Background
Nasal cavity and Paranasal sinus malignancies are very rare, in which maxillary sinus is the commonest, followed by ethmoid, frontal and sphenoid sinus. Computed Tomography (CT) & Magnetic Resonance Imaging (MRI) play a key role in diagnosis, staging and management of paranasal sinuses and nasal pathologies. Multiplanar imaging in CT helps better imaging of critical anatomical areas. Aim of our study was to study the incidence, clinical features, CT features and its importance in the management of sinonasal neoplasms.
Materials and Methods
This prospective study was carried out in a tertiary care hospital of MP, India. Consecutive 40 histologically proven cases of sinonasal neoplasia who visited the Department of Otorhinolaryngology and Radiotherapy are included in our study. Demography and clinical features were recorded. Cases of nasal and paranasal sinus masses diagnosed on CT attending ENT and Radiotherapy OPD or admitted in the Radiotherapy ward forms the material of this study. This included patients of both sexes and all ages. Histopathological examination was asked to confirm the diagnosis made on CT.
Results
There were total 40 cases of sinonasal neoplasia among which 24 were benign. Almost all the benign cases were seen in the age group <40 y with mean age of 20 y and most of the malignant cases were seen in the age group above 40 y with mean age of 55 y. In our study we found male preponderance with male female ratio of 4:1 in both benign and malignant conditions. The commonest presenting symptoms of the patients with sinonasal masses in our study was nasal obstruction (75%) and nasal discharge (67.5%) followed by nasal mass (65%), epistaxis (62.5%) and headache (60%). Angiofibroma and papilloma were the commonest benign lesions. Commonest malignant lesion was squamous cell carcinoma. Of the malignant Sinonasal tumours studied in our series, maxillary sinus was involved in 13, ethmoid sinuses and nasal cavity in 10 cases each, and frontal sinuses in 2 cases.
Conclusion
Contrast enhanced computed tomography with multiplanar reconstruction is an excellent modality for imaging sinonasal masses. CT can define the character of the sinonasal mass, thus differentiating benign from malignant. CT helps better imaging of critical anatomical areas and helpful in planning treatment procedures such as surgery and radiotherapy.
Introduction
Tumours of sinonasal cavities are rare, and sinonasal malignancies comprise only 3% of all head and neck cancers and 1% of all malignancies, with a peak incidence in the 5th to 7th decades and with a male preponderance [1]. The Sinonasal tract plays host to an enormous variety of neoplasm derived from a multitude of tissue types. Both epithelial and nonepithelial neoplasms arise from the nose and paranasal sinuses, in which epithelial part predominates. Epithelial neoplasia may arise from the mucosa, minor salivary tissue or olfactory mucosa. Each of the mesenchymal tissue of the sinonasal tract can give rise to benign and malignant neoplastic components.
Due to the complex anatomy of the region and usual clinical symptoms of rhinosinusitis such as nasal blockage, rhinorrhea, lacrimation and epistaxis and therefore neglected both by the patients and doctors, more than 50% of the tumours would have reached an advanced stage with a poor prognostic outcome at the time of diagnosis [2,3].
In older days plane X-ray and tomography has failed to delineate the lesion with precision in these critical areas. The incapability in most instances made the disease to progress to a very advanced stage where the treatment was only confined to debulking.
Modern imaging like CT & MRI played a revolutionary role to diagnose the disease early, plan the treatment and picking up the metastasis. The local extension of the disease to the areas like the skull base, the orbit and intracranial compartment could be made with absolute precision. The information gained through these modern imaging could permit a realistic treatment planning and subsequent follow up. MRI is better modality in evaluation of sinonasal tumours due to brilliant visualization of soft tissue lesions, bone marrow changes and perineural spread of disease which is more common in head and neck malignancies. Signal characteristics of the lesions in MRI may help to differentiate a mass from inflammatory pathology and retained secretion. However, CT scan is more commonly used modality for sinonasal pathology. It is easily available, cheaper, take less imaging time, and best modality to assess the bony changes. Bony destructions and presence of calcifications are poorly demonstrated by MRI [4].
