Palmaris longus, phylogenetically a retrogressive muscle, exhibits significant anatomical variations compared to other muscles of the upper extremity. It is of great surgical importance because, it is the first option tendon for graft procedures in various cosmetic, plastic and reconstructive surgeries. It has also been widely used in various tendon transfer procedures in treating facial paralysis, ptosis correction, lip augmentation and digital pulley reconstruction. We report a rare variant pattern of Palmaris longus with duplicated tendons and with multiple insertions to thenar and hypothenar muscles, fasciae and the flexor retinaculum along with its normal continuation as palmar aponeurosis. Variations in its insertions not only contribute, but also augment the various pathological processes such as Dupuytren’s contracture, Carpal tunnel and Guyon’s syndromes. So it is of utmost importance for surgeons, physicians and radiologists, to be aware of these variations, well in advance.
Case Report
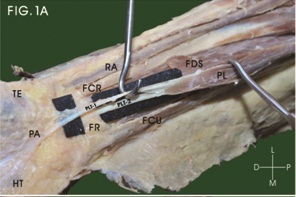
During routine anatomical dissection, we encountered a unilateral variation in the insertion of Palmaris longus tendon on the right upper limb of an 82-year-old formalin embalmed, male cadaver. The fusiform muscle belly of Palmaris longus with dimensions 17.5×1.5×0.95 cm, proximally originated from medial epicondyle of the humerus, along with the other superficial flexor muscles of forearm. The muscle belly prolonged downwards into two separate well-formed flattened tendons at the middle of the forearm, 9 cm proximal from wrist, ran towards the wrist covering flexor digitorum superficialis and median nerve, on the medial side of flexor carpi radialis tendon [Table/Fig-1a]. The superficial tendon was thicker, size 10.5×0.75 cm, passed over the flexor retinaculum, and at the distal half of the retinaculum, it is divided into three slips. The central slip, thick, broad and shiny, appeared to be the main continuation, merged with apex of the flattened palmar aponeurosis. The lateral collateral slip, thicker and stronger, was fused with the deep fascia covering abductor and flexor pollicis brevis muscles and contained few muscle fibres of origin of these muscles. The medial collateral slip, relatively small and thin, merged with deep fascia covering abductor and flexor digiti minimi [Table/Fig-1b]. The deep tendon was relatively thin, size 9.5×0.5 cm, passed deep to flexor retinaculum and faned out to merge with transverse tendinous fibres of flexor retinaculum [Table/Fig-1c]. The Palmaris longus tendon on the left side of forearm was normal as in textbook morphology.
Dissection of right forearm showing the dual tendons of Palmaris Longus
PL - Palmaris longus; PLT-1 - Superficial tendon of Palmaris longus; PLT-2 -Deep tendon of Palmaris longus; PA - Palmar aponeurosis; FR - Flexor retinaculum; FDS - Flexor digitorum superficialis; FCR - Flexor carpi radialis; FCU - Flexor carpi ulnaris; RA - Radial artery; TE - Thenar muscles; HT - Hypothenar muscles
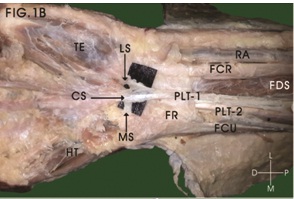
Dissection of front of right wrist showing three slips of insertion of superficial tendon of Palmaris Longus into palmar aponeurosis, thenar and hypothenar eminences
PLT-1 - Superficial tendon of Palmaris longus; MS - Medial slip; CS - Central slip; LS - Lateral slip; PLT-2 - Deep tendon of Palmaris longus; FR - Flexor retinaculum; FDS - Flexor digitorum superficialis; FCR - Flexor carpi radialis; FCU - Flexor carpi ulnaris; RA - Radial artery; TE - Thenar muscles; HT - Hypothenar muscles
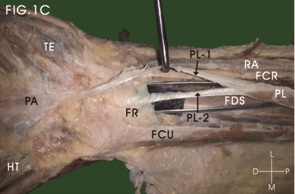
Dissection of front of right wrist showing insertion of deep tendon of Palmaris Longus into flexor retinaculum
PL - Palmaris longus; PL-1 - Superficial tendon of Palmaris longus; PL-2 - Deep tendon of Palmaris longus; PA - Palmar aponeurosis; FR - Flexor retinaculum;FDS - Flexor digitorum superficialis; FCR - Flexor carpi radialis; FCU - Flexor carpi ulnaris; RA - Radial artery; TE - Thenar muscles; HT - Hypothenar muscles
Discussion
