Silver amalgam has been the material of choice worldwide for class I and class II restorations for more than a century. But acceptance of amalgam began declining in the early 1980’s due to problems like corrosion, difficulty in bonding to tooth structure, the necessity to remove more of sound tooth structure for enhancing the retention, lack of aesthetics and mercury toxicity [1].
Both the declining acceptance of amalgam and patients’ interest in dental aesthetics have resulted in the development of new tooth coloured restoratives and techniques [2]. Lutz calls it the “Post Amalgam Age” [3]. The composites were first introduced in the 1960s. A major step in composite technology occurred in the 1970s with the introduction of light cured composite resins such as Nuva-Fil (DENTSPLY). In the early 1980s, resins especially for posterior use appeared. In the mid-1980s, significantly improved light-cured composite resins intended for universal use called hybrids which had a particle size of approximately 1μm were introduced. Despite advances that have been made, many clinical and material limitations have restricted the universal use of resin composites as posterior restorative materials. One of the most undesirable characteristic of composite resin is its polymerization shrinkage [4].
The factors involved in shrinkage stress are: the cavity geometry which includes configuration factor and cavity size; the placement technique which includes, layering and light curing mode and the restorative material which includes stiffness (modulus of elasticity) and dimensional change (shrinkage) [5]. For posterior composite resins restorations, several procedures have been developed to counter this sealing problem.
Oblique layering technique with increments (1 to 1.5 mm in depth) of wedge- or triangle-shaped, which allows the composite to be placed in such a way as to produce lowest C factor [6].
Low polymerization shrinkage due to oxirane monomers and increased hydrophobicity due to the presence of siloxane species in its composition gives the resin its added advantages [7,8].
Many studies have reported that polymerization of a resin composite can create shrinkage stress that may disrupt the bond to the cavity wall [9].
A recent method designed to reduce shrinkage stress consists of reducing the initial conversion, which controls the flow capacity of resin composite. The pulse mode and soft-start polymerization techniques may increase the marginal integrity of resin composite restorations without affecting the polymerization of the material [10,11].
So, the present study was designed to compare the effect of two different placement techniques and two different curing modes in reducing the marginal microleakage of two different composites in Class II cavities, where oblique and horizontal placement technique and ramp & pulse curing mode are used during restoration.
Materials and Methods
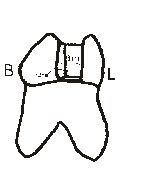
Eighty human multi-rooted teeth free of caries and restorations were collected depicted in [Table/Fig-1]. The teeth were ultrasonically cleaned and disinfected and stored in normal saline. Each specimen was mounted with the adjacent teeth for building of the proper contact. Eighty class II cavities (slot preparation) were prepared on the mesial or distal surfaces of each tooth. The final preparation showed the following dimensions: 1.5 mm mesio-distal extension, 3.0 mm buccal-lingual extension, and the gingival seat were placed at the CEJ as shown in [Table/Fig-2]. After the application of Tofflemier band and retainer (Hanenkratt, Germany) and proper wedging, mounted tooth samples were randomly divided into eight groups as shown in [Table/Fig-3].
Eighty extracted multi-rooted teeth
Diagrammatic representation of final preparation
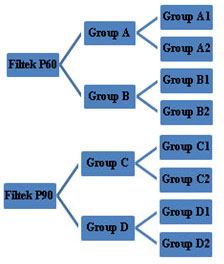
Group A and Group B were acid etched with 35% phosphoric acid for 15 sec, rinsed with water for 15 sec and excess water was removed with the help of a tissue paper, leaving a glistening hydrated surface. Then, the Adper Single Bond 2 adhesive was applied to etched enamel and dentin and light cured for 40 sec. Then the specimens were randomly divided into four groups for restoration:
Group A1 was restored with the posterior resin composite Filtek P60 (3M, ESPE) using horizontal layering technique and pulse curing mode of LED.
Group A2 was restored with the posterior resin composite Filtek P60 (3M ESPE), using horizontal layering technique and ramp curing mode of LED.
Group B1 was restored with the posterior resin composite Filtek P60 (3M ESPE), using oblique layering technique and pulse curing mode of LED.
Group B2 was restored with the posterior resin composite Filtek P60 (3M ESPE), using oblique layering technique and ramp curing mode of LED.