Materials and Methods
This prospective study was carried out in a tertiary care hospital of Madhya Pradesh, India between 2007 January to 2008 December. Cases of nasal and paranasal sinus masses diagnosed on CT attending ENT and Radiotherapy OPD or admitted in the Radiotherapy ward forms the material of this study. This included patients of both sexes and all ages. The detailed history as per the proforma was noted. The chief complaints such as nasal obstruction, nasal discharge, nasal mass, epistaxis, facial asymmetry, headache, aural symptoms and loosening of tooth etc. were noted.
Computed Tomographic Evaluation : CT evaluation was done with SIEMENS Somatom plus (single slice spiral) and Somatom volume zoom (Quad slice). Scanning was done in the spiral/sequence mode, both in the axial and coronal sections with 5 mm slice thickness in Somatom plus and only axial sections were taken in Somatom volume zoom (Quad slice), coronal images were reconstructed from axial images. Initially non-contrast enhanced scans were obtained from the sphenoid to the frontal sinuses. Any signs of mass lesions involving the nasal cavity and paranasal sinuses were carefully looked for. Any abnormal foci of calcification within the mass lesion or bone changes were carefully evaluated. Bony changes and calcification were viewed at wide window settings.
Evidence of bone remodeling, erosions or destructions were looked for at a wide window setting. Key areas like the bony orbital walls, cribriform plate, fovea ethmoidalis, and posterior wall of the maxillary sinus, pterygopalatine fossa, the sphenoid sinus and the posterior table of the frontal sinus were carefully evaluated.
Intravenous nonionic contrast medium was administered as a single bolus and scanning was commenced in the caudo-cranial or antero-posterior direction depending on whether axial or coronal study was done. The enhancement pattern of the mass lesion, their site of involvement and extension into adjacent structures were noted. Inflammatory masses were excluded from the study.
Results
There were total 40 cases of sinonasal neoplasia among which 24 were benign. Almost all the benign cases were seen in the age group <40 y with mean age of 20 y and most of the malignant cases were seen in the age group above 40 y with mean age of 55 y.
A bimodal age distribution (2nd and 5th decades) was seen in the cases of Sinonasal lymphoma. One case of Rhabdomyosarcoma was diagnosed in a patient of 40 y. In our study we found male preponderance with male female ratio of 4:1 in both benign and malignant conditions. The commonest presenting symptoms of the patients with Sinonasal masses in our study was nasal obstruction (75%) and nasal discharge (67.5%) followed by nasal mass (65%), epistaxis (62.5%) and headache (60%). Angiofibroma and papilloma contributes the majority of the benign lesions [Table/Fig-1].
Commonest malignant lesion was squamous cell carcinoma [Table/Fig-2]. Of the malignant Sinonasal tumours studied in our series, maxillary sinus was involved in 13 cases (81.25%), ethmoid sinuses and nasal cavity in 10 cases (62.5%) each, and frontal sinuses in 2 cases (12.5%).
Spectrum of CT Findindgs: Both benign and malignant lesions revealed HU values in the range of 26-60. In case of malignant lesions, complete opacification of sinuses were frequently observed.
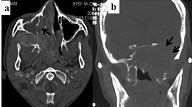
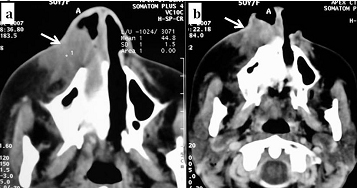
Almost all the benign case shows bone deformity and erosion. Bony abnormality most commonly seen in cases of malignant sinonasal tumours was destruction (12 in our cases) [Table/Fig-3a,b]. However, lymphoma cases showed mild expansion, remodeling and mild erosion of adjacent bones.
Most of the cases of juvenile angiofibroma in our study shows deformity of the base of the ipsilateral medial Pterygoid lamina [Table/Fig-4a,b] and anterior bowing of the posterior wall of the maxillary sinus (Holman – Miller sign)
Enhancement pattern of the benign and malignant lesions varied depending on the nature of the lesion. All the cases of Nasopharyngeal angiofibroma showed characteristic intense homogenous post-contrast enhancement.
Inverted papillomas are commonly seen as expansile soft tissue mass in nasal cavity. Five cases arise from lateral nasal wall and two cases from nasal septum. None of them shows calcification. Focal area of Sclerosis was seen in two cases of inverted pailloma which can be used as a predictor of Tumour Origin site and is helpful during surgery to avoid recurrence [Table/Fig-5a,b].
Two cases of of osteoid osteoma were seen in Frontal sinus as bone density masses and both of them were incidental not obstructing the drainage pathway [Table/Fig-6].
