Multidisciplinary Approach in Management of a Large Cystic Lesion in Anterior Maxilla - A Case Report
Abhinav Diwan1, Moushmi Chalakkarayil Bhagavaldas2, Vivek Bagga3, Akshay Shetty4
1 Professor, Department of Conservative Dentistry & Endodontics, Sri Rajiv Gandhi Dental College & Hospital, Bangalore, India.
2 Post Graduate Student, Department of Conservative Dentistry & Endodontics, Sri Rajiv Gandhi Dental College & Hospital, Bangalore, India.
3 Post Graduate Student Department of Oral & Maxillofacial Surgery, Sri Rajiv Gandhi Dental College & Hospital, Bangalore, India.
4 Professor, Department of Oral & Maxillofacial Surgery, Sri Rajiv Gandhi Dental College & Hospital, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abhinav Diwan, Professor, Department of Conservative Dentistry & Endodontics, Sri Rajiv Gandhi Dental College & Hospital, Bangalore-560032, India. E-mail : drabhinavdiwan@yahoo.co.in
Management of large cystic lesion requires a multidisciplinary approach. In this case report a large radicular cyst is managed by conventional root canal treatment with triple antibiotic paste followed by surgical enucleation. In this case, patient presented with a 4 cm symptomatic swelling of the palate adjacent to teeth 21, 22 and 23. The swelling was soft on palpation and the overlying mucosa was of normal color. Radiographically, a well-defined unilocular radiolucency with corticated margins was seen. A full-thickness flap was reflected and revealed a large cyst-like lesion that had perforated the lingual cortical plate. The lesion was enucleated and submitted for microscopic examination. The biopsy report confirmed the diagnosis as radicular cyst.The patient was recalled after 6 months, and no symptoms or signs were noted. Radiograph showed the healing lesion.
Enucleation, Radicular cyst, Root canal treatment, Triple antibiotic paste
Case Report
A 32-year-old male was referred to the Department of Conservative Dentistry and Endodontics with the chief complaint of pain and difficulty in having food because of swelling behind front teeth for past one month. Medical history was noncontributory. According to the patient's clinical records, he reported a history of pain in the upper left side three months back. He consulted a general dentist 30 days back; where root canal treatment is initiated with respect to two upper left front teeth. There was an increase in swelling after the initiation of the treatment. Pain was present which was of sudden onset, with mild to moderate intensity and was intermittent in nature. Because of the swelling he found it difficult to masticate and speak. He also gives a history of trauma three years back. Clinically there was Ellis class II fracture in relation to 21 and 22.
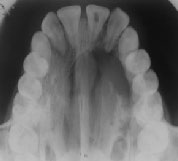
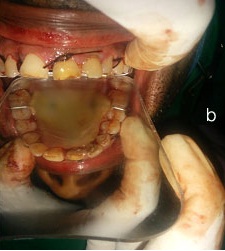
On extraoral examination, patient’s lip was incompetent. Intraoral examination revealed a soft non-tender swelling of the palate in the concerning region covered with normal mucosa [Table/Fig-1a]. Access openings of tooth 21 and 22 were found to be left open, which were tender to percussion and with probing tooth no 22 exhibited grade 1 mobility. The electric pulp test, cold test and heat test were negative for teeth 21, 22 and 23. An occlusal radiograph showed a well-circumscribed radiolucent lesion eroding the hard palate, involving 21, 22, 23, 24 and 25 and slightly crossing the midline [Table/Fig-1b].The lesion was approximately 3 x 4.5 cm in maximum diameter. After evaluating all the data, root canal treatment of 21, 22 and 23 was planned, tooth no 24 & 25 showed positive response to electric pulp testing, cold test & heat test, hence no treatment was initiated for tooth no 24& 25. After getting informed consent from the patient, on the same day, the working length determination and cleaning and shaping of the root canal was done for 21 and 22 under rubber dam isolation with wedgets. The canals were instrumented with size 15–60 K-files using a step-back technique. A haemorrhagic, purulent exudate was found from the canal of tooth no 22. During the instrumentation, the canal was irrigated copiously with 3% sodium hypochlorite solution using a 27-gauge endodontic needle after each instrument. Drainage was performed until the discharge through the canal ceased. The canals were dried with sterile paper points and then dressed with triple antibiotic paste consisting of ciprofloxacin, metronidazole, and minocycline. A sterile cotton pellet was inserted into the access cavity before sealing it with Cavit. The dressing was placed for 21 days. Root canal treatment for 23 was completed within 7 days as the tooth was asymptomatic & canal was dry. The obturation for 21 and 22 was done with gutta-percha and AH plus sealer on the same day of surgery and referred to the department of oral and maxillofacial surgery for the surgical enucleation of the lesion.
Intraoral photograph showing extent of the lesion

An occlusal radiograph showing a well-circumscribed radiolucent lesion eroding the hard palate
Under a tentative diagnosis of radicular cyst, surgical treatment was planned. Under local anaesthesia, palatal flap was reflected and entire cystic lesion was exposed [Table/Fig-2]. The enucleation was performed without any complications. Palatal stent was given to the patient postoperatively [Table/Fig-3a&b].
Shows reflection of Mucoperiosteal flap & enucleation of cyst

