Metabolic disorders, such as diabetes and hyperlipidemia are a threat to public health. Though exercise has positive health effects for individuals, efficacy of several types of physical activity interventions is unclear. There is a need to carry out well-designed studies in order to evaluate the effectiveness of physical activity interventions and identify the types of interventions that show the most promise [1]. Regular exercise of moderate intensity is good for maintaining fitness of all systems in the human body [2]. It decreases the blood levels of IL-6 and TNF-α [3]. Exercise also alters the number and function of circulating cells of immune system secreting these cytokines. An increase in leukocyte count is observed during and immediately after exercise, depending on the intensity and duration of exercise [4]. Hence, different levels of exercise can be used as different grades of stress to study the secretion of IL-6 and TNF-α [5]. The change from a physically demanding lifestyle in natural outdoor settings to an inactive indoor lifestyle is the cause for many of the widespread diseases that are endemic in our modern society. The logical solution is to revive human activity pattern to the extent that it is achievable and practical [6]. Hence regular physical activity/yoga can promote better health. Yoga is popular as a stress-relieving therapy because of its greater effectiveness and no associated side effects.
Materials and Methods
Two hundred and eighteen subjects took part in the study. One hundred and nine volunteers (51 males and 58 females) in the age group of 20 to 60 years, who practiced yoga regularly for over five years for a period of one hour daily, performed a bout of moderate exercise and a bout of strenuous exercise. Blood samples were collected between 7 and 8 AM; (a) just before performing exercise (baseline); (b) immediately at the end of one bout of moderate exercise and; (c) at the end of one bout of strenuous exercise, for analysis of IL-6 and TNF-α. Strenuous exercise was performed on a different day. All subjects performed exercise under supervision. Anthropometrically matched, age matched and gender matched subjects, who did not practice yoga (non-yoga group) were chosen as controls (non-yoga, n=109). The non-yoga group also performed similar exercise. Informed written consent was obtained from all the subjects volunteering to participate in the study. The study protocol was approved by the institutional ethics committee.
Sample size estimation was carried out based on a pilot study [10] in which it was found that there was a significant difference in TNF-α between yoga and non-yoga group before and after strenuous exercise. Considering an effect size of 0.4 and with the power of 80 and desired confidence level of 95 percent, the sample size was estimated to be 100 in each group.
The subjects were selected based on the following inclusion and exclusion criteria:
Healthy volunteers between the ages of 20 to 60 years practicing yoga were included in the study. The subjects practicing yoga had performed Asanas/yogic exercises and relaxation techniques, pranayama and meditation regularly for one hour per day for the last five years. Individuals below and above the age range and those suffering from any kind of illnesses including chronic disorders and on long term medication and people who smoked, consumed alcohol and/or illicit drugs in any form were excluded from the study.
The standardized 10 m Shuttle Walk test was the exercise protocol adopted for this study [11,12]. In the 10m Shuttle Walk test, marker cones are positioned at the two ends of a plain 10m long path. The participants in the study start to walk the 10m path once the initial beep is given out by an audio player. The subject has to reach the other cone at the end of the path by the time the next beep is sounded by the audio player. As time progresses, there is a gradual shortening of duration between the beeps. Hence, the participants will have to increase the pace of walking. The heart rate keeps on increasing as time progresses from the beginning of the Shuttle walk. At about 7th to 8th minute, the heart rate increases to 100 to 125 per minute (about 50 percent compared to resting level). This is considered as moderate exercise. At about 11th to 12th minute, the heart rate increases to 125 to 150 per minute, (it doubles or increases by 100 percent). This is considered as strenuous exercise. This is according to the WHO criteria for grading exercise [13]. No adverse events were noted in any of the subjects during the study.
Estimation of IL-6 and TNF - α: The cytokines IL-6 and TNF - α were estimated from serum samples. Estimation was done using the ELISA method as per the procedure given by the manufacturer (Immunotech (France) kit). The serum was incubated in Polystyrene microtiter plates coated with monoclonal capture antibody for two hours. The corresponding biotinylated detection antibody was added after this. Incubation was continued for a further period of 30 minutes. After this, substrate was added. 2N sulphuric acid was added to stop the reaction. Finally, Optical density (O.D) reading was taken (450nm). A standard curve was generated using the standards provided by the manufacturer. The levels of cytokines IL-6 and TNF - α were expressed in pictograms/ml read from the standard curve [14].
