Foray of Cytologically Diagnosed Intramuscular Sarcocystosis- A Rarity
Hemalatha Anthanahalli Lingappa1, Anoosha Krishnamurthy2, Ashok Kagathur Puttaveerachary3, Abhishek Mandya Govindashetty4, Swati Sahni5
1Professor, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B. G. Nagar, Mandya district, Karnataka, India.
2Post Graduate, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B. G. Nagar, Mandya district, Karnataka, India.
3Post Graduate, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B. G. Nagar, Mandya district, Karnataka, India.
4Associate Professor, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B. G. Nagar, Mandya district, Karnataka, India.
5Post Graduate, Department of Pathology, Affiliated to Rajiv Gandhi University of Health Sciences, B. G. Nagar, Mandya district, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hemalatha Anthanahalli Lingappa, No: 156, 12th Cross, 2nd Main, Jayanagar, Mysore- 570014, India.
E-mail: halingappa@gmail.com
Sarcocystosis is an uncommonly encountered zoonotic coccidial protozoal infestation of human beings. The sarcocystis species is known to produce intestinal and muscular infestations in humans. We report a rare case of a 35-year-old female with an intramuscular swelling in the lumbar region diagnosed cytologically as “Intramuscular Sarcocystosis” and subsequently confirmed on histopathology. This case highlights the role of fine needle aspiration cytology in the identification of Sarcocystis and its role in differentiating it from other intramuscular parasites which is of immense value in precise diagnosis and appropriate patient management.
Infestation, Parasitic cyst, Sarcocystis
Case Report
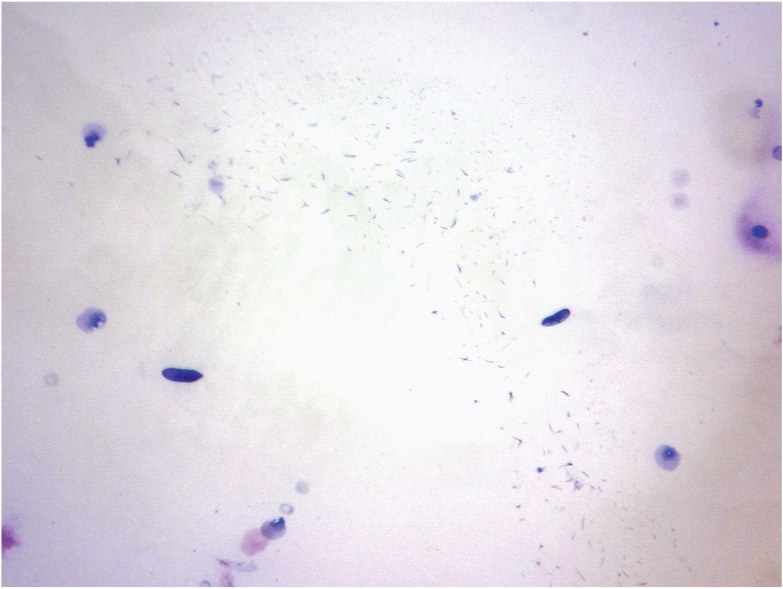
A 35-year-old female patient presented to the FNAC clinic with a painful mass in the right lumbar region observed since a fortnight. On local examination, the swelling was found to be solitary and ill-defined, measuring 2 cms across. It arose from the muscular plane, had soft to cystic consistency and was mildly tender with restricted mobility. FNAC aspirate yielded 0.5 ml of straw- coloured fluid material intermixed with whitish solid fragments. Smears stained by May- Grunwald Giemsa and Haematoxylin and eosin revealed a few banana shaped structures against a mixed inflammatory background [Table/Fig-1,2]. A cytological diagnosis of parasitic cyst suggesting the possibility of Sarcocystis was signed out.
