Purpose
To evaluate the efficacy/safety of ‘tamsulosin and darifenacin’ (TD) vs. ‘tamsulosin and placebo’ (TP) for patients with symptomatic benign prostrate hyperplasia (BPH) with accompanying overactive bladder (OAB) symptoms.
Materials and Methods
This study included symptomatic patients of BPH with one or more of the following OAB symptoms; micturition frequency >8, nocturnal frequency > 2, urgency > 1 per 24 hour between November 2012 and February 2014. After protocol approval by ethics committee and obtaining informed consent, patients were randomly assigned to receive tamsulosin 0.4mg plus placebo (TP) (n=30) or tamsulosin 0.4 mg plus darifenacin 7.5 mg (TD) (n=30) for 8 weeks. The mean change from baseline in urinary frequency and incontinence episodes/24 hour (primary end points), and nocturnal frequency; mean change in PVR and changes in IPSS (secondary end points) were compared between groups at 0/eight week using voiding diary and ultrasonography.
Results
The mean change in frequency, incontinence, nocturnal frequency/24 hour and IPSS (International prostrate symptom score) were (−4.83 vs. −3.93, p=0.023), (−1.50 vs. 1.08, p=0.001), (−2.20 vs. −1.87, p<0.001) and (−7.90 vs. −6.27, p<0.001) in the TD/TP group respectively (significant). Apart from some minor side effects (12 vs. 9) all interventions appeared to be safe and well tolerated. The mean change in the PVR (Postvoid residual) was marginal (+10.84ml and -16.93) and the incidence of urinary retention was 13% and 3% in the TD and TP groups respectively (p=0.35).
Conclusion
Treatment with tamsulosin and darifenacin for 8 weeks is an effective and safe treatment modality in select patients of BPH with accompanying OAB symptoms.
Introduction
Lower urinary tract symptoms (LUTS) in men with benign prostatic hyperplasia (BPH) comprises of storage symptoms (frequency, urgency, nocturia, and urinary incontinence) and voiding symptoms (weak stream, intermittency, hesitancy, straining and terminal dribbling) [1,2]. The storage sub-classification category of LUTS is same as the overactive bladder syndrome (OAB), which has been previously defined by the International Continence Society (ICS) as ‘urgency, with or without urge incontinence, usually with frequency and nocturia’ [2].
Patients with LUTS due to BPH are generally prescribed alpha-adrenergic antagonists alone or in combination with 5-alpha-reductase inhibitors [3] with or without anticholinergics with invasive therapy reserved for those responding inadequately to medical therapy [4]. Antimuscarinics have been shown to be clinically effective in treating clinically unobstructed BPH with OAB symptoms [5]. The clinical effectiveness of Darifenacin (M3 receptor specific) antimuscarinic drug in the men with OAB symptoms has been demonstrated in several phase III studies [6-8]. Various studies have demonstrated that antimuscarinic agents combined with alpha blockers can improve LUTS in men with symptomatic BPH associated with overactive bladder symptoms or detrusor instability [9-11]. In this randomized study we aim to compare the clinical efficacy and safety of ‘tamsulosin and darifenacin’ versus ‘tamsulosin’ therapy for management of ‘symptomatic BPH with accompanying overactive bladder’.
Materials and Methods
From November 2012 to February 2014, 60 patients of BPH with accompanying OAB symptoms were screened in the out-patient clinic of University College of Medical Sciences (University of Delhi, India) & GTB Hospital, Delhi. After protocol approval by the Institutional Ethics Committee and after obtaining a written informed consent, all eligible patients satisfying the entry criteria, they were enrolled in to the present study. This study has been registered with the “Clinical trials registry of India, CTRI/2014/08/004811”. Entry criteria included, symptomatic patients of BPH (determined by LUTS and supplemented by IPSS/focused urological examination/investigations) associated with any one or more of the following overactive bladder symptoms like; urinary frequency/24 hour(day and night) >8 per 24 hour, nocturnal frequency > 2 per 24 hour, urgency episodes > 1 per 24 hour with or without urge incontinence. Patients of BPH with Qmax <5 ml/s, voided volume <50 ml/s, ultrasound proven PVR >150 ml/s and or progressively rising PVR, renal failure, untreated UTI and vesical stones, patients with the contraindications of α1-adrenergic receptor antagonist or antimuscarinic agent were excluded from this study.