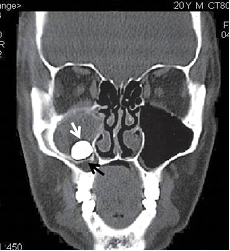
Odontogenic lesions presenting as maxillary sinus mass was seen in two cases. They appeared as well defined expansile mass in relation to floor of maxilla; a thin cortical rim was seen separating the lesion from sinus lumen in both the cases. Presence of tooth within the lesion is diagnostic of dentigerous cyst [Table/Fig-7].
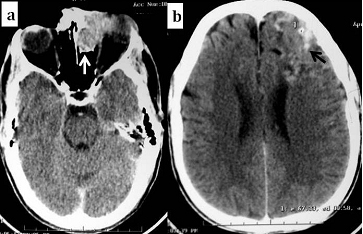
One case of paraganlioma was seen as intensely enhancing mass in ethmoid sinus extending into the frontal sinus. Prominent vessels were noted in adjacent anterior cranial fossa [Table/Fig-8a,b].
One case of brown tumour of hyper parathyroidism was seen as an expansile mass with internal calcification in the left maxillary sinus [Table/Fig-9a,b].
Sino nasal lymphomas are seen as mildly enhancing homogeneous soft tissue density mass on both sides of sinus wall causing remodeling and mild erosion of adjacent bones [Table/Fig-10a,b].
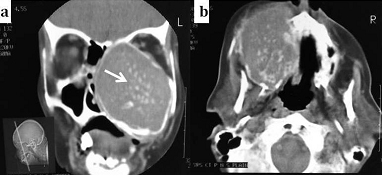
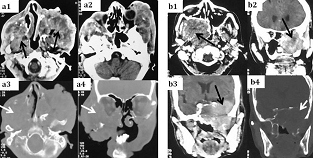
The malignant lesions showed variable enhancement with a few showing ill defined areas of low density within the lesions, indicating areas of necrosis. In our study squamous cell carcinoma [Table/Fig-11a] and adenocarcinoma [Table/Fig-11b] were indistinguishable on CT findings both appear as aggresive heterogeneously enhancing masses showing necrotic areas and extensive bony destruction.
Soft tissue mass extending beyond the areas of origin was seen in all the cases of malignant Sinonasal tumours especially the squamous cell carcinoma and adenocarcinoma. In our study malignant tumours showed extension to orbits in 8 cases, infratemporal fossa in 5 cases and Nasopharynx in 2 cases. 1 case of paraganglioma, 1 case of esthesioneuroblastoma, 1 case of squamous cell carcinoma and 1 case of adenocarcinoma were showing Intracranial extension (4 cases). Level II and III are the commonly involved cervical lymph node groups in our study.
Discussion
Benign sinonasal tumours are most commonly seen in the second decade. Nasopharyngeal angiofibroma and Papilloma remain most common among them. Malignant sinonasal lesions are common in the 5th and 6th decade. Squamous cell carcinoma is the commonest among them. These correlates well with most of the previous studies (Chatterjee et al., and Lathi et al.,) [5,6]. Among the 4 cases of lymphoma 2 were Hodgkins and other 2 were Non Hodgkins lymphoma. Hodgkins Lymphoma showed bimodal age distribution (2nd decade and 5th decade), however Non Hodgkin lymphoma cases were seen in 6th and 7th decade. Rhabdomyosarcoma in the adults most commonly seen in 4th and 5th decade and correlates well with the study done by Steven D et al., on adult Rhadomyosarcoma 3[7]. Our study also showed male preponderance for sinonasal masses with male to female ratio of 4:1 similar to other studies [5,6,8]. Nonspecific symptoms like nasal obstruction and nasal discharge were commonest presenting symptoms of any sinonasal neoplasms followed by nasal mass, epistaxis and headache [6]. Similar observation was made in other studies which results in delay in diagnosis.
