Background
Gingival biotype is the thickness of the gingiva in the faciopalatal dimension. It has a significant impact on the outcome of the restorative, regenerative and implant therapy. It has been suggested that a direct co-relation exists with the susceptibility of gingival recession followed by any surgical procedure. So, the study was aimed to assess gingival biotype in different age groups of males and females using transgingival probing method.
Materials and Methods
Gingival thickness (GT) was evaluated in 336 patients including males and females of different age groups. The latter was based on the transparency of the periodontal probe through the gingival margin while probing the buccal sulcus. Final data collected was then used for statistical analysis.
Results
A significant difference was found between males and females with males showing thick biotype. Out of the total samples 76.9% of males showed thick biotype compared to 13.3 % of females which was statistically significant.
Conclusion
This was probably one of the few attempts to correlate gingival biotype with different age groups in males and females. A clear thick gingiva was found in more than two-third of the male subjects whereas majority of female subjects showed thin biotype. Also, it was seen that in females, the gingival biotype varies with age unlike in male.
Introduction
The term “gingival phenotype“ has been introduced to address the common clinical observation of great variation in the thickness and width of facial keratinized tissue [1,2]. Gingival biotype [3–5] is described as the thickness of the gingiva in the faciopalatal/ faciolingual dimension. Reduced gingival thickness is one of the factors that can cause periodontal attachment loss and marginal tissue recession in a patient, which is a major concern for periodontal disease progression [6].
The term periodontal biotype introduced by Seibert and Lindhe categorized the gingiva into “thick-flat“ and “thin scalloped“ biotypes [7]. Thick gingival biotype usually depicts broad zone of keratinized tissue with flat gingival contour which indicates thick underlying bony architecture and is more resilient to any inflammation or trauma. On the other side, thin gingival biotype is related with a thin band of the keratinized tissue and scalloped gingival contour which suggest thin bony architecture and is more sensitive to any inflammation or trauma [Table/Fig-1]. Inflammation of the periodontium results in increased pocket formation in thick biotype and gingival recession in thin tissues [8]. A study by Nisapakultorn et al., found that peri-implant tissue biotype was significantly associated with facial marginal mucosal level. Also, patients with a thin biotype had less papilla fill and had increased risk of peri-implant facial mucosal recession [9].
Difference between thin gingival tissue and thick gingival tissue

Gingival biotypes have been previously classified into two or three categories. Ochsenbien and Ross stated that gingival biotypes are of two types i.e. either scalloped and thin or flat and thick. They also proposed that the underlying bone depicts the contour of the gingival above [10]. Later Siebert and Lindhe categorized the gingiva into “thick - flat“ and “thin – scalloped“ biotypes [7]. A gingival thickness of ≥ 2 mm was considered as thick tissue biotype and a gingival thickness of <1.5 mm was referred as thin tissue biotype [11]. Becker et al., proposed three different periodontal biotypes: flat, scalloped and pronounced scalloped gingival [12]. Also, De Rouck et al., revisited the subject of gingival biotype and developed for simple visual inspection a new method for the classification of gingival biotype based on the following four clinical parameters: crown width/crown length ratio, gingival height, papilla height, and gingival thickness [13]. This classification is based only on a maxillary observation regardless of the mandibular parameters and the following biotypes were identified: thin scalloped, thick-scalloped, and thick-flat scalloped gingival biotype. The classification of biotype in clinical situations or research is thought to be quite subjective because a precise criterion of classification does not yet exist.
Gingival biotype can be evaluated either by direct visual assessment, by using periodontal probe or by direct measurements using endodontic spreaders, endodontic files and calipers. If the terms “thick“ and “thin“ are focused upon, only the buccopalatal measurement of gingival thickness is worth evaluating for clinical and research purposes. Various invasive and non-invasive methods were proposed to measure tissue thickness. These include direct measurement, probe transparency (TRAN) method, ultrasonic devices, and cone-beam computed tomography (CBCT) scan [11,14–24].
