Background and Objectives
Infra orbital nerve block is utilized for postoperative pain control in children undergoing cleft lip repair. This study was conducted to compare the effectiveness, advantages and disadvantages of infra orbital nerve block and opioids for postoperative pain relief following cheiloplasty.
Materials and Methods
Sixty paediatric patients aged 3 months – 13 years undergoing cheiloplasty were selected by simple random sampling and were divided into two groups. All the children received standardized premedication with midazolam, were operated upon under general anaesthesia and the block was performed at the end of surgery before reversal. Group B patients were administered bilateral infra orbital nerve block with 0.25% Bupivacaine (upto 2 mg/kg). Group O patients received Pentazocine 0.5 mg / kg IV. Postoperatively, the heart rate and respiratory rates were recorded every 15 minutes for the first 60 minutes, half hourly till 4 hours and then at 12 and 24 hours. Behavioural assessment for pain / discomfort was done at intervals of ½, 1, 2, 3, 4, 12 and 24 hours. Need for supplementary analgesics and duration between the administration of block/opioid and the first dose of supplementary analgesics were noted. Side effects such as nausea and vomiting, pruritus, respiratory depression and bradycardia during each of these periods were noted.
Results
Both the groups were comparable for age, sex, weight and operative time with no statistical difference. The mean duration of analgesia for infra orbital nerve block was 357.5 minutes i.e. 5 hours 58 minutes and that for opioid was 231 minutes i.e. 3 hours 51 minutes which was significantly lower than the hours of analgesia provided by the block. Further, at the 4th hour, 76.6% of the patients in Group O required supplementary analgesics, in contrast to only 16.6% in Group B. The incidence of nausea and vomiting and pruritus was also higher in Group O.
Conclusion
The results indicate that bilateral infra orbital nerve block provides effective analgesia in the postoperative period, lasting for 6 hours in comparison to 3½ - 4 hours following the administration of intravenous Pentazocine, with no major untoward effects.
Introduction
Cleft lip and palate are common craniofacial abnormalities. The incidence of cleft lip and palate is 1 in 600 live births. Cleft lip repair surgery is most commonly done at 5–6 months of life. Children are special in this regard as it is difficult to differentiate restlessness or crying due to pain from that of hunger or fear [1].
Adequate postoperative analgesia in children is a vital part of perioperative care, as postoperative pain can have adverse physiological effects [2]. Good pain relief minimizes the oxygen requirement, reduces cardio-respiratory demands and promotes early recovery. Regional block given in combination with general anaesthesia provides good pre-emptive analgesia and reduces analgesic requirements in the postoperative period [3]. Bilateral infraorbital nerve block is the local analgesic technique of choice for repair of cleft lip [4].
This study was hypothesized to comparatively evaluate the effect of bilateral infra orbital nerve block with intravenous Pentazocine for postoperative pain relief following cleft lip surgery as fewer comparative studies were done. Pentazocine, a synthetic opioid was selected for this study because it is easily available, cheap and its property of increasing plasma catecholamines accounts for the increase in heart rate which is desirable in infants and children.
Materials and Methods
This study was conducted after approval from the hospital ethical committee and informed parental consent. Sixty paediatric patients between the age group of 3 months – 13 years belonging to ASA Grade I & II undergoing unilateral or bilateral cleft lip surgery were selected on the basis of simple random sampling method and subdivided into two groups of 30 each as follows:
Group B– Bilateral Infra orbital nerve block with 0.25% Bupivacaine (upto 2 mg/kg).
Group O – Intravenous pentazocine (0.5 mg/kg) for postoperative pain relief.
All the patients were operated upon under general anaesthesia. Per-rectal paracetamol suppositories were inserted in all the patients pre-operatively. At the end of surgery and before reversal, infra orbital nerve block or injection Pentazocine was administered. Intravenous paracetamol (10-15mg per kg) was used as a rescue analgesic after extubation, the basal physiological parameters, like heart rate, respiratory rate were recorded every 15 minutes for the first 60 minutes in the recovery room. In the postoperative ward, physiological and behavioural assessment for pain/discomfort scoring was done at intervals of ½, 1, 2, 3, 4, 12 and 24 hours. The scoring system adopted for the present study was based on the one developed by Hannallah et al., and is as shown below:
Interpretation
Minimum score : 0
Maximum score : 8
The higher the score, the greater the degree of pain. A FIVE POINT ‘FACES’ SCALE was also used for behavioural assessment at ½, 1, 2, 3, 4, 12 and 24 hours [Appendex].