Palmaris longus, a superficial flexor of the forearm, arises from medial epicondyle of humerus by the common flexor origin, from adjacent intermuscular septum, and also from antebrachial fascia. The slender, fusiform belly converges into a long flattened tendon in the middle of the forearm, runs on the medial side of flexor carpi radialis, crosses the wrist superficial to flexor retinaculum, and terminates into a flat palmar aponeurosis. A few fibres interweave with the transverse fibres of the flexor retinaculum. It is supplied by median nerve of brachial plexus through C7 and C8 segments of spinal cord.It is a week flexor of metacarpo-phalangeal and carpo-metacarpal joints, but mainly anchor the skin and fascia of the hand and in resisting the horizontal shearing forces in distal direction, as in holding a golf club [1]. The most frequent variations include complete absence in one or both sides; anomalies in the form and location of its fleshy part viz. - reversed, centrally placed, triple headed reversed, digastrics, hypertrophied and completely muscular; duplicated, bifid or bitendinous, epifascial accessory; aberrant insertions into the neighboring structures namely, tendons, fasciae, ligaments and bones and accessory tendinous slips to any of these structures [2]. These variations assume clinical importance because they may cause or aggravate the symptoms of compartment syndromes of the forearm and wrist leading to Volkmann’s ischaemic contracture, Carpal tunnel syndrome, Guyon’s syndrome and Dupuytren’s contracture. They may also cause difficulties in image interpretation by radiologists [3]. Palmaris longus tendon assumes great surgical importance, since it is the first option in tendon graft procedures in various cosmetic, plastic and reconstructive surgeries, due to its superficial position, vestigial without much functional impairment. It is also utilized in tendon transfer procedures in treating facial paralysis, ptosis correction, lip augmentation, digital pulley reconstruction and various other nerve palsies [4]. So, it is of utmost importance for surgeons, physicians, radiologists and physiotherapists to be aware of the possibility of these variations. The purpose of the present case report is a detailed description of anomalous insertions of Palmaris longus and its adverse clinical impact.
The forearm flexors develop from a mesodermal condensation of dorsolateral cells of somites that migrate into the limb bud during 7th week of embryonic development. These mesenchymal cells, form the flexor mass, which subsequently undergoes division into two layers - superficial and deep. The deep layer gives rise to the flexor digitorum superficialis, flexor digitorum profundus and flexor pollicis longus. The superficial layer of flexor mass goes to form pronator teres, flexor carpi radialis, palmaris longus and flexor carpi ulnaris [5,6]. The presence of an additional cleavage in the superficial forearm flexor mass during development leads to an additional tendon of Palmaris longus, which gains insertion to flexor retinaculum, interweaving with the transverse fibres of retinaculum and strengthen the carpal tunnel.
Palmaris longus is well known for its variations; being phylogenetically a retrogressive muscle, its absence in the human body is quite common. On searching the evolutionary history among vertebrates, the Palmaris longus was well developed in mammals, where the forelimbs were used for ambulation and weight bearing. Among the primates it is found in the lower groups, viz. - urangutan, but invariably absent in the higher apes viz. - chimpanzee, gibbon and gorilla. Among the predators, including cats, the Palmaris longus retracts the claws, thereby aiding in catching their prey [4,7]. As the evolution proceeds, the forelimbs become a prehensile organ, the function of palmaris longus has been taken over by the intrinsic muscles of hand, so it is partly degenerated and replaced by a flattened fibroaponeurotic palmar aponeurosis. With acquirement of the bipedal gait, the Palmaris longus underwent further degeneration with a small belly and a long tendon, thereby aids only in augumentation of grip with accessory flexion in the wrist and metacarpophalangeal joints.Morphogenetically the development of palmaris longus was regulated by a HOX gene [7].
Reihmann et al., conducted an extensive research on 1600 upper extremities and classified the variations of the palmaris longus muscle [8]. The palmaris longus was absent in 2.8 - 26% of individuals, largest being in American whites and Turks, with incidence of 12.8%, while Africans, Asians, and Mongoloids being the least with 3.4%. Agenesis of palmaris longus was more often seen in left forearm than on the right, higher in females than males and has been attributed to Mendelian characteristics, but its genetic transmission is not clear [2,9,10]. The wide variations in the reported data of agenesis may be attributed mainly to different methods of analysis viz., ranging from gross dissections to mere visual and palpatory techniques and other non-invasive techniques. So we advise a thorough check up of presence of palmaris longus tendon clinically, before proceeding on to harvesting the grafts.