The use of ultrasonic devices to determine thickness is a non-invasive method which has been proved to be reproducible [15], drawbacks include difficulties in maintaining the directionality of the transducer [19], unavailability of the device [25] and high costs. These factors may be responsible for the fact that the device has not become part of the standard armamentarium of the clinician. A simpler method has been proposed to discriminate thin from thick gingiva based on the transparency of the periodontal probe through the gingival margin [20].
Recently cone-beam computed tomography scan (CBCT) is being used as advanced diagnostic aid in measuring thickness of hard as well as soft tissues [24]. Fu et al., stated that CBCT provides accurate measurements of both bone and labial soft tissue thickness. He concluded that CBCT measurements might be a more objective method to define the thickness of both soft and hard tissues than direct measurements [26].
Interestingly, studies on humans [25] and dogs [27] have shown that the gingival thickness varies according to the dental arch, gender, and age. Therefore, objective of this study was to assess the gingival biotype between different sex and age groups of a given population using visual transgingival probing method.
Materials and Methods
Subjects
A total of 336 systemically healthy individuals (186 males and 150 females) of different age groups ranging from 20 years to 70 years of age who came to the out-patient Department of Periodontology and Implantology, Institute of Dental Sciences, Bareilly, UP, India from February 2014 to September 2014, were randomly selected for the study. After obtaining the ethical board clearance, the subjects were provided with an informed consent for participating in the present study. All subjects were then provided with oral hygiene instructions preceded by oral prophylaxis, if necessary. Biotype was then measured immediately after screening in healthy individuals and was followed by scaling in patients having extrinsic stains.
The inclusion criteria were as follows:
1. Subjects presenting all maxillary incisors;
2. Subjects having good oral hygiene without any clinical signs of gingival inflammation or attachment loss (periodontal probing does not exceed 3mm).
The exclusion criteria were as follows:
1. Patients having pockets exceeding 3 mm or giving any past history of periodontitis.
2. Pregnant or lactating women;
3. Subjects taking medication with any known effect on periodontal soft tissues.
Clinical Evaluation
The gingival biotype for each of the subjects was determined by two examiners. No gingival index was used for this study. The study was based on criteria followed by various other authors where no gingival index was used [3,13,28]. The evaluation of gingival biotype was based on the transparency of periodontal probe. Measurements were made with a calibrated and standardized periodontal probe (UNC-15, Hufriedy) through the gingival margin while probing the sulcus at the midfacial aspect of both central maxillary incisors (Kan et al.,) [20]. If the outline of the underlying periodontal probe could be seen through the gingival, it was categorized as thin (score: 0); if not, it was categorized as thick (score: 1) [Table/Fig-2].
Transgingival probing method. Periodontal probing through midfacial region of maxillary central incisors

This resulted in three possible scores on a patient level [13]:
0 (both central incisors with score 0),
1 (one central incisors with score 1) or
2 (both central incisors with score 1)
After obtaining the data from the patients, suitable statistical analyses were performed such as chi-square test. The data was analysed according to different sex groups, age groups and together.
Results
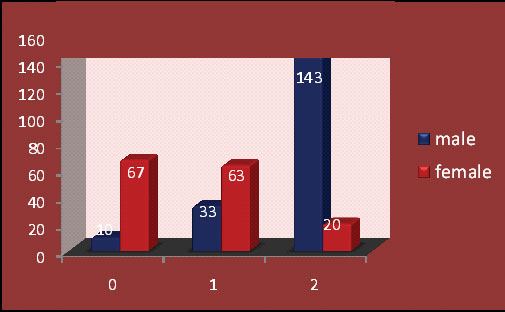
The study population consisted of 336 periodontal healthy individuals which included 186 males and 150 females, with age group ranging from 15 years to 75 years. Large group of age range was included in this study to determine the gingival biotype in different age groups. In older age, majority of patients have chronic periodontitis therefore patients with healthy periodontium were only examined. The study showed majority of healthy periodontium in age group below 50, after 50 years of age sample size reduced because rarely patients were seen with healthy periodontium. But still to know the type of biotype present in later ages, older age group was included in the study. Majority of the age groups was in between 20-30 years. Gingival biotype compared between males and females was statistically significant. The thick biotype are more prevalent in males that is 76.9% males showed thick biotype compared to thin biotype which is seen only in 5.4% males. Contrary to this, female population which showed 44.7% having thin biotype and only 13.3% thick biotype which was highly statistical significant [Table/Fig-3].