Omron Body Composition Monitor, Model No. HBF: 362 (Karada Scan) was used for measurement of BMI, body fat percent, skeletal muscle percent and resting metabolism. This machine measures fat and muscle by using the principle of bioelectrical impedance [15]. Serum cholesterol, triglyceride, HDL, VLDL were determined by using reagent kits obtained from Agappe Diagnostics. Its value was expressed as mg/dl. A semi-autoanalyser was used for its estimation.
Statistical Analysis
Data of all the TNF- α, IL-6, lipid profiles were expressed in terms of descriptive statistics like mean±SD. In view of non normality of the data, variables like TNF- α at baseline, TNF- α after one bout of moderate exercise, TNF- α after one bout of strenuous exercise, IL-6 at baseline, IL-6 after one bout of moderate exercise, IL-6 after one bout of strenuous exercise were converted to logarithmic transformation for the purpose of analysis. In order to test for statistical significance of differences in the mean values of each of these parameters at different time points, repeated measures of ANOVA was employed (i.e. to analyse the differences between the different grades of exercise in both the groups). Further, pair wise differences were tested using Bonferronis test. Pearsons correlation was used to find the correlation between BMI and TNF-α values and IL-6 values. Multiple linear regression was employed to predict the values of TNF-α and IL-6 on the basis of independent predictors like age, gender and BMI. Logarithmic transformation was carried out for the IL-6 and TNF- α values as the data was not normally distributed. Student t-test was applied to analyse the differences in values between cholesterol, BMI and the other variables which were measured only once in both the groups. p<0.05 was considered to be significant.
Results
Resting TNF-α and IL-6 levels were lower in yoga group when compared to the non-yoga group: the difference in TNF-α levels was significant (p < 0.05). There was a significant increase in both TNF-α and IL-6 after moderate exercise and strenuous exercise in the non-yoga group when compared with yoga group [Table/Fig-1,2]. This indicates that the yoga group exhibits reduced inflammatory response as evidenced by lower levels of TNF- α and IL-6. In the non-yoga group, there is significant difference in the IL-6 as well as TNF-α levels between baseline and post exercise (both moderate and strenuous) values. However this difference was not observed in yoga group, indicating that the non-yoga group does show significant increase in the levels of the pro-inflammatory cytokines with physical stress [Table/Fig-3,4].
Comparison of TNF-α levels (pg/ml) between groups, with each level of exercise
| Exercise | Non-yoga/Control (n=109) | Yoga (n=109) |
|---|
| Mean ± SD | Median | Mean ± SD | Median |
|---|
| 1.Baseline (Before) (Log transformation) | 79.64±33.91 (1.86±0.02) | 79.00 | 55.34±23.36* (1.70±0.02) | 53.60 |