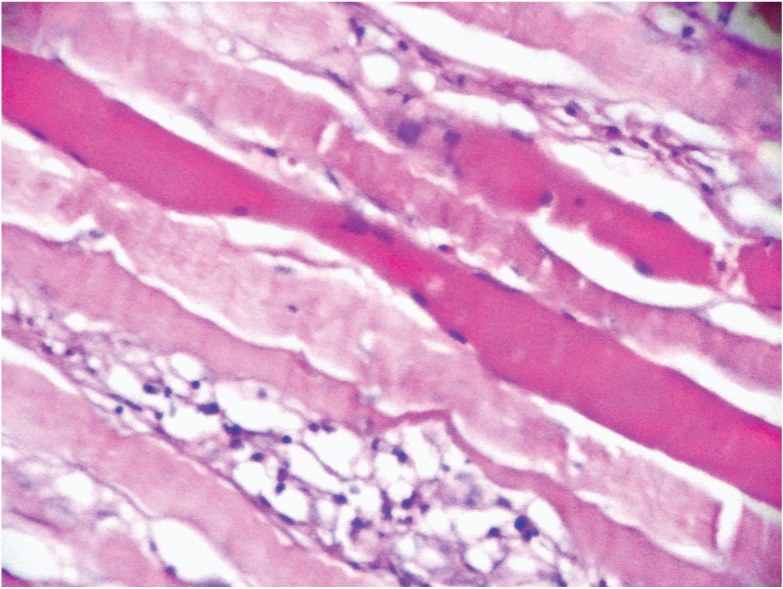
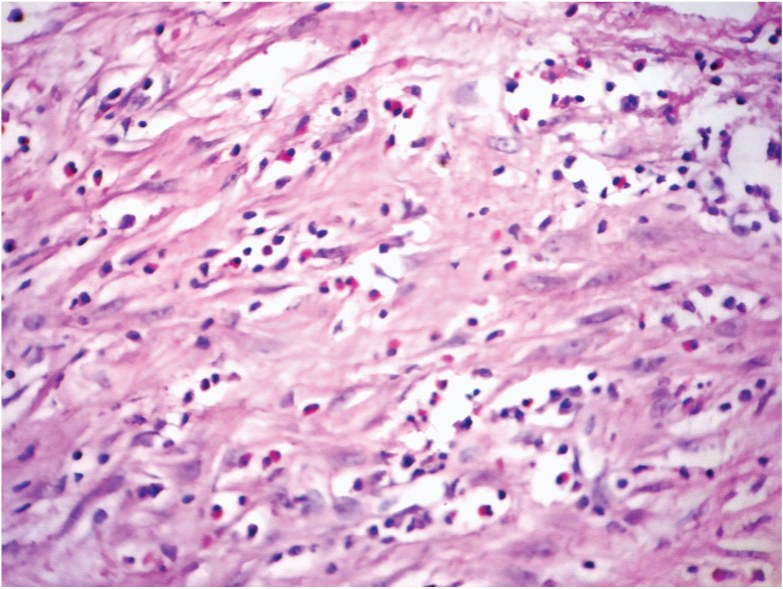
Laboratory investigations- Peripheral blood smear examination revealed marked eosinophilia. The absolute eosinophil count was found to be markedly elevated at 975/μl (Normal range- 40-400/μl). The Erythrocyte Sedimentation Rate was found to be elevated at 40 mm/hour (Normal range- 0-29mm/hour) and the serum creatine kinase levels were at 214 U/l (Normal range-38-176 U/l). Ultrasonography report revealed- “A benign cystic lesion of probable parasitic aetiology”. A wide excision was performed and the specimen was submitted for histopathological examination. Gross examination showed an irregular grey- white to grey-brown tissue bit measuring 3 x 2.5 x 0.5 cms. A focal cyst- like area measuring 1.5 x 0.7 cms was seen. Microscopy revealed skeletal muscle bundles with large areas of myolysis admixed with chronic inflammatory cell infiltrates [Table/Fig-3]. The predominant cells were eosinophils [Table/Fig-4]. At places, the inflammatory cell aggregates were seen surrounding a linear central degenerated structure with indistinct morphological features [Table/Fig-5]. Final correlative Cytohistological diagnosis-Intramuscular parasitic granuloma-Sarcocystis.
Discussion
Human muscular sarcocystosis is a rare parasitic infestation caused by the coccidian parasite belonging to the family Sarcocystidae. The invasive forms in muscular Sarcocystosis are considered to belong to a single species of Sarcocystis namely S lindemanni where man acts as an intermediate host while dogs or cats act as definitive hosts. Humans acquire infection by ingestion of water or food contaminated with faeces of cat or dog containing sporocysts of S. lindemanni. Diagnosis is suspected based on various criteria including clinical presentation, muscle biopsy findings and laboratory investigations such as eosinophilia and elevated serum creatine kinase levels [1,2]. The patient in the present case presented with the usual clinical signs and symptoms and the provisional clinical diagnosis of a parasitic cyst based on ultrasonography findings. There was no history of exposure in this case. The unique aspect of the present case is the diagnosis of this rare lesion on cytology. In fact, the parasitic morphology was clearer on cytological aspirate smear than in the paraffin sections. The definitive species identification was possible only on cytology smears since the parasitic morphology was obscured due to myonecrosis on histology. This fact upholds the utility of cytology as a better and more reliable diagnostic aid than histology in specific situations like the present one. Extensive search of available literature did not reveal any report of muscular Sarcocystosis diagnosed on cytology.