GINGIVAL BIOTYPE in Male & Female with percentage
| CODE | M | F | TOTAL | F(%) | M(%) | p-value |
|---|
| 0 | 10 | 67 | 77 | 44.7 | 5.4 | p<0.05 significant |
| 1 | 33 | 63 | 96 | 42.0 | 17.7 | p<0.05 significant |
| 2 | 143 | 20 | 163 | 13.3 | 76.9 | p<0.05 significant |
| TOTAL | 186 | 150 | 336 | | | |
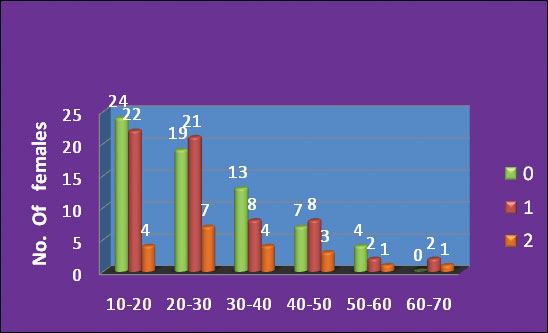
When the gingival biotype was compared among the age groups, in males thick biotype was maximum in 20-30 years of age and minimum in 60-70 years of age [Table/Fig-4]. Among the female subjects there was no significant age group showing thin biotype, it was evenly distributed among all age group [Table/Fig-5,6]. Among all age groups of males, thick biotype was statistically significant in all age groups whereas in females, thin biotype varied from age to age [Table/Fig-5].
Frequency age group wise distribution of gingival biotype in males
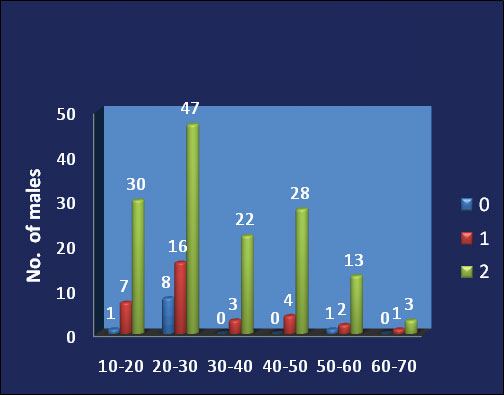
Age Group wise GINGIVAL BIOTYPE in Male & Female
| AGE | MALE | FEMALE |
|---|
| 0 | 1 | 2 | 0 | 1 | 2 |
|---|
| 10-20 | 1 | 7 | 30 | 24 | 22 | 4 |
| 20-30 | 8 | 16 | 47 | 19 | 21 | 7 |
| 30-40 | 0 | 3 | 22 | 13 | 8 | 4 |
| 40-50 | 0 | 4 | 28 | 7 | 8 | 3 |
| 50-60 | 1 | 2 | 13 | 4 | 2 | 1 |
| 60-70 | 0 | 1 | 3 | 0 | 2 | 1 |
| TOTAL | 10 | 33 | 143 | 67 | 63 | 20 |
Frequency age group wise distribution of gingival biotype in females
Discussion
Tissue biotype is one of the critical factors that determine the result of dental treatment. Initial gingival thickness predicts the outcome of any root coverage procedures or any restorative treatments [16,29]. It has been documented that patients with thin gingival biotype were more likely to experience gingival recession following nonsurgical periodontal therapy. Mucogingival problems may result from orthodontic movement of teeth away from the alveolar process, particularly among patients with thin periodontium. The thicker biotype prevents mucosal recession, hides the restorative margins and camouflages the titanium implant shadows. It also prevents biological seal around implants, thus reducing the crestal bone resorption. The level of gingival thickness before regenerative surgery was found to be a predicting factor for further recession. However in thin biotype, the periodontal surgical procedures can enhance the quality of tissue resulting in a more favourable treatment outcome [30].