Group C and Group D were treated with the self-etched primer and the adhesive (P90 system adhesive) as per manufacturer’s instructions. The specimens were randomly divided into four groups for restoration:
Group C1 was restored with the posterior resin composite Filtek P90 (3M ESPE), using horizontal layering technique and pulse curing mode of LED.
Group C2 was restored with the posterior resin composite Filtek P90 (3M ESPE), using horizontal layering technique and ramp curing mode of LED.
Group D1 was restored with the posterior resin composite Filtek P90 (3M ESPE), using oblique layering technique and pulse curing mode of LED.
Group D2 was restored with the posterior resin composite Filtek P90 (3M ESPE), using oblique layering technique and ramp curing mode of LED.
Following the restorative procedures, the teeth were stored in water at 37°C for 24 h. All restorations were then finished after 24 h with fine & ultra-fine finishing disks and all specimens were thermocycled in a thermo cycling unit for 1000 cycles at 5°C and 55°C with a dwell time of 60 sec in distilled water and a five-second transfer time. Next, the open apices were sealed with cyanoacrylate adhesive and the teeth were coated with two applications of nail varnish up to 1mm from the gingival margins. All teeth were immersed in a freshly prepared aq. 2% methylene blue solution (pH 7.0) for 4 h at 37°C, then washed in water. Finally each tooth was sectioned vertically through the centre of restoration with a diamond disk. Microleakage at the gingival margin was evaluated with an optical stereomicroscope (30X magnification).
Scoring for dye penetration for marginal microleakage on the gingival wall as shown in [Table/Fig-4]:
Photographs of dye penetration scores tooth- composite interface under 30X Magnification
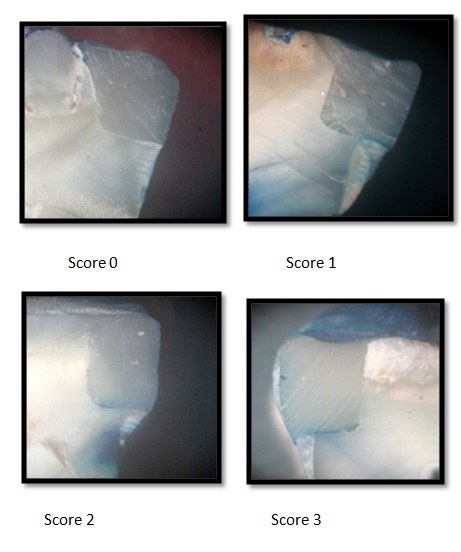
0 – No dye penetration.
1 – Dye penetration into half extension of cervical wall.
2 – Dye penetration into more than half or complete extension of the cervical wall.
3 – Dye penetration into cervical and axial walls toward the pulp [12].
Results
P90 composite when placed in the cavity with oblique incremental technique and cured with ramp mode of LED showed no microleakage, whereas P60 composite when placed in the cavity with oblique incremental technique and cured with ramp mode of LED showed highest mean microleakage of 2.00 ± 1.33. It was seen that restorations free of microleakage were hard to achieve at the gingival margin except for group D2 as shown in [Table/Fig-5]. There is significant difference between Filtek P90 and Filtek P60 (p=<0.05). There is no significant difference between Horizontal and Oblique placement technique (p=0.80). There is no significant difference between the Pulse-curing and the ramp-curing mode (p=0.62) as shown in [Table/Fig-6,7,8]. The order of microleakage can be expressed as follows- D2<C1<C2=D1<A2<A1=B1<B2 as depicted in [Table/Fig-9].