| 2.After Moderate (Log transformation) | 112.78±48.95 (2.02±0.02) | 111.20 | 63.07±31.29* (1.75±0.02) | 60.60 |
| 3.After Strenuous (Log transformation) | 204.17±120.87 (2.24±0.02) | 199.00 | 75.49±61.62* (1.81±0.02) | 73.00 |
*p<0.05 statistically significant
Comparison of IL-6 levels (pg/ml) between groups, with each level of exercise
| Exercise | Non-yoga/Control (n=109) | Yoga (n=109) |
|---|
| Mean ± SD | Median | Mean ± SD | Median |
|---|
| 1.Baseline (Before) (Log transformation) | 29.12±17.99 (1.38±0.03) | 28.40 | 22.60±19.9 (1.20±0.03) | 19.80 |
| 2.After Moderate (Log transformation) | 61.62±32.12 (1.72±0.03) | 59.00 | 31.03±25.90* (1.34±0.03) | 29.00 |
| 3.After Strenuous (Log transformation) | 139.20±61.75 (2.09±0.03) | 141.00 | 43.18±37.43* (1.47±0.03) | 40.20 |
*p<0.05 statistically significant
Comparison of serum TNF-α levels (pg/ml) before and after (moderate and strenuous) exercise, within each group
| BCC | 1.Baseline (Before) | 2.After Moderate | 3.After Strenuous |
|---|
| Non-yoga/Control (n=109) (Log transformation) | 79.64±33.91 (1.86±0.02) | 112.78±48.95* (2.02±0.02) | 204.17±120.87* (2.24±0.02) |
| Yoga (n=109) (Log transformation) | 55.34±23.36 (1.70±0.02) | 63.07±31.29 (1.75±0.02) | 75.49±61.62 (1.81±0.02) |
*p<0.05 statistically significant
Comparison of serum IL-6 levels (pg/ml) before and after (moderate and strenuous) exercise within each group
| BCC | 1.Baseline (Before) | 2.After Moderate | 3.After Strenuous |
|---|
| Non-yoga/Control (n=109) (Log transformation) | 29.12±17.99 (1.38±0.03) | 61.62±32.12* (1.72±0.03) | 139.20±61.75* (2.09±0.03) |
| Yoga (n=109) (Log transformation) | 22.60±19.9 (1.20±0.03) | 31.03±25.90 (1.34±0.03) | 43.18±37.43 (1.47±0.03) |
*p<0.05 statistically significant
There was significant difference between the TNF-α levels of yoga and non-yoga groups before exercise and after moderate and strenuous exercise. The IL-6 levels were higher in non-yoga group compared to yoga group before exercise. The IL-6 levels were significantly higher in non-yoga group compared to yoga group after moderate exercise and strenuous exercise [Table/Fig-3,4]. No differences between the genders were observed in both the yoga group and non yoga group. With increase in level of physical activity, the rate of increase in the levels of IL-6 and TNF-α was higher in non-yoga group compared to yoga group [Table/Fig-5,6].
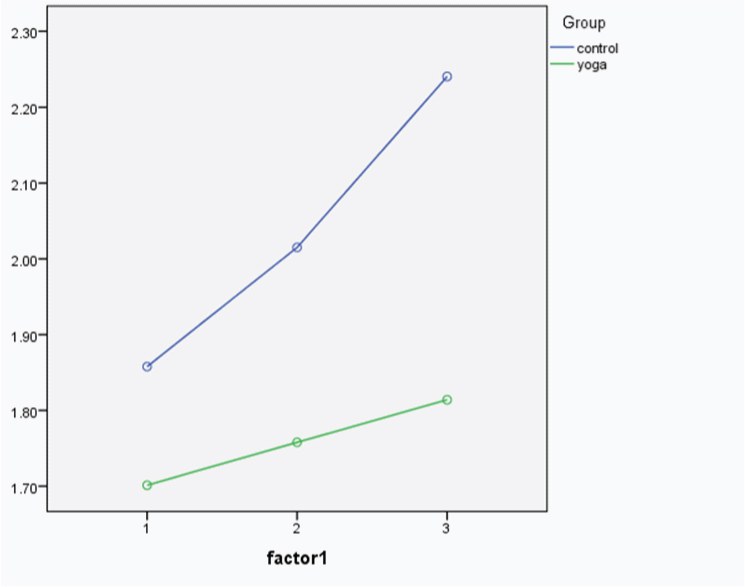
Serum TNF-α levels with different grades of exercise in yoga group and non-yoga (control) group
Factor 1 denotes the time points at which the blood samples were collected, i.e.
1 = Baseline (no exercise)
2 = After one bout of moderate exercise and
3 = After one bout of strenuous exercise
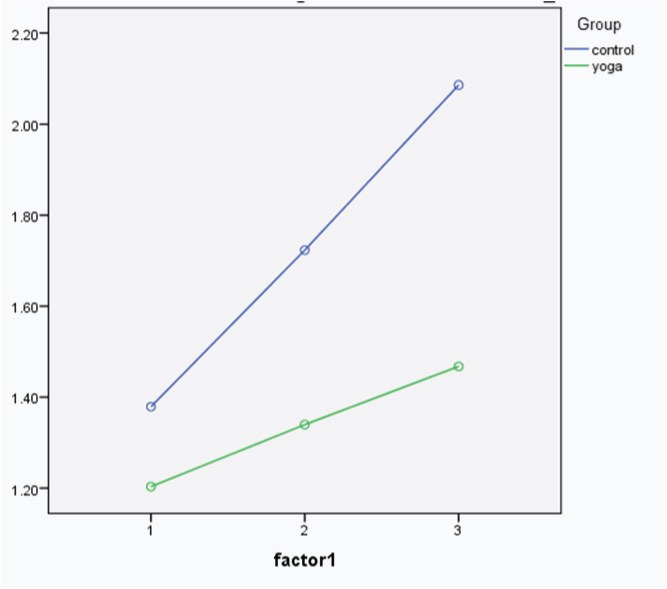
Serum IL-6 levels with different grades of exercise in yoga group and non-yoga group
Factor 1 denotes the time points at which the blood samples were collected, i.e.