Patients with thick and flat gingival biotypes exhibit short papillae whereas thin and scalloped biotypes represent long papillae. This morphometric difference may be the cause of more papilla loss in the thin biotype. Thick biotypes include flat soft tissue and bony architecture, denser and more fibrotic soft tissue with large amount of attached masticatory mucosa, it is more resistant to any acute trauma and respond to disease by pocket formation and infra bony defect. The gingival thickness affects the treatment outcome possibly because of the difference in the amount of blood supply to the underlying bone and susceptibility to resorption. Gingival or periodontal diseases are more likely to occur in patients with a thin biotype and the remodelling process, after tooth extraction results in more dramatic alveolar resorption in the apical and lingual directions. Therefore, special care must be taken when treatment planning is done for the cases of thin gingival biotype and if required should be followed by surgical procedure that enhances gingival thickness. Also, thin biotype in female patients might be one of the probable risk factor for high prevalence of chronic periodontitis in females.
The ability of the gingival tissue to cover any underlying material is essential for attaining aesthetic results, especially in cases of implant, regenerative and restorative dentistry, where subgingival metal restorations are mainly used. In this study, the metal periodontal probe was used in the sulcus to evaluate gingival tissue thickness because it seems to be a reliable, objective, economical and minimally invasive method since periodontal probing procedures are routinely performed during any aesthetic, restorative, periodontal, and implant treatments. A study done by Kan et al., compared various methods for assessing gingival biotype and reported no statistically significant difference on comparing the periodontal probe assessment and the tension-free calliper [3]. Use of Cone beam computerized tomography (CBCT) is superior in diagnosing but this procedure requires technical expertise and is expensive as well with higher radiographic exposure to the patient. Hence, a simple method like periodontal probing can help the clinician with the better treatment planning and definitive treatment outcome in routine practise.
In the present study gingival biotype presented a significant difference between male and female subjects [Table/Fig-7]. These results are in accordance with study done by Muller et al., [2] and Vandana et al., [25] reporting a generalized thinner masticatory mucosa for females. De Rouck et al., in his study also stated a significant difference between male and female subjects. He concluded that 84% of all measured central incisors of male participants showed thick biotype compared to females participants [13].
Frequency distribution of gingival biotype in males and females
This study suggested that in majority of the population, the thick periodontal biotype was more prevalent than the thin scalloped form. Olsson and Lindhe in their study stated that in 85% of the population, the thick periodontal biotype was more prevalent than the thin scalloped form (15%) [31]. Anu Kuriakose and Saranyan Rajuin evaluated the thickness of palatal masticatory mucosa in Indian subjects between 17 to 49 years of age, using ‘bone-sounding” (transgingival probing) technique and concluded that the younger age group had significantly thinner masticatory mucosa than the older age group. They also stated that females have thinner mucosa compared to males, but the difference was not statistically significant [32]. Also, Kolliyavar et al., reported the same findings in his study [33]. On contrary, Vandana and Savitha studied the thickness of the gingiva in association with age and found the gingiva to be thicker in the younger age group than in the older [25]. Kolte et al., also observed the same i.e. the younger age group having significantly thicker gingiva but less width than that of the older age group and the gingiva was found to be thinner and with less width in females compared to males [34]. According to a survey conducted by Bhat et al., the thicker biotype is more prevalent in male population whereas the female population consists of thin and scalloped biotype. The thick flat biotype was mainly associated with younger individuals while older age group showed thin scalloped gingival biotype [28]. The probable reason for this may be change in oral epithelium caused by age related thinning of the epithelium and diminished keratinization. Also with age, the interdental papilla recedes which may lead to greater frequency of thin biotype in older age group. Warasswapati et al., [35] explained that racial and genetic factors may also have a significant impact on biotype.
Thick periodontal biotypes are usually related with good periodontal health as tissue is dense and fibrotic with a large zone of attached gingiva. Also, surgical evaluation of the thick biotype reveals thicker as well as flatter underlying osseous bone [26].
