With the scientific and technological advancement in medicine, dentistry and other areas of health, there has been significant increase in life expectancy [1], and as a result of aging, general prevalence of chronic diseases has increased, as these occur more frequently in persons of this age group. This may be translated into a greater demand for health services and financial resources for the treatment of these diseases and the consequent disablement they cause. In addition to the greater prevalence of these diseases in the elderly population, and as a result of these, one observes that the elderly have greater difficulty to maintain themselves functionally independent and active in society, leading to their social exclusion. As regards oral health care, Frenkel et al., [1] in their study, found a high degree of dependence on help with this care because an average of 82% of the volunteers considered it difficult or impossible to clean their dentures. This study confirmed the presence of limitation in cleaning dentures, probably as a result of functional alterations inherent to aging.
For the maintenance of oral health, biofilm control is essential. The denture-mucosa interface is an ideal medium for biofilm formation, and this process is favoured by diminished salivary flow, roughness of the material due to surface irregularities and temperature in the mouth of around 37°C [2]. The quantity of microorganisms found on the denture base is greater than that on the surface of the palate, which indicates that acrylic resin acts as a reservoir of infection [3]. The effects of poor oral hygiene are also related to systemic health. The micro organisms presents in biofilm act as a source of infection, which may be aspirated, causing pneumonias, especially in bed-ridden and/or hospitalized patients; gastrointestinal problems, or affect the bloodstream and lead to cardiovascular problems [1,4,5].
The most popular method of removing biofilm from dentures is brushing with dentifrice [6,7]. If correctly performed, this method efficiently removes accumulated biofilm. Nevertheless, effective biofilm removal requires a degree of manual dexterity and visual acuity which is frequently diminished, especially in the elderly [8].
As an alternative for cleaning the dentures of patients with some motor limitation of the hand, especially in cases of arthritis or after a stroke, adaptation of a device to toothbrush handles can be indicated [9]. This device increases the volume of the handle and makes it easier to use the brush, thereby enabling the patient to perform brushing by him/her, consequently diminishing his/her dependence and improving self-esteem, thereby contributing to the maintenance of the elderly patient’s functional capacity. In view of the above considerations, the aim of this pilot study was to evaluate the effectiveness of toothbrushes with handles individually adapted with the use of acrylic resin, in the reduction of biofilm on complete dentures of elderly patients in the Municipality of Cascavel, PR, Brazil.
Materials and Methods
This prospective, randomized, pilot study, was approved by the Ethics Committee on Research in Human Beings of São LeopoldoMandic School Dentistry and Research Denter, Brazil, protocol 2006/0201, and held at Condominium of the Third Age, Cascavel-Paraná, Brazil between August and December 2006.
Selection of Volunteers
Residents of the Condominium of the Third Age, Cascavel-Paraná, Brazil, who were functionally independent, in a good state of cognition, and wearers of complete maxillary dentures participated in the research. Elderly persons whose denture bases had defects (fractures, deep cracks) and/ or presence of relining materials, and denture that had been in use for over 20 y were excluded from the sample.
All 85 residents of the Condominium for the Elderly were evaluated, after they consented to participate in the study. They were submitted to the Barthel Test [10] to evaluate the patients’ functional independence. To evaluate the cognitive capacity, the instrument for tracing cognitive compromise, denominated Mini Mental-State Examination (MMSE) was applied [11]. As the MMSE scores are subject to significant influence of the individual’s age and schooling, differentiated cut-off points were used [12]. For elderly persons without schooling, the cut-off point was 19, and for those with some schooling the cut-off point was 23 [13].
Complete maxillary denture wearers were selected and answered a questionnaire with personal data and questions related to oral health and the prosthetic appliance. The clinical oral exam was performed by a single, previously trained dentist. This professional verified the presence of oral lesions related to the denture and its condition, to meet the above-mentioned inclusion and exclusion criteria.
After the mentioned exams and evaluations, 16 elderly subjects were included in this experiment, and were randomly divided into 2 experimental groups (n=8): Group 1: Adapted toothbrushes handles and Group 2: Toothbrush without adaptation – conventional type.