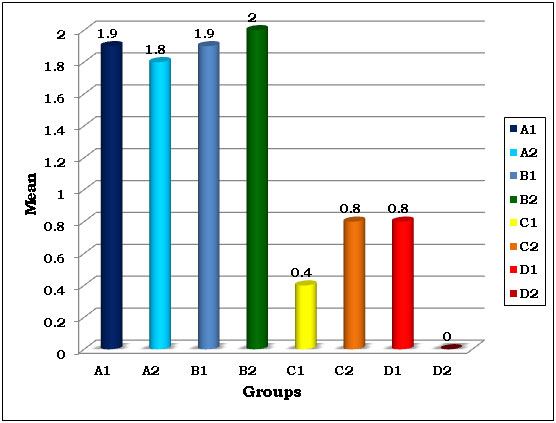
Frequency of dye penetration score as an indicator of marginal Microleakage
| SCORE |
|---|
| GROUPS | N | 0 | 1 | 2 | 3 | MEAN ± SD |
|---|
| A1 | 10 | 2 | 1 | 3 | 4 | 1.90 ± 1.20 |
| A2 | 10 | 1 | 3 | 3 | 3 | 1.80 ± 1.03 |
| B1 | 10 | 0 | 5 | 1 | 4 | 1.90 ± 0.99 |
| B2 | 10 | 2 | 2 | 0 | 6 | 2.00 ± 1.33 |
| C1 | 10 | 6 | 4 | 0 | 0 | 0.40 ± 0.52 |
| C2 | 10 | 3 | 6 | 1 | 0 | 0.80 ± 0.63 |
| D1 | 10 | 3 | 6 | 1 | 0 | 0.80 ± 0.63 |
| D2 | 10 | 10 | 0 | 0 | 0 | - |
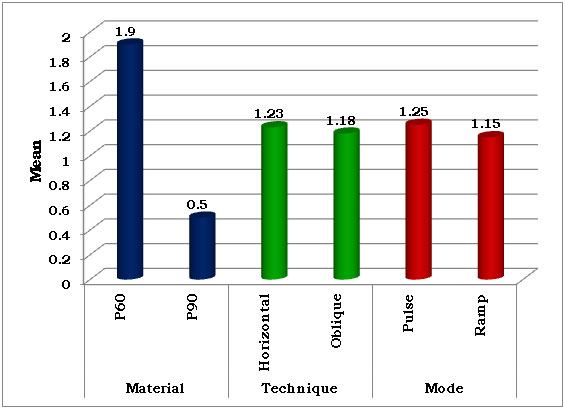
Overall comparison according to the material, placement technique & curing mode
| | Mean | Std. Error | p value |
|---|
| Material | P60 | 1.90 | 0.14 | <0.05* |
| P90 | 0.50 | 0.14 |
| Technique | Horizontal | 1.23 | 0.14 | 0.80 |
| Oblique | 1.18 | 0.14 |
| Mode | Pulse | 1.25 | 0.14 | 0.62 |
| Ramp | 1.15 | 0.14 |
(*-Statistically significant)
Comparison between various groups
| Group | A1 | A2 | B1 | B2 | C1 | C2 | D1 | D2 |
|---|
| A1 | - | 1.00 | 1.00 | 1.00 | 0.08 | 0.12 | 0.12 | <0.05* |
| A2 | - | - | 1.00 | 1.00 | 0.01* | 0.20 | 0.20 | <0.05* |
| B1 | - | - | - | 1.00 | 0.01* | 0.12 | 0.12 | <0.05* |
| B2 | - | - | - | - | 0.00* | 0.60 | 0.60 | <0.05* |
| C1 | - | - | - | - | - | 0.97 | 0.97 | 0.97 |
| C2 | - | - | - | - | - | - | 1.00 | 0.48 |
| D1 | - | - | - | - | - | - | - | 0.48 |
| D2 | - | - | - | - | - | - | - | - |
(*-Statistically significant, p<0.05)
Overall comparison according to the material, placement technique & curing mode
Mean dye penetration score as an indicator of marginal microleakage
Discussion
Restoration of deep class II cavities with the cavity margins formed of dentin, cementum or both with resin composites has always been a topic of debate. Direct class II Resin Composite restorations can be done to an acceptable standard if the gingival margin is on sound enamel. Polymerization shrinkage usually does not cause significant problem with restorations having all enamel margins, as enamel is a reliable substrate for bonding [13]. Bonding to dentin is more difficult to achieve due to the specific properties of dentin, such as tubular structure and intrinsic wetness [14]. Since the proximal boxes of many Class II restorations extend to or below the CEJ, the quality of the margin of an adhesive restoration is questionable [15,16].
Efforts have been directed to minimize the stress from polymerization shrinkage by improving placement techniques, materials and composite formulations and curing methods as it is influenced by restorative techniques, modulus of resin elasticity, polymerization rate and cavity configuration or “C-factor” [17].
Since the detrimental shrinkage stress tremendously weakens the performance and longevity of dental composites, numerous approaches have been advocated to decrease the shrinkage stress through manipulation of curing protocols and placement techniques. The use of oblique layering technique reduces the development of contraction forces between opposing walls, which could be result in stress build-up, gap formation, and cuspal fissures [18]. Hence, in this study the oblique & horizontal layering techniques were used.
