Materials and Methods
A prospective study of 310 patients having upper gastrointestinal disorders with clinical diagnosis of acute and chronic gastritis were included in this study over a period of 19 months from July 2013 to January 2015 in Department of Pathology in ACPM Medical college Dhule, India. Patients with history of drugs like NSAIDS, chronic tobacco use and chronic alcoholic were excluded from this study.
After the informed written consent, videogastroscopy was performed with Olympus GJ-140 gastroduodenescope and biopsy was taken from the antral and posterior wall of the stomach. The endoscopic gastric biopsy specimens were already fixed in 10% formalin overnight processed and embedded in paraffin wax. Four micron thick sections were taken and stain with regular Haematoxylin and Eosin stain. Besides studying the biopsy specimens for morphological changes under low and high power magnification, all slides were screened under oil emulsion for the presence of bacterial organisms. After identification if spiral, coiled shaped bacteria in the specimens they were stained with Giemsa stain. The results and observation were organised and interpretated in light of clinical, gender and pathological findings.
Results and Observations
In the present study, a total of 310 patients with symptoms of vague chest pain, postprandial pain, intermittent vomiting and epigastric discomfort were subjected to endoscopy. On videogastroscopic examination signs of gastritis were noted and biopsy from the antrum was taken. Taking Histopathology as the gold standard for diagnosis, presence and absence of H.pylori and morphological changes due to H.pylori associated gastritis were studied in 310 cases and following results were obtained.
In total 310 cases of chronic gastritis, the most common age of incidence was 31 to 40 years with male predominance. The male to female ratio was 1.07:1 as per [Table/Fig-1,2]. This was in concordance with Yakub MY et al., [8].
Sex distribution of gastritis patients
| Gender of the patient | No. of patients |
|---|
| Male | 160 (51.6%) |
| Female | 150 (48.4%) |
| Total | 310 (100%) |
Age distribution of gastritis patients
| Age groups | No. of patients |
|---|
| 10-20 | 15 (4.8%) |
| 21-30 | 63 (20.2%) |
| 31-40 | 115 (36.8 %) |
| 41-50 | 63 (20.2%) |
| 51-60 | 35 (11.7%) |
| >61 | 19 (6.3%) |
| Total | 310(100%) |
H.pylori was detected in 144/310 (46.5 %) specimens of gastritis. The 166/310 (53.5%) cases were negative by histopathological method [Table/Fig-3]. This was comparable to figures of 48%, 50.4% and 66.9% from other studies from India by Dandin AS et al., [9], Satoskar A et al., [10] and Maitra TN et al., [11] respectively. The study conducted in Pakistan by Yakub MY et al., [8] showed 62.5% of H.pylori associated gastritis. In Bangladesh, 45.6% of H.pylori gastritis was observed by Akanda MR [12]. Abu- Ahmed NM et al., [13] in Jordan showed 67% of H.pylori positive patients in view small sample size. Rest are comparable in [Table/Fig-4].
Histopathological impression
| Histopathological Findings | Total no. of biopsies |
|---|
| H.pylori Positive | 144 (46.5 %) |
| H.pylori Negative | 166 (53.5 %) |
| Total | 310 (100 %) |
Comparative study of H.pylori associated gastritis
| 1) Satoskar A et al., [10] | 50.4 % |
|---|
| 2) Maitra TN et al., [11] | 66.9 % |
| 3) Yakub MY et al., [8] | 62.5 % |
| 4) Akanda MR et al., [12] | 45.6 % |
| 5) Abu- Ahmed NM et al., [13] | 67.0 % |
| 6) Dandin AS et al., [9] | 48.0 % |
| 7) Present study | 46.5 % |
Our results were concordance with Dandin AS et al., [9] and Akanda MR et al., [12] from India and Bangladesh respectively. In a study by Singhal AK [14] quoted prevalence with a wide range of 31-84%
Prevalence of H.pylori associated gastritis and morphological changes due to bacillus was noted by Hui Pak et al., [15]. Irregular epithelial surface and loss of apical mucin was noted in 161/310 cases with lymphoid aggregates in 125/310 cases. Reactive atypia was seen in 24/310 cases as in [Table/Fig-5]. H.pylori may produce gastric epithelial cell damage directly or by stimulating host immune response. Adherence of the organism produces loss of microvilli and irregularity of the luminal border [8]. It is also known to release vacuolating cytotoxins and enzymes including urease, which has toxic effects on the epithelium. Lymphoid aggregates were significantly more frequent (40.2%) finding in H.pylori infected slides [Table/Fig-1,2].The normal human stomach is devoid of organised MALT. The significant association of H.pylori and MALT indicates that the bacterium may induce local humoral and T-cell response in the gastric mucosa. H.pylori infection triggers the development of MALT tissue, which can act as a nidus in which a lymphoma might develop [8].