Sarcocystis was first seen as white thread- like cyst in the skeletal muscle of a house mouse. It was reported as early as 1843 by Meischer and was hence referred to as ‘Meischer’s tubules’. In 1967, the crescent shaped bodies (Bradyzoites) were identified on electron microscopy. Sarcocystis species are intracellular protozoan parasites which have an obligatory two host cycle [1].
The sexual reproduction (Gametogony and Sporogony) takes place in the intestine of an omnivore or carnivore (Definitive host) whereas, the asexual reproduction (Schizogony) occurs in the tissue of an herbivore (Intermediate host). Human beings double up as both definitive and intermediate hosts [2].
Sarcocystis causes intestinal and muscular infestations in humans. The former is caused by S. hominis and S. suihominis and the latter by S. lindemanni [3,4]. Muscular Sarcocystosis is common in non- human primates [5]. Man acquires the infection following ingestion of food or drinks contaminated with faeces of cat or dog containing the oocyst [2]. Each oocyst releases 4 sporozoites into the intestine. Schizonts are formed in the capillary endothelium following penetration of intestinal mucosa. Subsequently, asexual multiplication occurs leading to Haematogenous dissemination of merozoites which invade the muscular microcirculation and harbour the sarcocysts [6,7].
An inflammatory reaction ensues in the muscles, composed predominantly of eosinophils and lymphocytes [8] as in the present case, which causes a wide spectrum of symptoms such a myalgia, swelling, fever, weakness, vasculitis, eosinophilia [4,9] and myonecrosis [10]. Arness et al., reported elevated ESR and serum kinase levels [10] which was also observed in our case along with absolute eosinophilia.
A presumptive diagnosis of Sarcocystosis is based on history of recent consumption of undercooked or raw meat [11,12]. Ancillary diagnostic studies such as PCR and serological testing to check for antibodies and prior exposure are also helpful [2]. This case highlights the importance of FNAC as a preliminary diagnostic modality in distinguishing intramuscular Sarcocystosis from other intramuscular parasites such as Cysticercus cellulosae and Echinococcus granulosus. Contrary to the popular belief that histopathology is the gold standard for final diagnosis and definitive sub typing of lesions, the present case proves that cytology can occasionally overtake histopathology. The cytologically aspirated material in the present case had distinctive morphological features of bradyzoites which were actually more distinctive than the degenerated parasitic structure with indistinct morphology as seen on histopathology.
There is no known prophylaxis or specific treatment for infestation with Sarcocystosis [1,2]. Corticosteroids have been recommended for symptomatic relief. Wide excision is curative and is associated with an excellent prognosis [2].