Nasopharyngeal angiofibromas can be diagnosed by their typical location and characteristic enhancement in adolescent male [4,9]. All the cases of nasopharyngeal angifibromas were arising from sphenopalatine foramen and causing anterior bowing of the posterior wall of the maxillary sinus (Holman – Miller sign) which was well correlated with studies [4,9]. Inverted papillomas are seen in the nasal cavity originating either from lateral nasal wall or septum and sometimes focal sclerosis at the site of origin. Two cases of inverted papilloma showed sclerosis at the site of origin which correlates well with the study by D K Lee et al., [10]. Osteoma appears as dense cortical bone density lesion and CT demonstrate its relationship with mucociliary drainage pathways [1]. These type of dense bony lesions are better demonstrated by CT rather than MRI. Because in MRI dense bony lesions will be difficult to identify in the air filled sinus cavity but better seen in CT. Dental pathologies like dentigerous cysts and odontogenic keratocysts can extend into maxillary sinus and mimics sinonasal neoplasia. Presence of tooth in a cystic lesion is diagnostic of dentigerous cyst. On CT Malignant lesions appears as heterogeneously enhancing soft tissue density masses completely filling the sinus cavity with extensive destruction of bones and extending into adjacent areas. Esthesioneuroblastoma usually arises from superior nasal fossa, extends into paranasal sinuses and anterior cranial fossa. CT features of this aggressive tumour are similar to squamous cell carcinoma and can be diagnosed only based of histopathology. Intracranial extension of sinonasal tumours are commonly seen in esthesioneuroblastoma, paraganlioma, squamous cell carcinoma and adenocarcinoma types, anterior cranial fossa is involved almost all the cases. Level – I, II and III lymph nodes and retropharyngeal lymph nodes are commonly involved in Sinonasal malignancies [1]. Lymphomas appear as diffusely infiltrating masses along the walls of nasal cavity, homogeneous soft tissue density masses on both sides of sinus wall causing remodeling or erosion of bones [1,11]. All the cases of lymphoma in our study shows homogeneous infiltrating masses along both sides of bones with smooth erosions which correlate well with the studies by Heidi B et al., [1] and Sander et al., [11]. Long standing thick mucus secretions are difficult to differentiate from mass lesions sometimes on CT but can be well differentiated on MRI. Perineural spread of malignancy cannot be demonstrated which is commonly seen in head and neck malignancy. MRI is the modality of choice to demonstrate the perineural spread of disease. However, CT has more advantages than MRI in demonstrating calcification, and bone destruction, cost effectiveness and easy availability. Hence, CT can be considered as first line of investigation in any sinonasal neoplasia.
List and number of benign cases
| Histology (Benign Lesions) | No. of cases |
|---|
| Angiofibroma | 10(41.6%) |
| Papilloma | 7(29%) |
| Paraganglioma | 1(4%) |
| Brown tumor of hyperparathyroidism | 1(4%) |
| Osteoma | 2(8%) |
| Odontogenic keratocyst | 1(4%) |
| Dentigerous cyst | 1(4%) |
| Hemangioma | 1(4%) |
List and number of malignant cases
| Histology (Malignant Lesions) | No. of Cases |
|---|
| SCCA | 7(43%) |
| Adenocarcinoma | 2(12%) |
| Lymphoma | 4(25%) |
| Rhabdomyosarcoma | 1(6%) |
| Esthesioneuroblastoma | 1(6%) |
| Malignant melanoma | 1(6%) |
CT sections in bone window showing typical bone changes (black arrows) such as remodeling (a) in benign and destruction, (b) in malignant cases
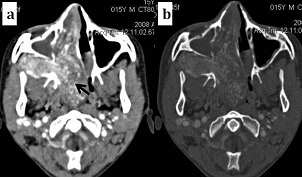
Nasopharyngeal Angiofibroma - CT axial images showing intensely enhancing soft tissue mass (black arrows) in the sphenopalatine fossa & nasopharynx and causing widening the Pterygopalatine fossa
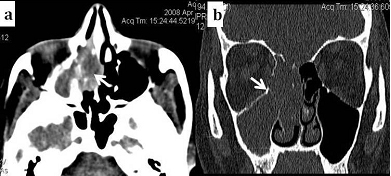
Inverted Papilloma - CT axial (soft tissue window - a) & coronal(bone window - b) images showing soft tissue density mass seen involving ethmoidal sinus, nasal cavity and extending into maxillary sinus
