroid hormone, amiodarone therapy, and prognosis in left ventricular systolic dysfunctionJournal of endocrinological investigation 2011 34(6):e144-48. [Google Scholar]
[15]. E Tatar, F Kircelli, G Asci, JJ Carrero, O Gungor, MS Demirci, Associations of triiodothyronine levels with carotid atherosclerosis and arterial stiffness in hemodialysis patientsClinical journal of the American Society of Nephrology : CJASN 2011 6(9):2240-46. [Google Scholar]
[16]. S Razvi, L Ingoe, G Keeka, C Oates, C McMillan, JU Weaver, The beneficial effect of L-thyroxine on cardiovascular risk factors, endothelial function, and quality of life in subclinical hypothyroidism: randomized, crossover trialJ Clin Endocrinol Metab. 2007 92(5):1715-23. [Google Scholar]
[17]. BO Asvold, T Bjoro, TI Nilsen, LZ Vatten, Association between blood pressure and serum thyroid-stimulating hormone concentration within the reference range: a population-based study J Clin Endocrinol Metab 2007 92(3):841-5. [Google Scholar]
[18]. E Bruckert, P Giral, R Chadarevian, G Turpin, Low free-thyroxine levels are a risk factor for subclinical atherosclerosis in euthyroid hyperlipidemic patientsJ Cardiovasc Risk 1999 6(5):327-31. [Google Scholar]