FNAC smear showing banana shaped bradyzoites of S. lindemanni, (MGG, ×1000)
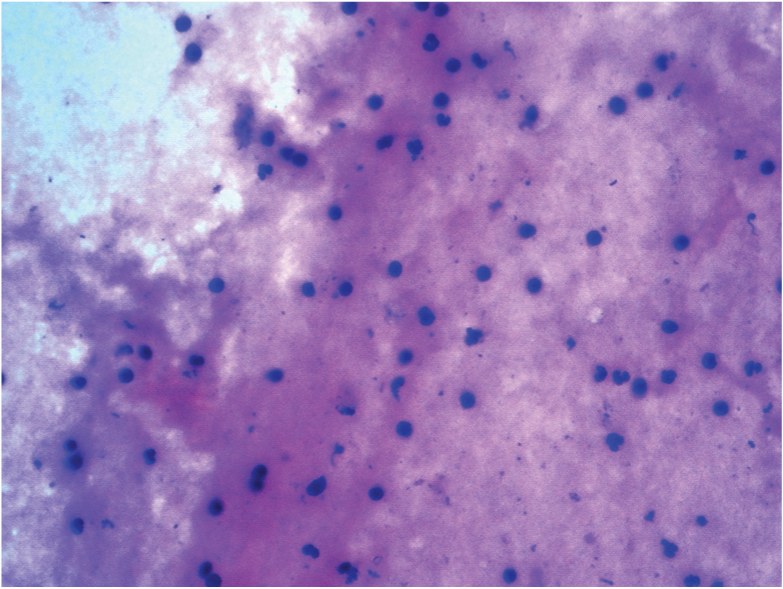
FNAC smear showing mixed inflammatory background, (H&E,×400)
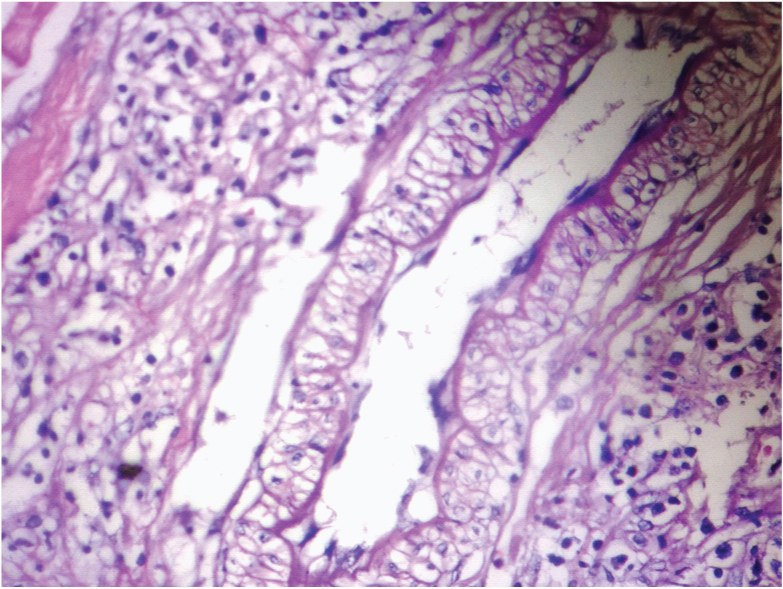
Large areas of myonecrosis and inflammatory infiltrates, (H&E,×400)
Granuloma with predominance of eosinophils, (H&E,×400)
Linear central degenerated parasitic structure amidst dense inflammatory background, (H&E,×400)
Conclusion
Clinicians need to be sensitized to the fact that FNAC is a useful diagnostic tool in establishing precise diagnosis of even rare entities like intramuscular Sarcocystosis. Besides this, it also helps exclude other intramuscular parasitic infestations. In developing countries, mass awareness programs regarding good hygienic habits, proper storage and cooking of meat and most importantly proper disposal of excreta are quintessential to aid in prevention.
[1]. R Fayer, Sarcocystis spp. in human infectionsClinical microbiology reviews 2004 16:894-902. [Google Scholar]
[2]. N Larbcharoensub, W Cheewaruangroj, P Nitiyanant, Laryngeal Sarcocystosis accompanying laryngeal squamous cell carcinomaCase report and literature review 2011 42(5):1072-76. [Google Scholar]
[3]. JK Frenkel, Sarcocystosis In: Connor DH, Chandler FW, Schwartz DA, et al, eds. Pathology of infectious diseases 1997 2Washington DCAppleton & Lange:1253-59. [Google Scholar]
[4]. Y Gutierrez, The tissue Apicomplexa: Sarcocystislindemanniand Toxoplasma gondii. In: Di¬agnostic pathology of parasitic infections with clinical correlations 1990 PhiladelphiaLea & Febiger:108-35. [Google Scholar]
[5]. DS Lindsay, Blagburn BL, Braundw KG, Sarcocystis spp. and SarcocystosisBAM 1995 5(3):249-54. [Google Scholar]
[6]. R Pathmanathan, SP Kan, Human Sarcocystis infection in MalaysiaSoutheast Asian J Trop Med Public Health 1981 7:247-50. [Google Scholar]
[7]. KT Wong, R Pathmanathan, High prevalence of human skeletal muscle Sarcocystosis in south-east AsiaTrans R Soc Trop Med Hyg 1992 86:631-32. [Google Scholar]
[8]. R Pamphlett, P O’Donoghue, Sarcocystis infection of human muscleAust NZ J Med. 1990 20:705-07. [Google Scholar]
[9]. R Fayer, Sarcocystisspp. in human infectionsClinMicrobiol Rev 2004 17:894-902. [Google Scholar]
[10]. MK Arness, JD Brown, JP Dubey, RC Neafie, DE Granstrom, An outbreak of acute eosinophilic myositis due to human SarcocystisparasitismAm J Trop Med Hyg 1999 61:548-53. [Google Scholar]
[11]. S Bunyaratvej, P Bunyawongwiroj, P Nitiyanant, Human intestinal sarcosporidiosis: report of six casesAm J Trop Med Hyg 1982 31:36-41. [Google Scholar]
[12]. A Saleque, PD Juyal, BB Bhatia, Effect of temperature on the infectivity of Sarcocystismeischerianacysts in porkVet Parasitol 1990 36:343-46. [Google Scholar]