Fabrication of toothbrush handle devices
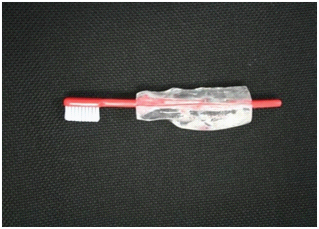
The devices for the patients of Group 1 were fabricated using heat-polymerized acrylic resin, after having obtained the silicone mold in the shape in which the brush would be held by the participant, [Table/Fig-1]. The technique for fabricating the device was the same as that described by de Mattos et al., [9] [Table/Fig-2].
Molding of patient’s hand with condensation silicone

Finalized toothbrush adaptation device
Application of the Experiment
The patient’s dentures were evaluated at three time intervals: A – In the beginning, B - After 7 days and C - After 21 days of using the toothbrush handles. The two groups were instructed to conventional denture hygiene and received new toothbrushes for denture cleaning. For comparative evaluation of the quantity of biofilm, the method used was staining, which is most commonly mentioned in the literature [14]. The revealer used on the internal surfaces of the denture bases was 5% erythrosine, as it has good staining capacity and is easily removed [15].
After the staining procedures, the dentures were placed on a platform at an angle of 45°, with the bases facing upwards, in order to take the photographs with a digital camera (Canon Rebel XT), in a standardized manner. Focus was centered on the median palatal raphe, halfway between the maxillary labial frenum and the posterior base of the denture [2]. The use of photographs contributed towards the limitation of the visual method, with low reproducibility and subjectivity [16].
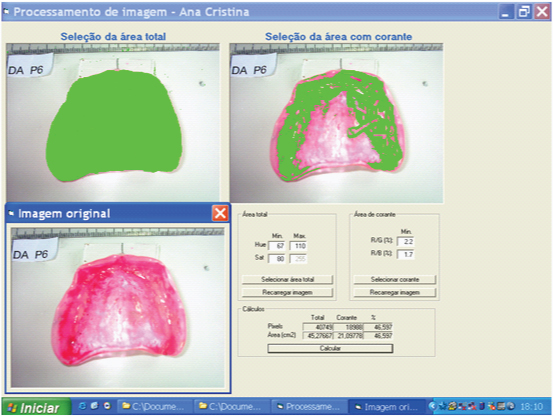
The digital images obtained were analysed with Image Tool® software, by means of which the total area of the internal surface of the denture base and area covered by biofilm were calculated [Table/Fig-3]. The results were expressed in percentage of stained area in relation to the total area of the internal surface of the denture base.
Software used for biofilm quantification, result expressed in % of area covered by biofilm in relation to total area of the internal surface of the denture base
Statistical Analysis
All analyses were performed with Biostat version 5.0 software, using Friedman’s test (Non-Parametric Repeated Measures Comparisons), p < 0.05.
Results
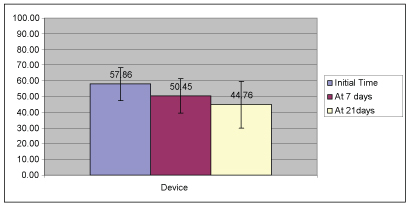
The final sample consisted of 16 elderly persons, 05 being men (31%) and 11 women (69%), age-range from 61 to 85 y of age, mean age of 73 y. The mean quantity of biofilm verified in Groups 1 and 2, at the three time intervals of the experiment may be seen in the figures [Table/Fig-4,5].
Mean values of biofilm quantification in patients of Group 1 (adapted toothbrushes handles) at the time intervals: initial, after 7 and 21 days (%)
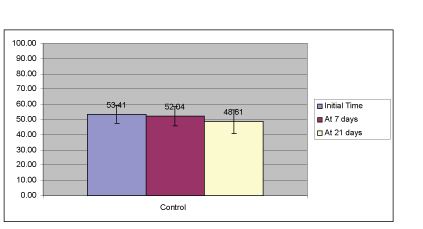
Mean values of biofilm quantification in patients of Group 2 (without adapted device) at the time intervals: initial, after 7 and 21 days (%)
The data obtained for Groups G1 and G2 were submitted to statistical analysis comparing the difference between the values obtained at the three time intervals of evaluation for each group separately [Table/Fig-6].