The sample size in the present study was determined on the basis of a study by Kaplan et al., [12] (tamsulosin 0.4 mg and solifenacin 5 mg add-on study and phase II results of solifenacin alone), in which the mean change in urgency episodes/24 hour after treatment with (tamsulosin 0.4 mg), and (tamsulosin and solifenacin 5 mg) was assumed to be 1.10 and 2.20, respectively with a standard deviation of 3.3 in all groups; in order to detect a superiority of ‘tamsulosin and solifenacin’ over ‘tamsulosin’ using t-test with a two-sided significance level of 0.05 with 80% power, 190 randomized patients per group were required. Due to protocol constraints we have limited the sample size to 30 per group in future we will endeavour to study a larger group.
Patients were randomized into two groups using the table from www.randomisation.com {to reproduce this plan, use the seed 22445, randomization plan created on Mon Sep 17 2012 12:43:52 GMT+0530 (India Standard Time)} and were allocated to receive either tamsulosin 0.4 mg plus placebo (TP group) at bed time after meals for 8 weeks while the other was given tamsulosin 0.4 mg plus 7.5 mg darifenacin (TD group ) tablet at bedtime similarly for 8 weeks. Follow up visits were done at 2, 4 and 8 weeks. The mean change in the micturition frequency/24 hour and incontinence episodes/24 hour were our primary end points; while the nocturnal frequency, mean change in PVR and changes in IPSS were our secondary end points. These endpoints were compared between both the groups at baseline (0 week) and at eight week. Safety was assessed by monitoring for adverse events and side effects occurring after starting therapy.
Statistical Analysis
Data was analysed using SPSS software (version 22.0) and the changes from baseline in total IPSS scores, PVR and frequency; nocturia and incontinence episodes in patients of both groups were analysed using a paired student’s t-test. Comparison of the mean change from baseline of primary and secondary outcomes between both groups in the study was analysed using repeated measure analysis of covariance (ANCOVA) test. Fisher-exact test was used to determine the statistical significance of differences in side effects and adverse events between two groups.
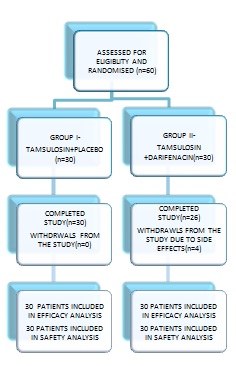
Missing data were handled using the last observation carried forward technique (LOCF). The recorded values in the voiding diary were averaged for all the recorded days, for completion a minimum of three day period data was necessary for inclusion in our analysis. In case less than three days data was available in the voiding diary we imputed the post baseline data using the last observation carry forward method. Patients who took study drugs at least once and for whom one efficacy assessment parameter had been measured at baseline and during the treatment period were included for the statistical analysis of efficacy end points (both primary and secondary). The flow of the study is depicted in [Table/Fig-1].
Results
The baseline characteristics of all the 60 patients in the two groups are shown in [Table/Fig-2a]. No significant baseline differences (age, body weight, prostate volume, IPSS, S PSA and residual urine) were noted between the two groups. The changes from baseline in the two groups after treatment with tamsulosin or the combination of tamsulosin plus darifenacin for 8 weeks are shown in [Table/Fig-2b]. In the TP group: mean urinary frequency/24 hour reduced from 12.00 to 8.07 episodes; the mean incontinence episodes/24 hour decreased from 2.88 to1.79; the mean nocturnal frequency decreased from 4.67 to 2.80 episodes and mean IPSS decreased from 19.97 to 13.70 ( all p<0.01). In the TD group: mean urinary frequency/24 hour reduced from 11.90 to 7.07 episodes; the mean incontinence episodes/24 hour decreased from 2.11 to 0.61 episodes; mean nocturnal frequency decreased from 3.87 to 1.67 episodes and mean IPSS decreased from 17.70 to 9.80 after 8 weeks of treatment(all p<0.01). The base line PVR was 28.43ml for TP group and 29.23ml for TD group. The mean change in PVR was a decrease of 16.93 ml in TP group patients and an increase of 10.84ml in TD group (not significant).
