Digital radiography has recently become an important diagnostic tool in endodontics [3]. It is utilized to assess canal morphology and length during root canal therapy because it has several advantages [4]. Lower patient dose, ease of archiving and transmission, and enhancement of images are a number of these advantages [5–7]. In addition, many software programs with different enhancement tools have become commercially available since the introduction of digital radiography to dentistry [8,9]. Each new software program is used in an attempt to resolve the deficiencies of previous one and to be more popular and user friendly. Enhancement tools that are commonly used in these software programs are contrast-brightness adjustment, magnification, noise reduction, edge enhancement, and contrast inversion [6,10–13].
Inversion of contrast changes the positive radiographic image into a negative one. For example, this enhancement changes the radiopaque white appearance of the bone into the black one and the radiolucent black appearance of the air into the white one. This altered image may be useful in some clinical situations due to its effect on observer perception. There are numerous studies about the effect of contrast inversion on radiographic diagnostic and measurement accuracy of dental problems such as caries, fractures, interproximal bone loss, and periapical lesions [14–18]. For example, Eickholz et al., [15] and Scaf et al., [17] evaluated the effect of the contrast inversion enhancement on the accuracy of linear measurements of the interproximal bone loss. The results of the first study showed that the enhanced image had reduced measurement accuracy [15]. However, the second study showed that the enhanced and original images had same measurement accuracy [17]. However, there is only one paper evaluating the effect of this enhancement on the accuracy of endodontic file length measurement in digital periapical radiograph [3]. In this paper an old version of the digital software program was used and the results showed no significant difference in the measurement accuracy of the original and enhanced images. Therefore, the present study was designed to assess the accuracy of endodontic file length measurement in inverted contrast digital periapical images by using the latest version of the Scanora software program (Soredex Corporation, Helsinki, Finland)”.
Materials and Methods
Following approval by the Ethics Committee of Isfahan University of Medial Sciences (no. 391284), 40 single-rooted single-canal mature permanent human teeth were included in this experimental ex-vivo study. The teeth had intact crowns and roots, measuring 20-24 mm in length. The teeth had been extracted for periodontal or prosthetic reasons. The samples were cleaned and disinfected by scaling and soaking in 0.5% sodium hypochlorite for 12 h and stored in distilled water at 4°C during the study. Teeth with any abnormalities or pathologies such as internal/external root resorption, root canal obliteration/calcification, severe curvature (curvature greater than 15° according to the Schneider method [19]), cracks, and fractures were excluded.
In the present study, the method of our previous study [20] was used. Anatomic access cavities were prepared with #008 and #010 fissure burs and an Endo-Z bur (Dentsply Maillefer, Ballaigues, Switzerland) in a high-speed handpiece. Gates-Glidden drills #3 and #4 (Dentsply Maillefer) were used to enlarge coronal and middle thirds of the root canals. ISO #08 K-files (Mani Inc., Utsunomiya, Japan) were inserted into the canals until the tip of the files were just visible at the apical foramen. The file length was measured with a digital caliper (Guanglu, Guilin, China) to the nearest 0.01 mm and the file was shortened by 0.5 mm, set as the gold standard for endodontic file length. Only teeth with a length of 20-24 mm were included. Then, the files were inserted into the canals again and fixed with flowable composite resin (Tetric Flow, Vivadent, Bad Sorgeheim, Germany). Then, to stimulate the clinical situation, the samples were placed in the suitable sockets of a dry human mandible [Table/Fig-1a].