Mean values and standard deviation of biofilm quantification on complete denture bases, considering the groups G1 and G2 evaluated (%)
| Group | Time Interval |
|---|
| Initial | 7 days | 21 days |
|---|
| Device (G1) | 57.86 (+ 10.55) a | 50.45 (+ 10.97) ab | 44.76 (+14.86) b |
| Control (G2) | 53.41 (+ 5.76) a | 52.04 (+6.33) a | 48.61 (+7.72) a |
Different letters on the same line indicate means with statistically significant differences
Discussion
Among the limitations perceived in patients with chronic diseases such as arthritis, for example, is the difficulty they have with holding objects, which may harm the cleaning of their teeth and dentures. The proposal of this research was to verify the reduction in biofilm on complete dentures in a comparative manner, between toothbrush handles individually adapted, and conventional toothbrushes. In addition to contributing towards the individual’s local and systemic health, it is in line with a broad concept of health in the elderly, which is directly related to maintenance of independence in daily life activities [17].
The initial results in both groups revealed a large accumulation of biofilm on the internal base of the dentures, on an average covering 55% of the internal area. These results corroborate the studies of other authors who affirmed that there are few complete denture wearers who are able to maintain them effectively cleaned [3,18–20].
Although there are toothbrushes on the market specifically for denture cleaning [21], they present a relatively high added value when compared with conventional toothbrushes. Furthermore, the handles have not been modified to meet the demand of patients with some type of motor limitation of the hands. In the present study, the option was to use conventional, low cost toothbrushes, accessible to a large part of the population, and approved by the Brazilian Dental Association, making it possible to change the toothbrush and keep the same device. These toothbrushes received acrylic resin adaptations on their handles, which were personalized for each participant in the experimental group, according to his/her hand-grip.
It should be pointed out that the group of elderly persons studied was composed almost entirely of illiterate persons with an income medium of one minimum wage brazilian, approximately US$ 310.00 per month, Lima-Costa et al., [21] affirmed that even small differences in monthly income are sufficiently sensitive to enable one to identify elderly persons in worse conditions of health in Brazil. The relationship between low income and dependence reinforces the importance of studies directed towards this portion of the population, with the goal of maintaining physical and mental abilities necessary for living an independent and autonomous life.
The results of this pilot study showed a reduction in mean biofilm for both groups. This may be related to the influence of the intervention and monitoring. Nevertheless, it was only for Group 1, which used the device, that the reduction was statistically significant between the evaluated time intervals. Thus, the results point out that the device adapted to the toothbrush handles showed superior competence for biofilm reduction on the internal surface of the base area of complete dentures, proving its effectiveness, and reinforcing its indication to potentiate motor capacity in elderly persons for the purpose of cleaning their dentures [9,22,23].
Customizing of toothbrush handles to improve the hand-grip on toothbrushes is something the dentist can do with materials available in the dental office [9,23]. Although acrylic resin is low cost, the working time for fabricating the device is long, and generally demands the help of a dental prosthesis technician. With the goal of making the technique easier and reducing the laboratory steps for fabricating personalized devices, one option would be to use heat polymerized resins [23], however, the cost of the light polymerizing box must be considered. Further researches that evaluate other materials are necessary, in order to associated the practicality of the technique with a lower cost.
In view of the results obtained in this pilot study as regards significant reduction in biofilm on complete dentures in the group that used the adapted toothbrushes, one understands that the devices adapted to toothbrush handles could be encouraged to a larger extent, particularly in the group of elderly patients. In addition to enabling them to remove biofilm from their dentures more efficiently, it would allow them greater independence in performing their daily life activities, especially in the case of patients who have difficulty with their hand-grip.
Conclusion
The use of toothbrushes whose handles were individually adapted with the proposed acrylic resin devices was shown to be more effective in reducing biofilm on dentures when compared with the group of volunteers who used conventional toothbrushes.
Different letters on the same line indicate means with statistically significant differences