Osteoma - CT coronal image showing a cortical bone density lesion in the frontal sinus
Dentigerous Cyst - CT coronal images showing an expansile mass in relation to floor of maxillary sinus with a tooth (white arrow) seen at the base and a thin cortical rim (black arrow) was separating the lesion from sinus lumen
Paraganglioma - CT axial images showing enhancing ethmoidal mass (white arrow) extending into frontal sinus & anterior cranial fossa showing contrast filled blood vessels (black arrow) in the brain parenchyma
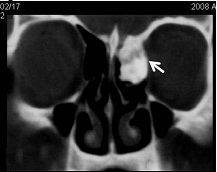
Brown Tumour Of Hyperparathyroidism - CT coronal (a) & axial (b) images showing an enhancing expansile mass with calcification (white arrow) in the left maxillary sinus
Lymphoma - CT axial images showing mass (white arrow) in the nasal cavity & premaxillary area causing mild remodeling without significant erosion
Bilateral Maxillary Squamous cell carcinoma (a1-a4) and Adenocarcinoma of Maxillary Antrum (b1-b4) - CT axial & coronal images showing aggressive heterogeneously enhancing masses (black arrow) with necrotic areas and extensive bony destruction (white arrow)
Conclusion
CT plays a very important role in the management of Sinonasal masses. CT is easily available, cheaper and faster in acquisition of data which prevents movement artefacts in unco-operative patients. No other modality will demonstrate the bony changes in addition to the extent of mass lesion and involvement of other structures like CT. Contrast enhanced computed tomography with multiplanar reconstruction is an excellent modality for imaging sinonasal masses. Although CT cannot reliably differentiate all benign and malignant cases, several imaging findings like location of the lesion, pattern of enhancement and bone involvement in a proper clinical setting can lead to reasonable diagnosis. CT helps better imaging of critical anatomical areas and helpful in planning treatment procedures such as surgery and radiotherapy. Though MRI has several advantages it is costlier, not easily available in all places and contraindicated in patients with pacemakers and cochlear implant.
[1]. HB Eggesb, Imaging of sinonasal tumoursCancer Imaging. 2012 12:136-52. [Google Scholar]
[2]. N Bhattacharyya, Factors affecting survival in maxillary sinus cancerJ Oral Maxillofac Surg 2003 61:1016-21. [Google Scholar]
[3]. C Thorup, L Sebbesen, H Danø, Carcinoma of the nasal cavity and paranasal sinuses in Denmark 1995–2004Acta Oncol 2010 49:389-94. [Google Scholar]
[4]. E Nyberg, SG Nour, JS Lewin, D Hsu, CF Lanzieri, Sinonasal Cavity, Nasopharynx,and Oropharynx. In Haaga JR, et al. editor. CT and MRI of the whole bodyTetracyclineTeratology 2009 15th EditionMosby:P567-89. [Google Scholar]
[5]. P Chatterjee, P Sharma, S Khanna, A Clinicopathological and Radiological Study of Sinonasal MassIndian Journal of Medical Research and Pharmaceutical Sciences 2014 1(5):21-26. [Google Scholar]
[6]. A Lathi, MMA Syed, P Kalakoti, D Qutub, SP Kishve, Clinico-pathological profile of sinonasal masses: a study from a tertiary care hospital of IndiaActa Otorhinolaryngologica Italica. 2011 31(6):372-77. [Google Scholar]
[7]. SD Allen, EC Moskovic, C Fisher, JM Thomas, Adult Rhabdomyosarcoma: Cross-Sectional Imaging Findings Including Histopathologic CorrelationAJR Am J Roentgenol 2007 189(2):371-77. [Google Scholar]
[8]. U Zafar, N Khan, N Afroz, SA Hasan, Clinicopathological study of non-neoplastic lesions of nasal cavity and paranasal sinuses Indian J Pathol Microbiol 2008 51:26-29. [Google Scholar]
[9]. S Mishra, NM Praveena, RG Panigrahi, YM Gupta, Imaging in the diagnosis of juvenile nasopharyngeal angiofibromaJ Clin Imaging Sci 2013 3(Suppl 1):1 [Google Scholar]
[10]. DK Lee, SK Chung, HJ Dhong, Focal Hyperostosis on CT of Sinonasal Inverted Papilloma as a Predictor of Tumour Origin AJNRAm J Neuroradiol 2007 28(4):618-21. [Google Scholar]
[11]. A Sandner, A Surov, AG Bach, S Kosling, Primary Extranodal Non-Hodgkin Lymphoma of the Orbital and Paranasal Region – A Retrospective StudyEur J Radiol 2013 82(2):302-08. [Google Scholar]