Variations and anomalies of the palmaris longus at its origin, course and insertions were seen in 7 to 10% of the subjects studied [2,9,10]. Variations in form ranging from short, fusiform, proximal belly, taper into a long tendon, completely muscular from origin to insertion or to a limited fibrous vestigial remnant. The muscle belly may be centrally or distally displaced or doubled forming a digastric muscle. Sometimes the muscle belly or tendons may be bifid or split on itself [2,8]. According to Paraskevas et al., the incidence of duplication of palmaris longus vary between 0.8-3.1% [11]. Variations in attachments occur rarely with an incidence of 0.5% [2]. They may be seen in origin or insertion, but the insertion of the muscle is highly variable. Variations in the insertions include the antebrachial, thenar and hypothenar fasciae, various carpal bones like pisiform, scaphoid, various muscles viz. - thenar, hypothenar muscles, flexor carpi ulnaris and to one of the long flexor tendons, transverse carpal ligament and the interosseous membrane. The tendon may be bifid distally with an additional slip inserting into any of the above structures [8].
In this case report, we presented a rare variant in the insertion of Palmaris longus tendon on the right forearm. The fusiform muscle belly terminates into two separate well-formed flattened tendons, at the middle of the forearm, crosses the wrist superficial to flexor digitorum superficialis and median nerve, along the inner side of flexor carpi radialis tendon. The thicker superficial tendon passes over the flexor retinaculum, and is divided into three slips. The thick, shiny central slip appears to be the main component, merged with the apex of the palmar aponeurosis. The strong lateral collateral slip, being aponeurotic, is fused with the thenar fascia and gives origin to few fibres of abductor and flexor pollicis brevis muscles. The smaller medial collateral slip is merged with fascia covering the hypothenar muscles. The deep tendon passes deep to the flexor retinaculum, splits and merges with the transverse tendinous fibres of flexor retinaculum and reinforces the carpal tunnel. Thus the palmaris longus tendons through its extended insertions into thenar, hypothenar muscles and to the carpal tunnel also take part in the abduction and flexion of thumb and little finger and strengthen the carpal tunnel, in addition to flexion of wrist and metacarpopahalangeal joints and in the augmentation of grip.
Anomalous insertions of palmaris longus tendon deep into the flexor retinaculum exert pressure on median nerve in the proximal part of carpal tunnel leads to carpal tunnel like syndrome. This may sometimes leads to a reduction in the muscular power of the hand, pain and numbness in the territory of median nerve in the hand and ape-thumb like deformity. Palmaris longus with additional slips of insertion to hypothenar muscles and fascia may compress ulnar nerve and vessels in Guyon’s canal leading to syndromes mimicking claw hand and compartment syndromes leading to Volkmann’s ischaemic contracture [12]. Anomalous insertions of palmaris longus through multiple tendinous slips to thenar and hypothenar eminences may aggravate, modify and hasten the signs and symptoms of Dupuytren’s contracture affecting forearm and hand. Mechanic who performs repetitive work tasks with palmaris longus anomalies may end up with effort related pain at wrist due to median nerve compression [4]. So patient complains of wrist pain with swelling at volar wrist should be suspected for anomalies in palmaris longus tendons. Anomalous palmaris longus insertions may also cause difficulties in the interpretation of local radiological images by radiologists. It may also cause difficulties in the electromyographical studies of the median nerve at the wrist and in the endoscopic wrist procedures [4]. A detailed knowledge of anomalies of palmaris longus is useful for orthopaedic and plastic surgeons during the differential diagnosis of tumour or ganglion on MRI or clinical examination [2]. In clinical practice, an aberrant palmaris longus could be incidentally found during clinical examination without provoking clinical symptoms and may simulate a soft tissue tumour [13].
Palmaris longus tendon assumes great surgical importance, since it is the first option in tendon graft procedures in various cosmetic, plastic and reconstructive surgeries. It is because that it fulfills the necessary criteria of length, width, easy surgical availability and readily detected in vitro, over other tendons, which makes harvesting easier than its counterpart the plantaris muscle in the leg [12,14]. Because of its superficial position and vestigial form without much functional impairment, it is widely used as a donor tendon in tendon grafts procedures for long flexor and extensor tendons defect of fingers. It can also be utilized in tendon transfer procedures in treating facial paralysis, ptosis correction, lip augmentation, digital pulley reconstruction, ligament reconstructions, blepharoptosis and in various other nerve palsies [6]. Alshaham et al., suggested that ‘V’ shaped split tendon of palmaris longus in some subjects may be utilized as a potential source to provide ‘V’-shape splint in selected reconstructive protocols like, oral and lid angle in facial palsy [14]. So therefore it is of utmost importance for surgeons, physicians, radiologists and physiotherapists to be aware of this possibility of these variations. Also, a thorough knowledge of variations in the insertions of palmaris longus tendon may be of immense help to the surgeons in planning their surgeries well in advance.