1 = Baseline (no exercise)
2 = After one bout of moderate exercise and
3 = After one bout of strenuous exercise
Cholesterol, triglyceride and VLDL levels in yoga group were significantly less compared to the non-yoga group. HDL level is significantly higher in yoga group compared to non yoga group [Table/Fig-7,8]. There was a positive correlation between BMI and baseline IL-6 levels in both groups (r = 0.56). However, it was not statistically significant. There was a positive correlation between BMI and TNF-α levels before exercise and after moderate exercise and after strenuous exercise (r = 0.275, 0.241 and 0.225 respectively) which was statistically significant (p < 0.05) [Table/Fig-9].
Comparison of lipid profile between yoga and non-yoga group
| Parameter | Age (years) | BMI (kg/m2) | Resting Metabolism (Kcal) | Visceral fat (%) | Total Cholesterol (mg/dl) |
|---|
| Non-yoga/Control (n=109) | 38.65± 10.45 | 24.96 ± 2.66 | 1403.67 ± 257.42 | 8.1 ± 3.8 | 188.22 ± 17.73 |
| Yoga (n=109) | 39.46± 10.75 | 25.32 ± 2.84 | 1447.02 ± 233.17 | 8.5 ± 4.2 | 163.17 ± 14.12* |
*p<0.05 statistically significant
Comparison of lipid profile between yoga and non-yoga group
| Parameter | Triglyceride (mg/dl) | HDL (mg/dl) | VLDL (mg/dl) |
|---|
| Non-yoga (n=109) | 170.53±38.85 | 34.92±8.10 | 34.11±7.77 |
| Yoga (n=109) | 110.64±41.91* | 51.23±14.39* | 22.13±8.38* |
*p<0.05 statistically significant
Correlation between BMI and the cytokines (IL-6 and TNF- α)
| | IL-6 (Baseline) | TNF- α (Baseline) | TNF-α (Moderate Exercise) | TNF-α (Strenuous Exercise) |
|---|
| Yoga | Non-Yoga | Yoga | Non-Yoga | Yoga | Non-Yoga | Yoga | Non-Yoga |
|---|
| BMI | Pearson’s Correlation | 0.56 | 0.56 | 0.112 | 0.275 | 0.157 | 0.241 | 0.028 | 0.225 |
|---|
| Significance | 0.06 | 0.06 | 0.245 | 0.004* | 0.103 | 0.011* | 0.774 | 0.019* |
| n | 109 | 109 | 109 | 109 | 109 | 109 | 109 | 109 |
*p<0.05 statistically significant
Discussion
Cytokines are mediators of immune system. Moderate exercise stimulates the human body to produce cytokines at optimum levels to maintain a healthy immune system. IL-6 and TNF-α are pro-inflammatory cytokines. The sources of TNF- α are Helper-T cells, monocytes, macrophages, dendritic cells, natural killer cells, B cells and mast cells. The function of TNF-α is to cause tumour cytotoxicity, cachexia (weight loss), induction of cytokine secretion, induction of E-Selectin on endothelium, activation of macrophages and antiviral activity. The source of IL-6 is Helper-T cells, monocytes, macrophages and dentritic cells. It helps in differentiation of myeloid stem cells and of B cells to plasma cells, induces Acute Phase Proteins (APP) and enhances T cell proliferation. Inflammation involves influx of white cells, complement, antibody and other plasma proteins into a site of infection or injury. A complex array of mediators is involved in inflammation. Some act directly on the smooth muscle wall surrounding the arterioles to alter blood flow [16]. Others act on the venules to cause contraction of the endothelial cells with transient opening of the inter-endothelial junctions and consequent transudation of plasma [17].
