Transient 2nd Degree Av Block Mobitz Type II: A Rare Finding in Dengue Haemorrhagic Fever
Ashwini Kumar Nigam1, Omkar Singh2, Ayush Agarwal3, Amit K Singh4, Subhash Yadav5
1 Associate Professor, Department of Medicine, S N Medical College Agra, Uttar Pradesh, India.
2 Junior Resident, Department of Medicine, S N MedicineAgra, Uttar Pradesh, India.
3 Junior Resident, Department of Medicine, S N MedicineAgra, Uttar Pradesh, India.
4 Junior Resident, Department of Medicine, S N MedicineAgra, Uttar Pradesh, India.
5 Lecturer, Department of Medicine, S N Medical CollegeAgra, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Omkar Singh, 424 Saptrishi Apartments Sector 16 B Awas Vikas Colony Agra-282008, Uttar Pradesh, India. E-mail : Dr.omkar.singh@gmail.com
Dengue has been a major problem as endemic occurs almost every year and causes a state of panic due to lack of proper diagnostic methods and facilities for proper management. Patients presenting with classical symptoms are easy to diagnose, however as a large number of cases occur every year, a number of cases diagnosed with dengue fever on occasion presents with atypical manifestations, which cause extensive evaluation of the patients, unnecessary referral to higher centre irrespective of the severity and therefore a rough idea of these manifestations must be present in the backdrop in order to prevent these problems. Involvement of cardiovascular system in dengue has been reported in previous studies, and they are usually benign and self-limited. The importance of study of conduction abnormalities is important as sometimes conduction blocks are the first sign of acute myocarditis in patients of Dengue Hemorrhagic Fever in shock. We present here a case of 2nd Degree Mobitz Type II atrioventricular AV block in a case of Dengue Hemorrhagic fever reverting to the normal rhythm in recovery phase and no signs thereafter on follow up.
Dengue fever, Conduction block, Mobitz type II AV block
Case Report
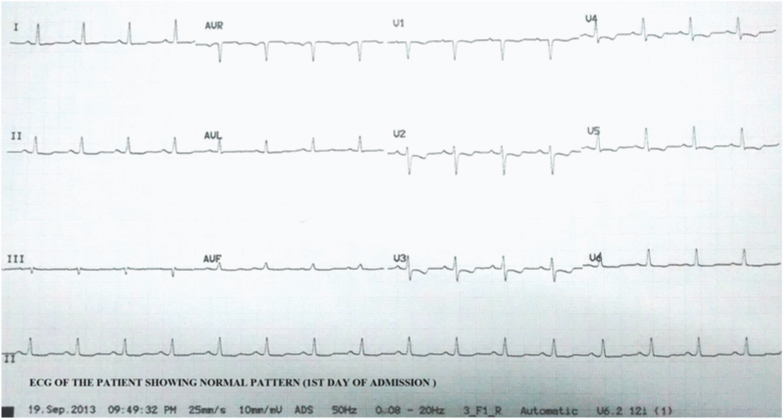
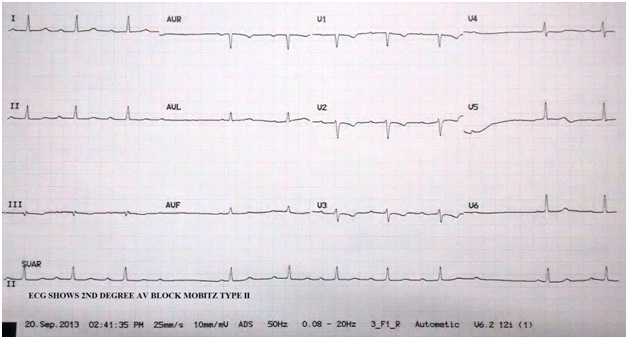
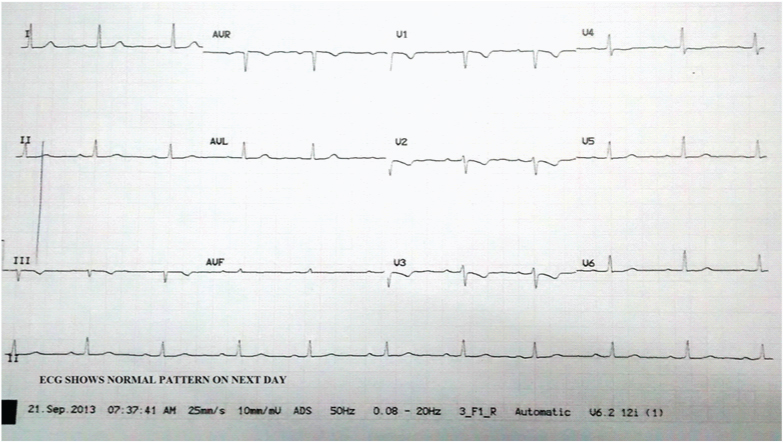
A 35-year-old female presented in emergency department with complaints of fever high grade, associated with chills and rigour, relieved on medication and with no diurnal variation for three days associated with generalized body ache, loss of appetite, nausea and a few episodes of vomiting. There was no history of cough, burning micturition, pain in abdomen, bleeding from any site. On general examination, patient was having conjunctival injection. There were no signs of