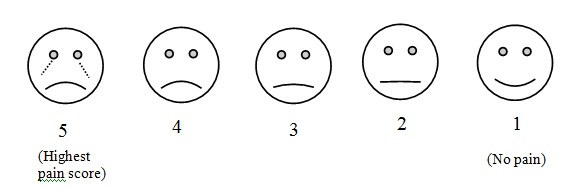
Children below 6 years of age with a total score 4 and children above 6 years complaining of pain were considered to have inadequate pain relief. Intravenous paracetamol was used as rescue analgesic for these patients less than 6 years with a total pain score of 4 and on complaints of pain in children more than 6 years. Postoperative complications, nausea/vomiting, pruritus, respiratory depression, bradycardia, cyanosis were also noted.
Statistical Analysis
The data collected was tabulated according to various epidemiological and statistical parameters. Analysis was done using arithmetic mean, standard deviation, standard error and t-test. Analysis of variance (ANOVA) was also used for the analysis.
Results
The demographic profile and mean duration of cheiloplasty was comparable among both the groups. Heart rate (HR) and respiratory rate showed more or less a constant change in both the groups over the first two hours. After two hours, there was a gradual increase in HR in Group O reaching a peak at 3 ½ -4 hours. In comparison, the heart rates in Group B had lower values till 6-8 hours peaking at around 12 hours postoperatively. Thus there is a differential change in hours within the Groups (p<0.001) which is statistically highly significant. The difference in Hours comparing both the groups is statistically significant (p<0.013). A similar trend was observed in the respiratory rate over the time.
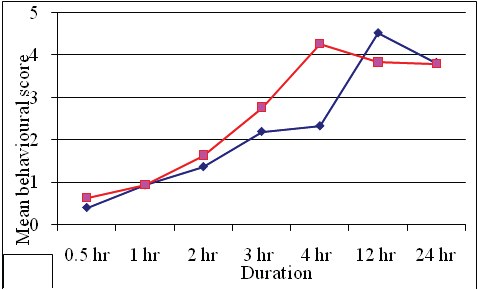
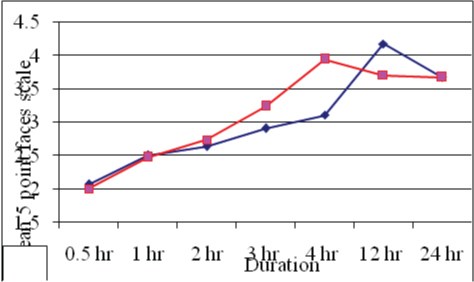
There was a statistically highly significant (p<0.001) change in both behavioural and five point faces scale from 1st to 24 hours. Group B had lower scores compared to group O upto 4 hours following which the scores kept on increasing in group O. While the scores in group B were still lower compared to group O till 12 hours. However, at 24 hours, there was no difference in the scores. With respect to median values, again group B had lower values. At the 4th hour while group O achieved higher median scores, group B continued to have lower scores [Table/Fig-2], Mean pain discomfort scores over duration [Table/Fig-3], (Mean five point faces score over duration).
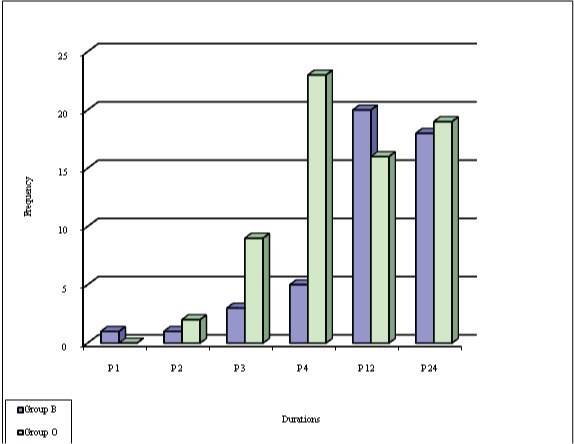
No patient in Group B required supplementary analgesics by the 1st hour. However, in Group O one patient (3.33%) required analgesic by the 1st hour. At the 2nd and 3rd hour, in Group B, 3.33% and 10% of patients had pain score ≥ 4 while in Group O, the patients with pain score ≥4 increased from 6.7 % at 2nd hour to 30% at 3rd hour. At the 4th hour, 16.67% of children in group B had pain score ≥ 4 in comparison to 76.67% in Group O and this difference was highly significant (p<0.001). Thus the requirement of supplementary analgesic was markedly increased in Group O by the 4th hour while it was still less in group B. By 12th and 24th hour, however, the number of patients with pain score ≥ 4 was almost comparable in both the groups [Table/Fig-4].
