Two Pelvic Digits on Same Side: Double Trouble?
Kavin Khatri1, Darsh Goyal2, Rajesh Paul3, H.S. Sandhu4
1Assistant Professor, Department of Orthopaedics, GGS Medical College and Hospital, BFUHS, Faridkot, India.
2Senior Resident, Department of Orthopaedics, Sports Injury Centre, Safdarjung Hospital, New Delhi, India.
3Professor and Head, Department of Orthopaedics, GGS Medical College and Hospital, BFUHS, Faridkot, India.
4Professor, Department of Orthopaedics, GGS Medical College and Hospital, BFUHS, Faridkot, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kavin Khatri, Hno 214, Bhan Singh Colony, Faridkot, Punjab-151203, India.
E-mail: kavinkhatri84@gmail.com
Pelvic digit is a rare congenital anomaly of pelvis usually discovered incidentally on plain radiography. It usually develops in the soft tissue adjacent to the normal skeletal tissue. Its importance lays in its differentiation from heterotopic ossification, osteochondroma, Fong’s disease and traumatic avulsion injuries of pelvis to avoid any unnecessary investigations and interventions. Here, we report a 32-year-old male presenting with complain of pain in right hip, was subjected to radiographic examination and two pelvic digits were noticed arising from the iliac bone in addition to features of osteoarthritis of hip joint. The symptomatology was attributed to osteoarthritis of hip after thorough physical examination and imaging investigations.
Computed tomography, Eleventh finger, Pelvic rib
Case Report
A 32-year-old male, domestic helpers by occupation, presented to the outpatient department of Guru Gobind Singh Medical College, Faridkot, India with complain of pain in his right hip since one year. The pain was insidious in onset, gradually progressive, non radiating, localized to right hip, increased on walking, squatting and relieved with rest and analgesics. Patient was not able to sit cross legged due to pain in both hips. There was no history of trauma, alcohol abuse, drug abuse including intake of steroid for long duration or fever. Core decompression of left femoral head was done at another hospital three years ago. Though there was decrease in pain but he continued to experience mild intermittent pain on the left side.
On physical examination there was surgical scar mark measuring 5cms present over the lateral aspect of left hip which healed with primary intention. There was no scar or sinus present on the right side of the hip or thigh. There was no palpable mass over either hip region. Restriction of movements at right hip with flexion limited to 60o, abduction of 15o, external rotation of 25o and internal rotation of 10o. Patient had Trendelenburg gait. However, there was no restriction of movements at the left hip. Muscular wasting of three centimeters was noticed of the right thigh. Rest of the clinical examination was unremarkable. The blood investigations including serum calcium, phosphate and alkaline phosphatase were within normal limits.
Pain radiographs revealed a bony protuberance arising from the lateral aspect of iliac wing at the level of right anterior inferior iliac spine, measuring several centimetres. There were subchondral cysts on the acetabular side and in the femoral head along with decrease in joint space. On left side, tract in the femoral and neck created by core decompression could be appreciated [Table/Fig-1]. Subsequently computed tomography [Table/Fig-2,3] was carried which showed two bony lesions one measuring 41 mm X 25 mm [Table/Fig-4] and another 43mm X 10 mm [Table/Fig-5] with corticomedullary differentiation and pseudoarticulation at the iliac wing along with features of osteoarthritis at the right hip. This helped differentiating it from osteochondroma and myositis ossificans.
The symptoms of the patient were attributed to the osteoarthritic changes at right hip joint and was advised hip arthroplasty, however the patient was not ready for the same and continued with hip strengthening, range of motion along with intermittent use of pain killers.
Discussion
Pelvic digit was first reported by Sullivan and Cornwell in 1974 [1]. They thought it to originating from first coccygeal vertebrae and histopathologically found it to be similar with rib. Later on other authors hypothesized that it could have arisen from displacement of rib or ossification centre of anteriosuperior iliac spine. Currently it is believed to be a failure of mesenchymal apoptosis for the anterior and lateral costal process. The segmentation of these cartilaginous centers gives the appearance of phalanges of a finger hence described as “the eleventh finger” [2]. It can be found at all levels of pelvic bone. It can arise from ilium, sacrum, coocyx, abdominal wall and symphysis pubis. Sometimes it may present on both sides of the hip joint.
Some authors had described it as pelvic digit or finger due to pseudoarticulations [3] in body of lesion resembling phalanges of finger however there was single pseudoarticulation in our case at its pelvic origin. Differential diagnosis of pelvic digit includes heterotopic ossification, traumatic avulsion injury of pelvis, Fong’s disease [4], myositis ossificans and osteochondroma. It can be differentiated from heterotopic ossification and myositis ossificans by corticated appearance of pelvic digit on radiological examination and absence of history of trauma. Osteochondroma has cortical continuity at its origin while pelvic digit has pseudoarticulation at its origin. Fong’s disease is a hereditary condition characterized by absent or hypoplastic knee caps and iliac horns. The iliac horns are bilateral in majority of the cases and associated with dysplatic nails. Computed tomography is an investigation which can help in differentiating pelvic digit from mimics.
Avascular necrosis of hip is leading cause of osteoarthritis in adults. It can lead to pain in hip and limitation of movements. While reviewing the literature we did not come across as any other case with co-existent avascular necrosis and pelvic digit. Rijal et al., had reported a case of asymptomatic pelvic digit associated with rheumatoid arthritis [5]. Their patient presented with pain and marked restriction of movements at the right hip joint. He was put on disease modifying anti rheumatoid drugs and the symptoms resolved within one month. The patient was saved from an early operative intervention. Maegele et al., had advised reported excision of only symptomatic pelvic digits [6]. Suarez et al., had also reported marked improvement in range of movements and relief in pain after excision of symptomatic pelvic digit [7]. While planning for operative intervention we should first determine whether the symptoms are due to pelvic digit or any other associated joint pathology. The surgical removal of asymptomatic digits can lead to morbidity arising due to extensive surgery.
Radiograph showing bony protuberance on the right side with features of osteoarthritis and tract of previous core decompression on left side