In the present study in TP group, 1 /30(3.3%) patients had a single episode of acute urinary retention that resolved on catheterization. A successful trial without catheter was observed in the patient after keeping catheter in situ for 2 weeks with continuing medication.
0.001In TD group, 4/30 (13.3%) patients had acute urinary retention in whom after discontinuation of darifenacin all patients became catheter free within two weeks. Comparison of the therapeutic effect between the two groups after 8 weeks treatment showed that the improvement of OAB symptoms and IPSS in the (TD) group was significantly greater than in the (TP) group (both p<0.05), there were some side effects but no adverse events were encountered in the current study [Table/Fig-3a].
Discussion
The primary objectives of the medical treatment for LUTS/BPH are to produce rapid, sustained, and safe improvements in the LUTS associated with benign prostatic hyperplasia that affect the quality of life in the majority of men over the age of 50 years. The incidence of OAB associated with BPH is around 40–75%, and because the symptoms of the two are similar and often overlapping, it may be difficult to distinguish them clinically [13]. In the past several large well-designed, randomized, placebo-controlled trials have provided evidence for efficacy/safety of tamsulosin for treating LUTS associated with BPH [14-16]. According to one study [11] only a third of men undergoing treatment for BPH and OAB were found to have improvement with alpha blocker monotherapy but 75% of patients were found to have significant improvement in OAB symptoms on combining an antimuscarinic agent with alpha blocker [11].
Antimuscarinic agents have been shown to be clinically effective in treating clinically unobstructed men with OAB symptoms [5]. However; antimuscarinic agents are prescribed with caution for this disease because of the worry that they might increase voiding problems and the risk of urinary retention. We decided to evaluate the efficacy/safety of combination therapy with tamsulosin and darifenacin in BPH patients with accompanying OAB symptoms since recent studies on darifenacin have also indicated some promising results in relieving OAB symptoms accompanying BPH [6-8]. In our study, a total of 60 patients were presented with BPH with accompanying OAB symptoms and were found to satisfy the entry criteria for our study.
Our results indicated that the patients in this study had benefited from combination therapy with tamsulosin and darifenacin, which proved to both efficacious and relatively safe. After eight weeks treatment, all patients in the two groups had statistically significant improvements in their OAB symptoms (frequency, nocturia and incontinence) and IPSS. The reductions in the OAB symptoms/IPSS was significantly greater in the darifenacin plus tamsulosin combination group [Table/Fig-2b]. Therefore, use of only α1-adrenergic receptor antagonist was not as effective as the combination treatment for patients with symptomatic BPH with accompanying OAB symptoms. In the combination therapy, IPSS was significantly reduced by 7.90 versus a decrease of 6.27 with tamsulosin mono therapy group; this may be related to an increased bladder capacity due to the treatment with an anticholinergic agent. These results seem to indicate that combination therapy produced a greater improvement in IPSS versus tamsulosin therapy alone in our select patients.
In the present study the base line PVR was 28.43ml (mean decrease of 16.93 ml) and 29.23ml (mean increase of 10.84ml) for TP/TD group respectively. Rise in PVR in BPH patients may be multi factorial; darifenacin inhibits muscarinic receptors in the bladder that may result in decreased urinary bladder contractions and decreased detrusor pressure; due to detrusor under activity or myogenic failure or as a result of ageing. Although there was a marginal increase in the PVR in TD group in the present study, this absolute change was small, not clinically meaningful and not significant as the benefits derived in terms of improvements of OAB symptoms far outweighed this marginal increase in PVR. Side effects in (TD) group (12/30) were higher than that in (TP) group (9/30) [Table/Fig-3a] which included dry mouth, constipation and dry eye all of which improved spontaneously. Acute urinary retention was recorded in 1/30(3.3%) patient in TP group vs 4/30(13.3%) patients in TD group (not significant between the two groups).