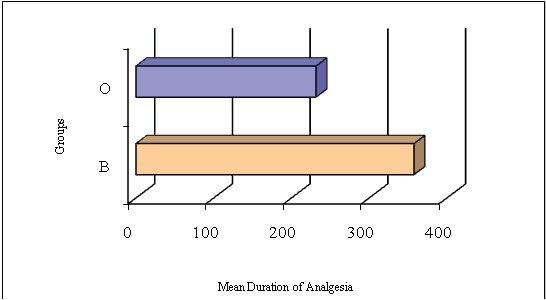
Duration of analgesia: The mean duration of analgesia in group B was 357.5± 42.12 minutes. In comparison, the mean duration of analgesia in Group O was 231.5 ± 25.4 minutes which was highly significant statistically (p<0.001) [Table/Fig-5], (Mean duration of analgesia for various groups).
Only one patient had nausea and vomiting in group B compared to 5 (16.67%) in Group O. No patient had pruritus in Group B compared to 2 (6.67%) in Group O. There was no incidence of respiratory depression, bradycardia or cyanosis in any of the groups.
Discussion
Children suffer postoperative pain in the same way as adults. Pain is a subjective quality that is particularly difficult in children to define and quantify. In fact, even today reliable and objective indicators of pain in children are not available [5]. Self-reporting is only possible in older children or those with considerable cognitive and communicable abilities.
Awareness and treatment of postoperative pain in children has improved over the past few years. Improved postoperative analgesia and shortened recovery have provided further impetus for refinement of techniques that can be used safely in combination with general anaesthesia in children.
Cleft lip repair is a common operation in infants and requires that the child is pain free during the postoperative period so that handling does not affect the integrity of the delicate surgery. While infraorbital nerve block is an established technique of analgesia during repair of upper lip lacerations in adults, its use in cleft lip repair has been controversial [6]. Various studies have shown that bilateral infraorbital nerve block is a simple and effective postoperative pain reliever in children following cheiloplasty. It is associated with postoperative haemodynamic stability, rapid and complete recovery and reduced analgesic requirement in the postoperative period [7]. Opioids are the mainstay in the management of postoperative pain in paediatric patients
None of the patients receiving infraorbital nerve block had any local or systemic undesirable effects associated with the local anaesthetics in the present study. In the present study, there was a gradual decrease in HR and respiratory rate followed by more or less a constant HR and RR in both the groups for first two hours. But after two hours, there was an increase in HR and RR in group O reaching a peak at 3½ to 4 hours while HR and RR continued to have lower values till 6-8 hours in Group B. (p< 0.001) [8]. However, the two groups did not differ significantly in the patterns of respiratory rate. At the end of the 3rd hour, 30% of patients in Group O had pain score ≥ 4, and hence received rescue analgesics compared to only 10% in Group B. At the 4th hour, there was a significant difference in the median values in the two groups. The median values of pain discomfort score in group O was 4 compared to 2 in Group B. The mean value of five point faces scale in group 0 was 5 (maximum pain) compared to 3 in Group B. Thus 76.6% of patients in Group O had pain discomfort score ≥ 4 and receiving supplementary analgesics compared to only 16.6% in Group B. Thus, indicating that the analgesic effect had worn off in Group O, while a significant number of patients in Group B continued to have adequate analgesia even after 4 hours. Ahuja S et al., conducted a similar study and concluded that the infants receiving infra orbital nerve block require less analgesics in the postoperative period [9]. Nicodemus et al., observed similar results in their study [10]. The pain discomfort scores 4 hours after the operation showed that none of the patients in the group receiving infraorbital nerve block were in pain, in contrast, 11 patients in the other Group were in mild to severe pain and required analgesics.
By the end of 12th and 24th hour, both the groups B & O had comparable and high median values of pain discomfort scores (4 and 5) as well as five point faces scale. This indicated that in both the groups, the analgesic effect had worn off by 12th and 24th hour and the analgesic requirements were also comparable in both the groups at 12th and 24th hour. A study conducted by Rajamani et al., [11] showed that patients with infraorbital nerve block had mean pain scores of 2.81 while the group receiving opioid had a higher mean pain score of 4.71. A study by Mane RS et al., [12] observed that infraorbital nerve block when given before incision has approximately 100% success rate with minimal complications. Takmaz SA et al., [13] observed that bilateral infraorbital nerve block administered at the end of surgery provides satisfactory analgesia with high parental satisfaction and lower complication rates and reduces rescue analgesic consumption in patients undergoing cleft lip repair which is in accordance with our study.