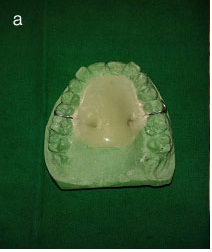
Palatal stent placed postoperatively
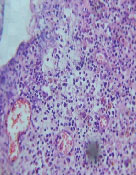
Cystic lining was enucleated & sent for histopathological examination. Histopathological investigation showed cystic lining composed of 3-5 cell layer thick ciliated stratified columnar epithelium with lumen filled with mucoid like eosinophilic material. Fragments of non keratinized stratified squamous epithelium showing arcading pattern in focal areas are seen [Table/Fig-4a&b]. Fibrovascular capsule shows mucous acinar glands, along with focal areas of dense chronic inflammatory infiltrate of lymphocytes and plasma cells. Few plasmacytoid cells are binucleated. Increased vascularity with numerous dilated endothelial lined blood capillaries and thickened vessels filled with RBCs are evident along with areas of haemorrhage.Thus biopsy report confirmed the diagonosis as radicular cyst [Table/Fig-5].
H & E section shows areas of ciliated & arcading pattern of non keratinized epithelium with inflammatory cells (10x magnification, 40x magnification)
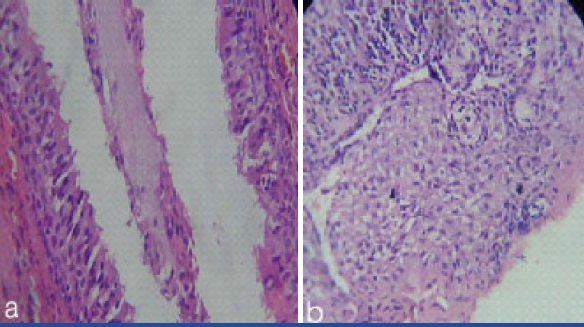
High power shows arcading pattern, mixed inflammatory infiltrate with areas of haemorrhage (40x magnification)
After 6 months postsurgery [Table/Fig-6a&b], the overlying soft tissue was healthy in appearance and the radiolucency had reduced drastically showing the signs of healing.
Shows occlusal radiograph & clinical photograph of healing lesion after 6 months

Discussion
Radicular cysts are inflammatory jaw cysts and occur at the apices of teeth associated with infected and necrotic pulps [1]. They are most common among the odontogenic cysts. Many cases can be prevented because they develop as a consequence of advanced carious lesions [2].
Root canal infections are polymicrobial and because of the complexity of the root canal infection, it is unlikely that any single antibiotic could result in effective sterilization of the canal. The most commonly used medicament is a combination of three antibiotics, referred to as a triple antibiotic paste (TAP) which contains metronidazole, ciprofloxacin, and minocycline. Metronidazole is a nitroimidazole compound. It is selectively toxic to anaerobic microbes and also exhibits broad spectrum antimicrobial activity against protozoa and anaerobic bacteria. Tetracycline, which includes doxycycline and minocycline are primarily bacteriostatic and they exhibit broad spectrum of activity against gram positive and gram negative microorganisms. It also increases the level of interleukin-10, an anti-inflammatory cytokine. Ciprofloxacin is a synthetic floroquinolone with rapid bactericidal action. It exhibits very potent activity against gram negative bacteria but very limited activity against gram positive bacteria. Most of the anaerobic bacteria are resistant to ciprofloxacin. Hence, it is often combined with metronidazole in treating mixed infections [3].
Most radicular cysts develop slowly and rarely become large enough to extensively erode adjacent bony structures as in our case. Surgical treatments for odontogenic cysts include total enucleation of small lesions, marsupialization for decompression of larger cysts, or a combination of these techniques. When surgical intervention becomes necessary, the clinician must decide whether to enucleate the lesion completely or to try “decompression”.
Enucleation is the preferred treatment for odontogenic cysts [4,5]; however, when the lesion is large, marsupialization can be performed owing to the risk of fracture or harming any important organ or tissue during the removal of the lesion by enucleation [6]. If marsupialisation with decompression is attempted first, the size of the lesion will be reduced, which will make it less difficult to remove, with less risk of damage to the neighbouring teeth and vital structures. Long-term follow-up is necessary because the re-ossification of the cyst generally takes two years [7].
Conclusion
Multidisciplinary approach involving Endodontist & Maxillofacial surgeon holds the key to management of large Radicular cysts. Long term follows up and radiographs taken at frequent intervals will help in eventual success of the treatment outcome.
[1]. Nair PN, New perspectives on radicular cysts: do they heal?Int Endod J 1998 31:155-60. [Google Scholar]
[2]. Meningaud JP, Oprean N, Pitak-Arnnop P, Odontogenic cysts: a clinical study of 695 casesJ Oral Sci 2006 48:59-62. [Google Scholar]
[3]. Ahmed N, Neelakantan P, Antiseptics and Antibiotics Used in Regenerative EndodonticsInternational Journal of Pharmaceutical and Clinical Research 2013 5(4):141-44. [Google Scholar]
[4]. Freedland JB, Conservative reduction of large periapical lesionsOral Surg Oral Med Oral Pathol 1970 29:455-64. [Google Scholar]
[5]. Neaverth EJ, Burg HA, Decompression of large periapical cystic lesionsJ Endod 1982 8:175-82. [Google Scholar]
[6]. Muglali M, Sumer AP, Squamous cell carcinoma arising in a residual cyst: a case reportJ Contemp Dent Pract 2008 9:115-21. [Google Scholar]
[7]. Martin SA, Conventional endodontic therapy of upper central incisor combined with cyst decompression: a case reportJ Endod 2007 33:753-57.Epub; 2007, March 21 [Google Scholar]