Histopathological finding in H.pylori gastritis patients
| HPE findings | No. of patients |
|---|
| Irregular surface mucosa and loss of apical mucin | 161 (52.08%) |
| Lymphoid aggregates | 125 (40.27%) |
| Reactive atypia | 24 (7.65%) |
| Total | 310 (100%) |
Discussion
The overall prevalence of gastritis by H.pylori in North Maharashtra using antral biopsies was 46.5%, which was consistent with recent studies in India and Bangladesh [9,12] respectively. Thus histopathological evaluation can be considered as gold standard technique for the demonstration of H.pylori in the biopsy specimen. The only disadvantage of this technique is the need for endoscopy to obtain the tissue. However, histopathological sampling does allow for the definitive diagnosis of infection, as well as degree of inflammation or metaplasia, presence and absence of MALT lymphoma and other gastric cancers in high risk patients [2].
A bewildering array of test are now available, which include urease breath test, rapid urease test, bacterial culture, serological test, PCR and molecular techniques, but most techniques are plagued by lack of specificity and sensitivity or are limited in use due to their exorbitant cost and inaccessibility [4]. Because of H.pylori is difficult to grow in culture media, the role of culture in diagnosis is limited mostly to research and epidemiological considerations. PCR allows identification of organisms in small samples with few bacteria present with major limitation of a few laboratories currently has the capacity to run the assay and it has false positive and negative results. Rapid urease takes the advantage of the fact that H.pylori is urease producing organism in view of inexpensive, fast and widely available. But also limited in value due to the false positive results, decrease urease activity and affection by drugs [2]. Serological test now a day's offer a fast, easy and relatively inexpensive methods of identifying infection with organism. However, this method is not useful means of confirmation and eradication of H.pylori.
Hence, keeping all above points, we undertake the histopathological method to diagnose and confirm the patients of H.pylori associated gastritis. In our study, the H.pylori was further confirmed by Giemsa method in doubtful cases only. So, it’s better useful to confirm other than H.pylori bacillus like Gastrospirillum Hominis. Gastritis due to spiral shaped bacteria other than H.pylori were also there as per Heilmann KL et al., [16]. But on scanning and transmission electron microscopy shows bacteria which invade and damage gastric mucosal cells. In contrast to H.pylori they were straight, less populated and invasive [16]. Misra V et al., [17] used Loeffler's methylene blue (a counter-stain for acid fast bacilli) to detect Helicobacter pylori in paraffin sections and touch smears of gastric mucosal biopsies from 15 patients with duodenal ulcer and 35 with non-ulcer dyspepsia. The Loeffler's methylene blue method was found to be simpler, quicker and cheaper than the modified Giemsa stain as per Misra V et al., [17].
Histopathologically, H.pylori is short, curved or spiral bacilli resting on the epithelial surface or in the mucus layer of gastric mucosa. It is also found deep into the gastric pits. The morphological changes, we observed are presence of irregular mucosa, loss of apical mucin and lymphoid aggregates seen with reactive atypia [Table/Fig-6,7]. After the treatment, the density of H.pylori is lowered or even absent and the shape of bacteria may be changed from spiral into round, coccoid or vibrio shape [Table/Fig-8]. Apart from gastritis, two cancers associated with H.pylori are gastric adenocarcinoma and MALT lymphoma [18]. In an extensive review of gastric cancer and H.pylori confers an approximately six fold risk of gastric cancer, accounting for about half of all the gastric cancers [19]. MALT lymphoma is associated with H.pylori in 80% of cases as per Issacson PG [20]. Hence, confirmation of diagnosis by histopathology always warranted to avoid above consequences.
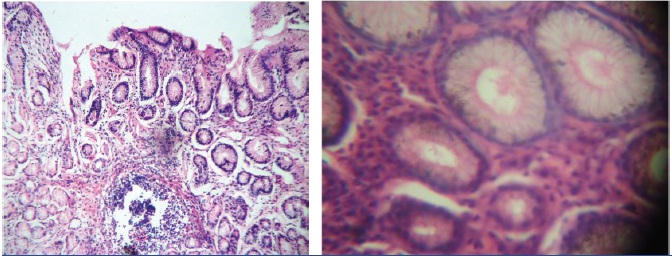
Microphotograph showing gastric mucosa with irregular surface and lymphoid aggregates.(H&E, x100 and x400)
Microphotograph showing spiral, round bacilli inside the lumen of gastric glands. (H&E,x1000)

In our study, the diagnosed cases were underwent medical treatment, in view of its etiology; first known bacteria as carcinogen that is H.pylori. Eradication of bacteria can be achieved by triple therapy comprising of Clarithromicin, Amoxycillin and Tinidazole or Lansaparozol, Clarithromicin and Metronidazole etc. In our study, in follow upto 6 months, 70% of the symptoms were relieved by medical treatment.
Conclusion
We conclude that H.pylori infection is not uncommon in North Maharashtra, India. A high prevalence of 46.5% H.pylori associated gastritis was noted in our study in gastritis patients. The prevalence of duodenal ulcer is high in North Maharashtra and the high prevalence of H.pylori might suggest a role in its pathogenesis. Early and definitive diagnosis of this organism by histopathology can help by initiating proper antibacterial therapy for the eradication of these bacilli and thus have major implications in patient recovery. More population based studies are required to evaluate H.pylori role in other gastrointestinal disorders in this region.