Example of (a) one sample in dry human mandible socket and (b) original and (c) enhanced images
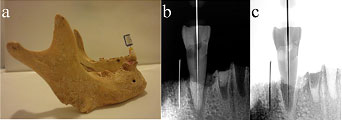
In order to eliminate radiographic magnification, a 10-mm round orthodontic wire was placed in the adjacent dental socket and fixed with wax. A Rinn-Endo-Ray film holder (Dentsply/Rinn Corporation, Elgin, IL, USA) was used to ensure parallelism. The film holder was used to ensure that all samples were imaged at the same geometric situation. The standard geometric configuration was fixed at 30-cm source-to-object distance. Radiographic images of each sample were obtained with the Digora storage phosphor plates (Soredex Corporation, Helsinki, Finland) and its special scanner, Digora Optime (Soredex Corporation), using a Prostyle dental X-ray unit (Planmeca OY, Helsinki, Finland) operating at 63 kVp, 8 mA and 1.5-mm Al-equivalent filtration for 0.03 seconds. The digital images [Table/Fig-1b] were numbered by the Scanora software program version 5.1 (Soredex Corporation, Helsinki, Finland) in a dimly lit room and saved in the DICOM format for further processing and analysis. The “contrast inversion” option was used for each image and the resultant (enhanced) image [Table/Fig-1c] was saved again in the same format. Then, three experienced oral and maxillofacial radiologists and three experienced endodontists determined the endodontic file tip and the most apical portion of the rubber stop of each file in the original and enhanced digital images. They also determined the most coronal and apical points of the orthodontic wire in the adjacent dental socket. The seventh observer measured the endodontic file and orthodontic wire lengths by using the measurement tool of the software program to the nearest 0.1 mm. The magnification coefficient of each image was determined using real and radiographic orthodontic wire lengths measured by the digital caliper and software caliper respectively. To eliminate the magnification effect of radiography, the obtained endodontic file length for each image was divided by the magnification coefficient. Then, the mean values of the radiologists and endodontists measurements were taken as data.
Statistical Analysis
Data were entered and classified in SPSS 15.0 software program (SPSS Inc., Chicago, IL, USA). Data were first verified with the Kolmogorov-Smirnov test for the normality of data distribution. Repeated measures ANOVA and Bonferroni tests were used to compare the gold standard and radiographic file lengths. The level of significance was set at 0.05. Cohen’s kappa statistics was used to assess inter-observer reliability.
Results
The results of the present study are summarized in [Table/Fig-2]. Repeated measures ANOVA showed significant differences between the original and enhanced images and the standard value in endodontic file length measurements (p<0.05). Bonferroni test showed significant differences between the original and enhanced digital radiographs (p<0.05). Enhanced images had longer measurements compared to original images. However, there were significant differences between the two sets of digital radiographs and the standard value (p< 0.05). Both the original and enhanced digital images had a tendency to overestimate the file length measurements [Table/Fig-1]. In addition, inter-observer agreement was excellent for the assessment of digital images with and without enhancement, exhibiting a kappa value of 0.79.
Statistical characteristics of the three groups
| Number | Mean±SD | 95% confidence interval |
|---|
| (mm) | (mm) | SE | LB | UB |
|---|
| Gold standard | 40 | 21.91a±0.98 | 0.16 | 21.60 | 22.23 |
| Original image | 40 | 22.33b±1.23 | 0.20 | 22.93 | 23.72 |
| Enhanced image | 40 | 22.70c±1.45 | 0.23 | 22.24 | 23.17 |
Means with different superscript letters (a,b,c) are statistically different (p<0.05)
SD = standard deviation, SE = standard error, LB = lower bound, UB = upper bound
Discussion
The aim of root canal therapy is to remove the contents of the root canal system [21]. Exact instrumentation, cleaning, shaping, disinfection, and obturation of the entire length of root canals are necessary [21]. Therefore, endodontic length determination is a vital step for successful treatment. There are several methods for determination of working length. Digital radiography has become a routine and popular method for this purpose [22,23]. One of the advantages of digital radiography is the potential for image enhancement. Contrast inversion is one of the most routine enhancements extensively studied in the dental literature for several purposes. In the present study, the effect of this enhancement was evaluated on the accuracy of endodontic file length.
In the present study, endodontic files were placed according to our previous and similar studies that assessed the endodontic file length [3,20,24,25]. In addition, an ISO #08 K-file was used to determine working length because discrimination of small file tips is more difficult in the clinical situation [3]. This difficulty is caused by problems in the selection of the optimal exposure time, the effects of scattered radiation, and differences in bone density. In addition, Kal et al., [3] showed that in enhanced images the mean error of working length determination decreases with an increase in file size.