Pain/ Discomfort Scoring used in present study
| Parameters | Findings | Points |
|---|
| Crying | Not crying | 0 |
| Responds to age Appropriate Nurturing | 1 |
| Does not respond to Nurturing | 2 |
| Movements | No movements, relaxed | 0 |
| Restless, Moving in Bed | 1 |
| Thrashing (Rigid) | 2 |
| Agitation | Asleep or calm | 0 |
| Can be comforted to lessen Agitation | 1 |
| Cannot be Comforted | 2 |
| Complains of pain | Asleep/ States no pain | 0 |
| Cannot Localize | 1 |
| Localizes pain | 2 |
Mean Pain discomfort score over duration
Five point faces score over duration
Frequency and percentage of pain discomfort score >=4 for various groups
Mean duration of analgesia for various groups
Conclusion
• Bilateral infra orbital nerve block with plain Bupivacaine 0.25% provides effective postoperative analgesia in children following cheiloplasty, lasting for about 6 hours, compared to 3½ - 4 hours following Pentazocine 0.5 mg / kg IV.
• Infraorbital nerve block is a simple procedure which is easy to perform, safe and is free of complications the block promotes easier nursing care and greater parental wellbeing.
• IV pentazocine caused nausea and vomiting in 16.67% and pruritus in 6.67% of patients. But after infraorbital nerve block, there was no incidence of any of the above side effects.
[1]. M Yaster, Analgesia and anaesthesia in neonatesJ Pediatr 1987 111(3):394-96. [Google Scholar]
[2]. Shankar V, Painless Procedures in PaediatricsIndian Pediatr 2006 43(4):295-99. [Google Scholar]
[3]. B Beilin, H Bessler, E Mayburd, G Smirnov, A Dekel, I Yardeni, Effects of Preemptive Analgesia on Pain and Cytokine production in the postoperative periodAnaesthesiology 2003 98(1):151-55. [Google Scholar]
[4]. Law RC, Klerk C, Anaesthesia for cleft lip and Palate SurgeryUpdate in Anaesthesia. 2002 14:27-30. [Google Scholar]
[5]. W Buttner, W Finke, Analysis of behavioural and physiological parameters for the assessment of postoperative analgesic demand in newborns, infants and young children, a comprehensive report on seven consecutive studiesPaediatr Anaesth 2000 10(3):303-18. [Google Scholar]
[6]. V Gaonkar, R Daftary Swati, Comparison of preoperative block with peri – incisonal infiltration for postoperative pain relief in cleft lip surgeriesIndian J Plast Surg 2004 37:105-09. [Google Scholar]
[7]. PK Prabhu, J Wig, S Grewaly, Bilateral infraorbital nerve block is superior to periincisional infiltration for analgesia after repair of cleft lipScand J Plast Reconstr Surg Hand Surg 1999 33(1):83-87. [Google Scholar]
[8]. AT Bosenberg, FW Kimble, Infraorbital nerve block in neonates for cleft lip repair; anatomical study and clinical applicationBr J Anaesth. 1995 74:506-08. [Google Scholar]
[9]. S Ahuja, A Datta, A Krishna, A Bhattacharya, Infraorbital nerve block for relief of post operative pain following cleft lip surgery in infantsAnaesthesia 1994 49(5):441-44. [Google Scholar]
[10]. HF Nicodemus, MJR Ferrer, VC Cristobal, L Castro, Bilateral infraorbital block with 0.5% Bupivacaine as postoperative analgesia following cheiloplasty in childrenScand J Plast Reconstr Hand Surg 1991 25:253-57. [Google Scholar]
[11]. A Rajamani, V Kamat, VP Rajavel, J Murthy, SA Hussain, A comparison of bilateral nerve block with intravenous fentanyl for analgesia following cleft lip repair in childrenPaediatr Anaesth 2007 17(2):133-39. [Google Scholar]
[12]. RS Mane, CS Sanikop, VK Dhulkhed, T Gupta, Comparison of Bupivacaine alone and in combination with fentalyl or pethidine for bilateral infraorbital nerve block for postoperative analgesia in paediatric patients for cleft lip repair: A Prospective randomized double blind studyJ Anaesthesiol Clin Pharmacol 2011 27(1):23-26. [Google Scholar]
[13]. Takmaz Suna Akin, Uysal Hale Yarkan, Uysal Afsin, Kocer Ugur, Dikmen Bayazit, Baltaci Bulent, Bilateral Extraoral, Infraorbital Nerve Block for Postoperative Pain Relief After Cleft Lip Repair in Pediatric Patients A Randomized, Double-Blind Controlled StudyAnnals of Plastic Surgery 2009 63(1):59-62. [Google Scholar]