In the present study in TP group, 1/30(3.3%) patients had a single episode of acute urinary retention that resolved on catheterization. A successful trial without catheter was observed in the patient after keeping catheter in situ for two weeks with continuing medication. In TD group, 4/30(13.3%) patients had acute urinary retention and were discontinued, but all recovered because of catheterization. Kaplan et al., [17], found that in BPH patients many factors can contribute to the development of urinary retention including bladder outlet obstruction, detrusor under activity and neurogenic bladder and these authors suggested that age, previous retention episodes, LUTS, chronic inflammation, serum prostate specific antigen levels, prostate size, and urodynamic variables appear to be predictors of acute urinary retention (AUR) [17]. In the TD group acute urinary retention might have been precipitated by concomitant consumption of alcohol in one patient with LUTS in the study, although this was inconclusive. This patient had a pre therapy PVR of 100 ml, prostate volume of 27 ml, and S.PSA value of 2.8 ng/ml, while in the remaining three patients the pre therapy PVR was 100/108/ 60 ml; prostate volume was 50.0/54.0/56.0 ml and PSA level was 2.0/2.2/3.80 ng/ml. We assume that in these patients detrusor muscle fibers might be over distended/less responsive to neural mechanisms, therefore these patients may be less responsive to drugs and may have develop acute urinary retention. Although there was higher incidence (13% versus 3%) of AUR episodes in the present study in patients of TP group versus TD group, it was not significant. The absence of statistical significance for the difference between the 2 groups may be due the small number of cases in the study (not enough power), and study with adequate number of cases may show a statistically significant difference. Further trials are warranted to establish the long-term safety of combined therapy with darifenacin and tamsulosin for patients of BPH with LUTS associated with OAB symptoms. We found on analysis of previous studies done on combination of alpha blocker plus antimuscarinic therapy vs. alpha blocker mono therapy in BPH/LUTS patients that the incidence of overall urinary retention was comparable to the present study as depicted in [Table/Fig-3b] [12,18-21].
Depicting the flow of the present study
Showing the comparison of demographic and initial baseline parameters
| INITIAL PARAMETERS | GROUP (I) (TP) MEAN±SD, N=30 | GROUP (II) (TD) MEAN±SD, N=30 | p value (NS) |
|---|
| AGE(Yrs) | 63.00±9.18 | 58.73±11.34 | 0.114 |
| BMI(Kg/m2) | 22.98±2.24 | 22.25±1.83 | 0.153 |
| PROSTATE SIZE (USG) (ml) | 30.70±15.93 | 32.37±15.35 | 0.681 |
| S. PSA (ng/ml) | 1.89±1.32 | 1.70 ± 0.99 | 0.536 |
| MICTURITION FREQUENCY /24 hrs | 12.00±4.42 | 11.90±3.35 | 0.922 |
| NOCTURNAL FREQUENCY /24 hrs | 4.67±2.48 | 3.87±1.35 | 0.128 |
| INCONTINENCE EPISODES/24 hrs# | 2.88±1.56 | 2.11±1.07 | 0.084 |
| PVR(ml) | 28.43±36.12 | 29.23±32.97 | 0.929 |
| IPSS* | 19.97±4.94 | 17.70±4.51 | 0.069 |
*IPSS: International prostate symptom score, PVR: Post void residue (volume in mls), NS: Not significant
# Subjects with incontinence episodes (n=24 for tamsulosin plus placebo; n=18 for tamsulosin plus darifenacin)
Showing a comparison of changes from baseline to end of treatment outcomes
| PARAMETER | TP(Group-I) Mean Change From Baseline (95%CI), (N=30) | TD (Group-II) Mean Change From Baseline (95% CI), (N=30) | Treatment Difference Mean Change (95% CI) | p-value# |
|---|
| Micturitions / 24 h | -3.93 (-2.01,-5.86) | -4.83(-3.94,-5.73) | 0.94 (0.13,1.76) | 0.023 |
| Nocturia Episodes/24 h | -1.87 (-1.34,-2.39) | -2.20 (-1.92,-2.48) | 0.69 (0.33,1.05) | <0.001 |