Coronal section of computed tomogram (CT) of pelvis confirming the findings seen on radiograph showing bony outgrowth from supra-acetabular region with acetabular cyst and decreased joint space on the right side. The tract in the left femoral head and neck is seen from previous core decompression

3D reconstructed image of CT scan showing two bony outgrowth from right supra-acetabular region

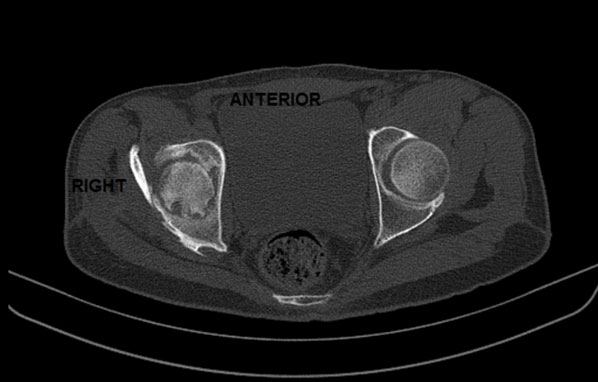
Transverse section of CT scan showing bony outgrowth with corticomedullary differentiation and pseudoarticulation on right supra-acetabular area
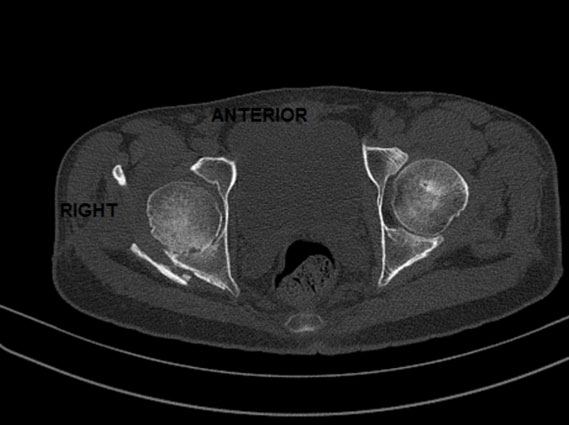
Transverse section of CT scan showing second bony outgrowth on right side
Conclusion
Pelvic digit is a developmental anomaly which may be incidentally discovered on a routine radiograph or occasionally present with symptoms. The symptomatology should be adequately correlated with it and differentiated from other conditions in order to avoid any unnecessary operative intervention.
[1]. D Sullivan, WS Cornwell, Pelvic rib. Report of a case.Radiology 1974 110(2):355-57. [Google Scholar]
[2]. Breuseghem V, The pelvic digit: a harmless “eleventh” fingerBr J Radiol 2006 79(945):e106-07. [Google Scholar]
[3]. BS McGlone, S Hamilton, MJ FitzGerald, Pelvic digit: an uncommon developmental anomalyEur Radiol 2000 10(1):89-91. [Google Scholar]
[4]. CJ Das, J Debnath, Nail patella syndromeIndian J Pediatr 2009 76(10):1077 [Google Scholar]
[5]. L Rijal, P Nepal, Multiple Pelvic digits: a rare congenital anomalyEur J Orthop Surg Traumatol 2010 20(5):411-13. [Google Scholar]
[6]. M Maegele, Pelvic digit as a rare cause of chronic hip pain and functional impairment: a case report and review of the literatureJ Med Case Reports 2009 3:139 [Google Scholar]
[7]. J Moreta-Suárez, O Sáez de Ugarte-Sobrón, A Sánchez-Sobrino, J Martínez-De Los Mozos, The Pelvic Digit: a Rare Congenital Anomaly as a cause of Hip PainJournal of Orthopaedic Case Reports 2012 2(4):19-22. [Google Scholar]