In this study, the groups were restored with two different posterior resin composites i.e. Filtek P60 (3M ESPE) and Filtek P90 (3M ESPE) using two different placement techniques i.e. 1) Horizontal increments 2) Oblique increments both of not more than 2 mm thickness; and cured by two different curing modes of LED i.e. Ramp mode and Pulse mode of LED.
This study used aging by thermocycling to simulate degradation of bond over a period of time due to changes of temperature in oral cavity. Gale and Darewell [19] observed that there were wide variations in the thermocycling regimens in different studies and indicated that the choice of the regimen adopted must be arbitrary. Varying authors have used different dwell times, ranging from as low as four seconds in each bath, to as high as 180 seconds without any justification for the same. Rossomando KJ et al., [20] from his study concluded that the dwell time should be clinically relevant and recommended dwell time of 10 sec or less.
All the teeth were thermally cycled between 5°C and 55°C with a dwell time of 30 sec and a transfer time of 10 sec. Teeth were assessed for microleakage by dye penetration method using 2% methylene blue. This method has the advantage of being simple, economic and fast and is most employed method. However, the subjectivity of interpretation of the microleakage of the specimens has been noted as a shortcoming of this methodology [21].
Next, the teeth were sectioned mesio-distally into two halves using a slow-speed diamond discs. Each section was examined under an optical stereomicroscope at 30X magnification and dye penetration was scored. The results showed that the new low-shrink composite restorative material (Filtek P90) had significantly lesser microleakage after thermocycling than that of Filtek P60 composite.
These results are in similarity to the findings of results reported by, Yamazaki and Bagis [22,23] who had proved that the microleakage of silorane is lower than that of methacrylate based composite, after loading. However, the results of the present study are not in agreement with the results of Ernst [24], who concluded that the microleakage of teeth restored with silorane was similar to others restored with methacrylate composite (Tetric Ceram) with adhesive (Clearfil SE Bond). Ernst used an all-in-one (7th generation) bonding agent of silorane in his study, whereas in the present study, P90 special adhesive, which is a two bottle system bonding agent (6th generation) is used, thereby giving different results.
Light-cured composites can be cured by different means such as QTH, Plasma arc, Laser lamps and LED lamps. LED is most commonly used because they are more compatible, provide proper wavelength and emit less heat. LED has various curing modes such as Ramp, Pulse and Fast curing mode. By using the Ramp cure technique, light is initially applied at low intensity and gradually increased over time to higher intensity. In pulse curing, constant wavelength of light is applied intermittently. The reasons for these modifications of curing techniques are to reduce the polymerization stress or to cure the composite slowly by inducing the composite to flow in the gel state [25].
It was observed that there was no significant difference between Ramp cure technique and Pulse curing groups in curing the composite to minimize the marginal microleakage. This is in similarity with the findings of Alomari QD, where he concluded that there was no significant difference between the groups cured by Fast-curing, Ramp-curing, Stepped-curing and Visible-light curing in reducing the cusp deflection by reducing polymerization shrinkage stress [26], Whereas according to Theunis G. Oberholzer et al., Ramp mode significantly reduced the microleakage among all LED modes [27].
The placement of the composite material in the prepared cavity can be done by two methods, either by bulk placement or by incremental placement of the material. The incremental technique for insertion and polymerization of resin composites is advocated by many authors [28]. The reason for the lesser amount of gap formation with the incremental technique may be a result of the low configuration factor (C-factor) [29].
In this study, two different methods of incremental placement of composite (Horizontal increment and Oblique increment) were compared and the results revealed that there is no significant difference between the two methods in minimizing the microleakage.
The results of the inter-group comparison in the present study showed that except one group (D2), all other groups showed microleakage. The group of teeth restored with Filtek P90 composite and oblique technique and ramp mode (D2) showed no microleakage, whereas the group of teeth restored with Filtek P60 composite and oblique technique and ramp mode (B2) showed the maximum microleakage.
Conclusion
Within the limitations of this study, it can be concluded that in restoring deep class II cavities, the use of a low-shrink composite (Silorane) with the oblique placement technique and ramp curing mode of LED is recommended to overcome the problem of marginal microleakage.
(*-Statistically significant)
(*-Statistically significant, p<0.05)