The aetiology and pathogenesis of periodontal disease followed by destruction to the tissue may be depends on gingival biotype. The gender prediction of the progression of periodontal disease may be because of the thin gingival biotype in females.Various limitations of the study was the sample size which was not enough and thus further studies with larger sample size should be conducted. Also, study just included the Bareilly population but to determine generalized universal biotype in healthy individuals, further multicentric studies with larger sample sizes are required to substantiate the findings.
Conclusion
A precise and careful examination of the gingival biotype is necessary for appropriate treatment planning and monitoring the patient treatment outcome.This was probably one of the few attempts to correlate gingival biotype with different age groups in males and females. A thin gingival biotype was found in about 44.7% female subjects and a clear thick in 76.9% male subjects. Also, it showed that in females, the gingival biotype varies with age unlike in male.
[1]. Muller HP, Eger T, Gingival phenotypes in young male adultsJ Clin Periodontol 1997 24:65-71. [Google Scholar]
[2]. Muller HP, Heinecke A, Schaller N, Eger T, Masticatory mucosa in subjects with different periodontal phenotypesJ Clin Periodontol 2000 27:621-26. [Google Scholar]
[3]. Kan JY, Morimoto T, Rungcharassaeng K, Roe P, Smith DH, Gingival biotype assessment in the aesthetic zone: Visual versus direct measurementInt J Periodontics Restorative Dent 2010 30:237-43. [Google Scholar]
[4]. Kois JC, Predictable single-tooth peri-implant aesthetics: Five diagnostic keysCompend Contin Educ Dent 2004 25:895-96. [Google Scholar]
[5]. Kao RT, Fagan MC, Conte GJ, Thick vs. thin gingival biotypes: A key determinant in treatment planning for dental implantsJ Calif Dent Assoc 2008 36:193-98. [Google Scholar]
[6]. Januario AL, Barriviera M, Duarte WR, Soft tissue cone-beam computed tomography: a novel method for the measurement of gingival tissue and the dimensions of the dentogingival unitJ Esthet Restor Dent 2008 20:366-74. [Google Scholar]
[7]. Seibert JL, Lindhe J, Aesthetics and periodontal therapy. In: Lindhe J, edTextbook of Clinical Periodontology 1989 2nd edCopenhangen, DenmarkMunksgaard:477-514. [Google Scholar]
[8]. Kao RT, Fagan MC, Conte GJ, Thick vs. thin gingival biotypes: a key determinant in treatment planning for dental implantsJournal of the California Dental Association 2008 36:193-98. [Google Scholar]
[9]. Nisapakultorn K, Suphanantachat S, Silkosessak O, Ratanamongkolgul S, Factors affecting soft tissue level around anterior maxillary single tooth implantsClin oral implants res 2010 21:662-70. [Google Scholar]
[10]. Ochsenbein C, Ross S, A re-evaluation of osseous surgeryDent Clin North Am 1969 13(1):87-102. [Google Scholar]
[11]. Claffey N, Shanley D, Relationship of gingival thickness and bleeding to loss of probing attachment in shallow sites following non surgical periodontal therapyJ Clin Periodontol 1986 13:654-57. [Google Scholar]
[12]. Becker W, Ochsenbien C, Tibbetts L, Becker BE, Alveolar bone anatomic profiles as measured from dry skulls Clinical ramificationsJ Clin Periodontol 1997 24:727-31. [Google Scholar]
[13]. De Rouck T, Eghbali R, Collys K, De Bruyn H, Cosyn J, The gingival biotype revisited: Transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingivalJ Clin Periodontol 2009 36:428-33. [Google Scholar]
[14]. Olsson M, Lindhe J, Marinello CP, On the relationship between crown form and clinical features of the gingiva in adolescentsJ Clin Periodontol 1993 20(8):570-77. [Google Scholar]