The results of the present study showed that this enhancement estimates the file length longer than the original image. Therefore, this enhancement decreases the measurement accuracy of the length of small endodontic files on digital periapical radiographs (p<0.05), which might be attributed to the theory that inversion of contrast decreases the visibility of details and changes the observer perception. This could be explained in this way that in the clinical situation, superimposition of fine radiopaque bony trabecula, frequently complicates the diagnosis of the small tip of the endodontic files in the apical third of the tooth. This could be more complicated by inversion of the radiographic contrast. Therefore, this might be resulted in increased probability of misdiagnosis of the endodontic file tip position because of observers’ unfamiliarity with the black radiographic appearance of the endodontic file and bony trabecula.
The results of the present study are in contrast with the results of a study performed by Kal et al., [3]. Although they used the Digora SPPs (Soredex, Orion Corporation, Helsinki, Finland) to produce the original images, the Image J 1.34 software program (National Institutes of Health, Bethesda, MD, USA) was used to produce the enhanced images. In addition, they used acrylic blocks instead of dry human mandibular sockets to mount the teeth. The results of the study performed by Kal et al., [3] showed that the original and enhanced images were not significantly different (p>0.05). The discrepancy in the results of the present and the above-mentioned studies might be attributed to differences in software programs and mounting of teeth.
Fuge et al., [26] used E-speed conventional films to produce radiographic images from teeth. Subsequently, to produce digital images, they scanned the conventional images using a Scanmaker II (Microtek International Inc, Hsinchu, Taiwan R.O.C) flat bed scanner. Then, contrast-inverted images were obtained using the Exchange radiographic system (Software of Excellence, Auckland, NZ). The results indicated that although the digital images were inferior (p<0.001) to the conventional ones in terms of clarity of the small endodontic file tip in relation to the radiographic apex, the original and enhanced images were comparable. These results are in contrast with the results of the present study. These differences might be attributed to indirect acquisition of digital images, type of the software program and lack of hard tissue simulation.
There are some other studies about the effect of contrast inversion enhancement on the measurement and diagnostic accuracy of the dental problems [14–18]. These studies evaluated the measurement accuracy of the interproximal bone loss [15,17] and the diagnostic accuracy of the lesions [14,16,18]. In one study, Eickholz et al., [15] compared the interproximal bone loss determined on the original and enhanced images with the measurements derived from surgery. They showed that the enhanced image had reduced measurement accuracy. In another study, Scaf et al., [17] revealed no significant difference in the measurement accuracy of the interproximal bone loss on the original and enhanced images. Tofangchiha et al., [14] compared the diagnosis ability of vertical root fractures on the original and enhanced periapical images. They showed that the contrast inversion enhancement had no significant effect on the diagnostic accuracy of these images. In addition, Haak et al., [18] revealed that the contrast inversion enhancement had no significant effect on the diagnostic accuracy of interproximal dental caries in digital periapical radiograph. In another study, Raitz et al., [16] evaluated the frequency of the use of the various digital enhancements by the observers to diagnose the radiolucent lesion on panoramic radiograph. They showed that the contrast inversion enhancement had the least frequency of the use. This might be attributed to that the observers are not comfortable with these inverted images.
In addition, the results of the present study showed that both enhanced and unenhanced digital images tended to overestimate the length of endodontic files, consistent with the results of studies performed by Williams et al., [27] and Fuge et al., [26]. In contrast, Schmitd et al., [28] and Brito-Junior et al., [29] reported that the accuracy of endodontic file length measurement on digital images was comparable to the gold standard. This inconsistency might be attributed to the type of receptor (phosphor storage plate versus solid-state detector), type of the software program, and the different situations in which the images were obtained.
Limitation
There were some limitations in the present study. First, the ex vivo model used in this investigation cannot be a complete representation of the conditions in clinical situations. Second, although a storage phosphor plate system was used in the present study, most endodontists benefit from the advantages of solid-state detectors to obtain periapical radiographs during root canal treatment. Third, in clinical situations, the soft tissue overlying the bone might alter the visual characteristics of the image. Fourth, only #8 K-file was used in the present study. The results might be different for smaller or greater files [3, 24].
Conclusion
Contrast inversion enhancement decreased the measurement accuracy of endodontic file length on digital images. Therefore, it is suggested that this enhancement should not be used in determining the lengths of small endodontic files.
Means with different superscript letters (a,b,c) are statistically different (p<0.05)
SD = standard deviation, SE = standard error, LB = lower bound, UB = upper bound