Conclusion
Palmaris longus is functionally insignificant in human beings, but its utility in various reconstructive surgeries is a proven fact beyond doubt. Aberrancy in its insertions not only contribute, but also augment the various pathological process, thus makes a challenging job for the surgeons during various surgical procedures. In the present case, the palmaris longus tendon splits to gain aberrant insertions to thenar, hypothenar muscles and fascia and to the flexor retinaculum in addition to its normal continuation as palmar aponeurosis, thereby complicating its action. So, we advise that all hand surgeons should be aware of these anatomical variations during various surgical procedures, before attempting to explore the palmaris longus tendon.
[1]. Ellis H, Healy JC, Johnson D, Williams A, Forearm. In: Standring S. Edinburg, editorGray’s Anatomy: The Anatomical Basis of Clinical Practice 2005 39th EdPhiladelphiaElsevier Churchill Livingstone:873-87. [Google Scholar]
[2]. Natsis K, Didagelos M, Manoli SM, Vlasis K, Papathanasiou E, Sofidis G, Fleshy palmaris longus muscle - a cadaveric finding and its clinical significance: a case reportHippokratia 2012 16(4):378-80. [Google Scholar]
[3]. Park MJ, Namdari S, Yao J, Anatomic Variations of the Palmaris Longus MuscleAm J Orthop 2010 39:89-94. [Google Scholar]
[4]. Vedpathak S, Belsare S, Palmaris longus– An overviewEjournal.mitmimer.com/issue5/palmarispdf [Google Scholar]
[5]. Bergman RA, Thompson SA, Afifi AK, Saadeh FA, Illustrated encyclopedia of human anatomic variation: Opus I: Muscular system: Alphabetical listing of muscles: P:palmaris longusBaltimore, Munich, Urban and Schwarzenberg 1988 1:12-3. [Google Scholar]
[6]. Patel RN, Sharma B, Gupta UK, Duplication of palmaris longus muscle: a case reportIndian Journal of Basic and Applied Medical Research 2014 3(3):247-50. [Google Scholar]
[7]. Angelini Junior LC, Angelini FB, de Oliveira BC, Soares SA, Angelini LC, Cabral RH, Use of the tendon of the palmaris longus muscle in surgical procedures: study on cadaversActa ortop. Bras 2012 20(4):226-29. [Google Scholar]
[8]. Reimann A, Daseler F, Anson B, Beaton L, The Palmaris longus muscle and tendon. A study of 1600 extremitiesAnat Rec 1944 89:497-505. [Google Scholar]
[9]. Pai MM, Prabhu LV, Nayak SR, Madhyastha S, Vadgaonkar R, Krishnamurthy A, The palmaris longus muscle: its anatomic variations and functional morphologyRom J Morph Embryo 2008 49(2):215-17. [Google Scholar]
[10]. Thompson NW, Mockford BJ, Cran GW, Absence of the palmaris longus muscle: a population studyUlster Med J 2001 70(1):22-24. [Google Scholar]
[11]. Paraskevas G, Tzaveas A, Natsis K, Kitsoulis P, Spyridakis I, Failure of palmaris longus muscle duplication and its clinical applicationFolia Morphol (Warsz) 2008 67(2):150-53. [Google Scholar]
[12]. Acikel C, Ulkur E, Karagoz H, Celikoz B, Effort-related compression of median and ulnar nerves as a result of reversed three headed and hypertrophied palmaris longus muscle with extension of Guyon’s canalScan J PlastReconstrSurg Hand Surg 2007 41:45-47. [Google Scholar]
[13]. Turner MS, Caird DM, Anomalous muscles and ulnar nerve compression at the wristHand 1977 9:140-42. [Google Scholar]
[14]. Alshaham AA, Mular P, Jawad K, Anomalous V-shape palmaris longus tendon: two casesJournal of Medical Cases 2010 1(2):68-70. [Google Scholar]