[15]. Eger T, Muller HP, Heinecke A, Ultrasonic determination of gingival thickness. Subject variation and influence of tooth type and clinical featuresJ Clin Periodontol 1996 23(9):839-45. [Google Scholar]
[16]. Baldi C, Pini-Prato G, Nieri M, Coronally advanced flap procedure for root coverage Is flap thickness a relevant predictor to achieve root coverage? A 19- case seriesJ Periodontol 1999 70:1077-84. [Google Scholar]
[17]. Goaslind GD, Robertson PB, Mahan CJ, Morrison WW, Olson JV, Thickness of facial gingivaJ Periodontol 1977 48(12):768-71. [Google Scholar]
[18]. Studer SP, Allen EP, Rees TC, Kouba A, The thickness of masticatory mucosa in the human hard palate and tuberosity as potential donor sites for ridge augmentation proceduresJ Periodontol 1997 68(2):145-51. [Google Scholar]
[19]. Daly CH, Wheeler JB, The use of ultrasonic thickness measurement in the clinical evaluation of the oral soft tissuesInt Dent J 1971 21(4):418-29. [Google Scholar]
[20]. Kan JY, Rungcharassaeng K, Umezu K, Kois JC, Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humansJ Periodontol 2003 74(4):557-62. [Google Scholar]
[21]. Kydd WL, Daly CH, Wheeler JB, The thickness measurement of masticatory mucosa in vivoInt Dent J 1971 21(4):430-41. [Google Scholar]
[22]. Terakura T, Non-invasive measurement of the thickness of oral soft tissuesJ Jpn Prosthodont Soc 1986 30(6):1402-11. [Google Scholar]
[23]. Lawson RB, Jones ML, An evaluation of a noninvasive method of assessing alveolar bone levels in an experimental model of cleft lip and palateCleft Palate Craniofac J 1998 35(1):1-8. [Google Scholar]
[24]. Barriviera M, Duarte WR, Januario AL, Faber J, Bezerra AC, A new method to assess and measure palatal masticatory mucosa by cone-beam computerized tomographyJ Clin Periodontol 2009 36(7):564-68. [Google Scholar]
[25]. Vandana KL, Savitha B, Thickness of gingival in association with age, gender and dental arch locationJ Clin Periodontol 2005 32:828-30. [Google Scholar]
[26]. Fu JH, Yeh CY, Chan HL, Tissue biotype & its relation to the underlying bone morphologyJ. Periodontal 2010 81:569-74. [Google Scholar]
[27]. Kyllar M, Witter K, Gingival thickness in dogs: Association with age, gender, and dental arch locationJ Vet Dent 2008 25:106-09. [Google Scholar]
[28]. Bhat V, Shetty S, Prevalence of different gingival biotypes in individuals with varying forms of maxillary central incisors:A survey Journal of Dental Implants 2013 3(2):116-21. [Google Scholar]
[29]. Hwang D, Wang HL, Flap thickness as a predictor of root coverage: A systematic reviewJ Periodontol 2006 77:1625-34. [Google Scholar]
[30]. Anderegg CR, Metzler DG, Nicoll BK, Gingival thickness in guided tissue regeneration and associated recession at furcation defectsJ Periodontol 1995 66:197-402. [Google Scholar]
[31]. Olsson M, Lindhe J, Periodontal Characteristics in individuals with varying form of the upper central incisorsJ Clin Periodontol 1991 18:78-82. [Google Scholar]
[32]. Kuriakose A, Raju S, Assessment of thickness of palatal mucosal donor site and its association with age and genderJournal of Indian Society of Periodontology 2012 16(3):370-74. [Google Scholar]
[33]. Kolliyavar B, Setty S, Thakur SL, Determination of thickness of palatal mucosaJournal of Indian Society of Periodontology 2012 16(1):80-83. [Google Scholar]
[34]. Kolte R, Kolte A, Mahajan A, Assessment of gingival thickness with regards to age, gender and arch locationJournal of Indian Society of Periodontology 2014 18(4):478-81. [Google Scholar]
[35]. Wara–aswapati N, Pitiphat W, Chandrapho N, Rattanayatikul C, Karimbux N, The thickness of palatal masticatory mucosa associated with ageJ Periodontol 2001 72:1407-12. [Google Scholar]