The migration of the leukocytes from the blood stream is facilitated by mediators which up-regulate the expression of adherence molecules on both endothelial and white cells and others which lead the leukocytes to the inflamed site through chemotaxis. The tissue macrophages under stress secrete pro-inflammatory mediators like IL-6 and TNF-α. These cytokines stimulate the endothelial cells and maintain inflammatory process by up-regulating the expression of Selectins. TNF-α and IL-6 also act on endothelial cells, fibroblasts and epithelial cells to stimulate the secretion of chemotactic proteins for several of different cell types which are particularly potent in attracting mononuclear phagocytes to the region of inflammation [18]. Chronic inflammation is a well recognized condition that promotes Tumour development. The pro-inflammatory cytokines like IL-6 and TNF-α can be double agents in mediating either pro-Tumour or anti-Tumour effects. These cytokines exert divergent and contradictory effects in different human and animal models suggesting a high degree of context dependence in their functions. The inflammatory cytokines mediate a feedback loop of auto-immunity, anti-Tumour immunity and Tumourigenesis. The pro-inflammatory cytokines are not just markers of inflammation, but can be deleterious to health. Therefore, these cytokines are both cause and effect of inflammation [19]. Severe stress increases plasma levels of the pro-inflammatory cytokines which in turn raises plasma levels of cortisol, catecholamines, Interferon alpha and IL-1. It reduces levels of Immunoglobulin- A (IgA) and causes immune deficiency and increased susceptibility to infections. Hence, over-exercising is harmful to health [20].
Since yoga involves mind body relaxation techniques (pranayama and meditation) along with mild to moderate physical exercise (Asanas), it was hypothesized that practice of yoga may optimize the production of the pro-inflammatory cytokines. To test the effect of practice of yoga, an exercise challenge in the form of one bout of moderate exercise and one bout of strenuous exercise was given, and the serum levels of IL-6 and TNF-α after each bout of exercise were estimated. In this study, a large number (218) of normative data has been obtained for serum IL-6 and TNF- α level from Indian population. It compares with the Egyptian normal range of 172.7 ± 39.19ρg/ml for serum TNF- α and 21.15 ± 10.99 ρg/ml for serum IL-6 level [21]. The levels are higher compared to the western population [22]. For serum TNF- α, it is 35.72 ± 0.72 and 16.28 ± 8.13 for IL-6. This may possibly indicate the health status of Indian population and their susceptibility for diseases.
Resting TNF-α and IL-6 levels were lower in yoga group when compared to the non-yoga group: the difference in TNF-α levels was significant (p < 0.05). There was a significant increase in both TNF-α and IL-6 after moderate exercise and strenuous exercise in the non-yoga group when compared with yoga group [Table/Fig-1,2]. This indicates that the yoga group exhibits reduced inflammatory response as evidenced by lower levels of TNF- α and IL-6. In the non-yoga group, there is significant difference in the IL-6 as well as TNF-α levels between baseline and post exercise (both moderate and strenuous) values. However, this difference was not observed in yoga group, indicating that the non-yoga group does show significant increase in the levels of the pro-inflammatory cytokines with physical stress.
Inflammation is a robust and reliable predictor of all cause mortality. Pro-inflammatory cytokines like IL-6 and TNF-α play a role in coronary heart disease, depression, type 2 diabetes, arthritis, osteoporosis, Alzheimer’s disease and periodontal disease [23].There was significant difference between the TNF-α levels of yoga and non-yoga group before exercise and after moderate and strenuous exercise. The IL-6 levels were higher in non-yoga group compared to yoga group before exercise. The IL-6 levels were significantly higher in non-yoga group compared to yoga group after moderate exercise and strenuous exercise [Table/Fig-1,2].
With increase in level of physical activity, the rate of increase in the levels of IL-6 and TNF-α was higher in non-yoga group compared to yoga group [Table/Fig-5,6]. This indicated that regular practice of yoga protects against the rise in these cytokine levels when individuals were exposed to physical stresses/unaccustomed physical activity. In the exercise challenge intervention, the yoga group fares significantly better than non-yoga group.
Increased levels of cholesterol, triglyceride and VLDL are a predisposing factor for complications and exacerbation of metabolic disorders. Increased plasma lipids can directly cause atherosclerosis, myocardial infarction and a range of other cardiovascular disorders leading to increased morbidity. That apart, hyperlipidemia by itself can lead to inflammation. The immune cells secrete higher quantities of pro-inflammatory cytokines in hyperlipidemic individuals. This in turn leads to an alteration in lipid metabolism [24]. Hence, we looked into the plasma lipid levels in practitioners of yoga and non-practitioners to see if there was any difference in the lipid levels in the two groups.