| IPSS Total Score | -6.27 (-5.40,-7.13) | -7.90 (-6.92,-8.88) | 2.19 (1.01,3.36) | <0.001 |
| Incontinence Episodes/24 h^ | -1.09 (-0.81,-1.36) | -1.50 (-1.15,-1.85) | 0.63 (0.27,1.00) | <0.001 |
| PVR | -16.93 (-9.30,-24.56) | +10.84 (+22.2,-0.54) | 27.84 (14.41,41.26) | <0.001 |
# p-values for comparisons between TP groups and TD group are based on analysis of covariance test using the treatment group as a factor and baseline as a covariate. ^ Only patients who had incontinence at baseline were included (24 vs 18)
Showing the comparison of side effects in TP group & TD group
| SIDE EFFECT | TP GROUP N=30 | TD GROUP N=30 | p- value, Fisher Exact Test (Non Significant) |
|---|
| Orthostatic hypotension | 2 | 1 | 1.00 |
| Headache | 2 | 1 | 1.00 |
| Retrograde ejaculation | 2 | 2 | 1.00 |
| Acute urinary retention | 1 | 4 | 0.35 |
| Constipation | 1 | 2 | 1.00 |
| Dry mouth | 1 | 2 | 1.00 |
Showing comparison of incidence of overall acute urinary retention episodes of present study with other similar studies
| Author | Antimuscarinic Used | Antimuscarinic + Alpha Blocker | Alpha Blocker + Monotherapy |
|---|
| Kaplan et al., [18] | Tolterodine | 2/225 | 0/215 |
| Chapple et al., [19] | Tolterodine | 3/329 | 2/323 |
| Kaplan et al., [12] | Solifenacin | 7/202 | 0/195 |
| Yamaguchi et al., [20] | Solifenacin | 4/414 | 0/209 |
| Lee et al., [21] | Tolterodine | 2/83 | 1/84 |
| Present Study | Darifenacin | 4/30 | 1/30 |
Limitations
Due to our protocol logistics there were certain limitations in this study. This study was of short eight week duration, it was low powered due to a small sample size, and it lacked a true non-treatment group since the basic intent to treat principle was followed. The sample size was calculated on the basis of urgency as an outcome which assessed indirectly via the IPSS. The diagnosis of associated OAB was based on patient symptomatology (voiding diary) with urodynamics being omitted due to additional costs, risk of UTI and due to our protocol limitations
Conclusion
The conclusions of the present study should be seen in the light of these limitations. Never the less despite these limitations this study appears to demonstrate that therapy with tamsulosin plus darifenacin may be an effective and safe treatment modality in select patients of BPH with accompanying OAB symptoms.
*IPSS: International prostate symptom score, PVR: Post void residue (volume in mls), NS: Not significant# Subjects with incontinence episodes (n=24 for tamsulosin plus placebo; n=18 for tamsulosin plus darifenacin)
# p-values for comparisons between TP groups and TD group are based on analysis of covariance test using the treatment group as a factor and baseline as a covariate. ^ Only patients who had incontinence at baseline were included (24 vs 18)
[1]. JM Fitzpatrick, The natural history of benign prostatic hyperplasiaBJU Int 2006 97(Suppl 2):3-6. [Google Scholar]
[2]. P Abrams, L Cardozo, M Fall, The standardization of terminology of lower urinary tract function: Report from the Standardization Subcommittee of the International Continence SocietyNeurourol Urodyn 2002 21(2):167-78. [Google Scholar]
[3]. JD McConnell, CG Roehrborn, OM Bautista, The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasiaN Engl J Med 2003 349(25):2387-98. [Google Scholar]
[4]. H Lepor, FC Lowe, Evaluation and nonsurgical management of benign prostatic hyperplasia. In: Campbell – Walsh Urology. Wein AJ (Ed) 2002 8th EditionSaunders Elsevier:1337-78. [Google Scholar]
[5]. CG Roehrborn, P Abrams, ES Rovner, Efficacy and tolerability of tolterodine extended-release in men with overactive bladder and urgency urinary incontinenceBJU Int 2006 97(5):1003-06. [Google Scholar]
[6]. MB Chancellor, F Kianifard, E Beamer, A comparison of the efficacy of darifenacin alone vs. darifenacin plus a Behavioral Modification Programme upon the symptoms of overactive bladderInt J Clin Pract 2008 62(4):606-13. [Google Scholar]
[7]. C Chapple, W Steers, P Norton, A pooled analysis of three phase III studies to investigate the efficacy, tolerability and safety of darifenacin, a muscarinic M3 selective receptor antagonist in the treatment of overactive bladder BJU Int 2005 95(7):993-1001. [Google Scholar]
[8]. N Zinner, J Tuttle, L Marks, Efficacy and tolerability of darifenacin, a muscarinic M3 selective receptor antagonist (M3 SRA), compared with oxybutynin in the treatment of patients with overactive bladderWorld J Urol 2005 23:248-52. [Google Scholar]
[9]. A Athanasopoulos, K Gyftopoulos, K Giannitsas, Combination treatment with an alpha-blocker plus an anticholinergic for bladder outlet obstruction: a prospective, randomized controlled studyJ Urol 2003 169(7):2253-56. [Google Scholar]
[10]. KS Lee, MS Choo, DY Kim, JC Kim, HJ Kim, KS Min, Combination treatment with propiverine hydrochloride plus doxazosin controlled release gastrointestinal therapeutic system formulation for overactive bladder and coexisting benign prostatic obstruction: a prospective. randomized, controlled multicenter studyJ Urol 2005 174(4 Pt 1):1334-38. [Google Scholar]
[11]. JY Lee, HW Kim, SJ Lee, Comparison of doxazosin with or without tolterodine in men with symptomatic bladder outlet obstruction and an overactive bladderBJU Int 2004 94(7):817-20. [Google Scholar]
[12]. SA Kaplan, K McCammon, R Fincher, Safety and tolerability of solifenacin addon therapy to alpha-blocker treated men with residual urgency and frequencyJ Urol 2009 182:2825-30. [Google Scholar]
[13]. JG Blaivas, BK Marks, JP Weiss, Differential diagnosis of overactive bladder in menJ Urol 2009 182:2814-17. [Google Scholar]
[14]. P Abrams, CC Schulman, S Vaage, Tamsulosin, a selective α1A-adrenoceptor antagonist: a randomized, controlled trial in patients with benign prostatic obstruction (symptomatic BPH). The European Tamsulosin Study GroupBr J Urol 1995 76:325-36. [Google Scholar]
[15]. CC Schulman, J Cortvriend, U Jonas, Tamsulosin, the First Prostate-Selective α1A-Adrenoceptor Antagonists. European Tamsulosin Study GroupEur Urol 1996 29:145-54. [Google Scholar]
[16]. CC Schulman, TMTW Lock, JM Buzelin, Long-term use of Tamsulosin to treat lower urinary tract symptoms/benign prostatic hyperplasiaEuropean Tamsulosin Study Group: J Urol 2001 166:1358-63. [Google Scholar]
[17]. SA Kaplan, AJ Wein, DR Staskin, Urinary retention and post-void residual urine in men: separating truth from traditionJ Urol 2008 180(1):47-54. [Google Scholar]
[18]. SA Kaplan, CG Roehrborn, ES Rovner, Tolderodine and tamsulosin for treatment of men with lower urinary tract symptoms and overactive bladder: a randomized controlled trialJAMA 2006 296:2319-28. [Google Scholar]
[19]. C Chapple, S Herschorn, P Abrams, Tolterodine treatment improves storage symptoms suggestive of overactive bladder in men treated with alpha-blockersEur Urol 2009 56:534-43. [Google Scholar]
[20]. O Yamaguchi, H Kakizaki, Y Homma, Solifenacin as addon therapy for overactive bladder symptoms in men treated for lower urinary tract symptoms randomized controlled studyUrology 2011 78(1):126-33. [Google Scholar]
[21]. SH Lee, BH Chung, SJ Kim, Initial combined treatment with anticholinergics and α-blockers for men with lower urinary tract symptoms related to BPH and overactive bladder: a prospective, randomized, multi-center, double-blind, placebo-controlled studyProstate Cancer Prostatic Dis 2011 14(4):320-25. [Google Scholar]