The cholesterol, triglyceride and VLDL levels in yoga group were significantly less compared to the non-yoga group. HDL level is significantly higher in yoga group compared to non yoga group [Table/Fig-7,8]. Hence, yoga group was less likely to develop cardiometabolic disorders. Adipose tissue is a dynamic endocrine organ secreting several hormones and proteins including many inflammatory markers. Increased levels of inflammatory markers such as C Reactive protein, IL-6, Interleukin 1 receptor antagonist and TNF-α is positively associated with increased adiposity and higher levels of cholesterol, triglyceride and VLDL. Low-grade pro-inflammatory state has a role in the origin and maintenance of many chronic diseases, such as cardiovascular disease, cancer, or Alzheimer disease. Inflammatory status is strongly associated with adiposity and with mortality [25].
There was positive correlation between BMI & baseline IL-6 levels in both groups (r = 0.56). However, it was not statistically significant. There was positive correlation between BMI and TNF-α levels before exercise & after moderate exercise & after strenuous exercise (r = 0.275, 0.241 and 0.225 respectively) which was statistically significant (p < 0.05) [Table/Fig-9]. Higher levels of pro-inflammatory cytokines contribute to dyslipidemia and plaque formation in atherosclerosis. Adaptive immunity plays an essential part in this process. Whether dyslipidemia and atherosclerosis are true autoimmune diseases in origin has not been established, but they definitely appear to contain an auto-inflammatory element. Atherosclerosis is a lipid storage disease associated with inflammation. Elevated levels of the inflammatory marker high-sensitivity C-reactive protein (hs-CRP) are associated with increased risk for both CVD and diabetes.
The regression equation derived for predicting the TNF-α levels after strenuous exercise is = Constant + 0.02 X Age + 0.245 X BMI + (- 0.583 X Duration of Yoga). The equation derived from the data indicates that TNF-α levels increase with age and BMI, but decrease with increased duration of yoga practice, when exposed to strenuous exercise/stress. When an individual is exposed to strenuous physical activity/stress, the TNF- α levels do not increase if the duration of yoga is more, probably indicating positive health benefits of performing yoga/physical activity on a regular basis.
Exercise when performed daily has a good impact on health. It enhances insulin sensitivity, and brings about good glycaemic control. Regular exercise prevents obesity and reduces the fat percentage in the body. It also reduces blood pressure and decreases the risk for cardiovascular disease. When the Free Fatty Acid (FFA) levels and pro-inflammatory cytokines increase in circulation, they predispose to vascular complications. It also leads to enhanced susceptibility to pathogens. The FFA gets oxidized and this leads to increased release of Reactive Oxygen Species (ROS) from mitochondria. This leads to subsequent activation of nuclear factor (NF)-κB and increased secretion of IL-6, TNF-α and other pro-inflammatory cytokines. The Free Fatty Acids directly stimulate the WBC’s and other immune cells to release pro-inflammatory cytokines and ROS.
Limitations of the Study
Gender may influence the levels of cytokines. This study did not show any significant gender difference. With increased sample size, probably, gender difference could be seen. The BMI of the subjects in the study is above 23kg/m2. It should be less than or equal to 23kg/m2 for Asians. However it is difficult to find all the subjects in the ideal BMI range.
Conclusion
1. Regular practice of yoga reduces the resting levels of inflammatory cytokines like TNF-α and IL-6. It also decreases the levels of cholesterol, triglyceride and VLDL.
2. Increase in the duration of practice of yoga favourably affects pro-inflammatory cytokine levels when exposed to unaccustomed stress/physical activity.
3. An excess of pro-inflammatory mediators is a predisposition to pro-inflammatory disorders, exacerbation, complications of metabolic disorders and cardiovascular disease. Hence, regular practice of yoga can favourably influence the health status.
*p<0.05 statistically significant
*p<0.05 statistically significant
*p<0.05 statistically significant
*p<0.05 statistically significant
*p<0.05 statistically significant
*p<0.05 statistically significant
*p<0.05 statistically significant