clubbing, oedema, lymphadenopathy, and icterus. Her B.P was 100/70 mm Hg in right arm supine position, respiratory rate 24/min and pulse was 98/min regular low volume. On investigation her Hb was 10.2gm/dl and platelet count was 24000/ mm3 and Total Leukocyte Count was 3900/ mm3 with 60% Neutrophills and 38% Lymphocytes. In view of fever with thrombocytopenia and leukocytopenia, Dengue fever was suspected and Dengue serology was done and patient was found to be NS 1 positive and IgM antibody negative and hence patient was diagnosed as case of suspected dengue fever and was started on conservative treatment. Fever started subsiding on 5th day of illness but patient started complaining of dizziness and light headedness. Her blood pressure was normal and pulse was irregular and ECG was taken. On ECG a 2nd Degree AV Block Mobitz Type II was seen. On routine CBC her Hb was 10.1 gm/dl and TLC was 4700/ mm3 and platelet count was 61000/ mm3, her Na+ was 134meq/L, K+ was 4.17meq/L, Mg++ was 2.12meq/L and Ca++ was 9.2meq/L. Arterial blood gas analysis and CPK-MB came out to be normal. Echocardiography revealed no abnormality with no restrictive pattern. Next day patient did not have any complaint of lightheadedness or dizziness and no episode of fever and her ECG was normal. [Table/Fig-1,2,3] shows the evolution and disappearance of AV Block. Dengue serology was sent again on 10th day and IgM antibody was positive where as IgG antibody was negative. Later on patient was discharged and on follow up visit after one week ECG was done and found to be normal.
ECG showing the normal cardiac rhythm on the day of admission
ECG on the 5th day of admission showing the 2nd degree AV Block Mobitz Type II
Ecg on 6th day shows normal pattern
Discussion
Almost every year there is an epidemic of Dengue (August to November) and every outbreak of Dengue creates a state of panic among patients, doctors and media persons. This is mainly due to problem of over diagnosis & under diagnosis and irrational management. Dengue virus belongs to Genus Flavivirus, Family Flaviviridae and has four serotypes [1–4] and Type II is the most dangerous [1]. These viruses are transmitted predominantly by Aedes Aegypti commonly known as Tiger Mosquito [2]. Mosquito breeds in relatively fresh stagnant water and is day time biter with a limited flight range of 100 yards.
Usually the patient presents with complaints of fever, headache, rash, retro-orbital pain, severe myalgia, and arthralgia. Severe presentation like shock is seen in a number of patients though far less than the extent of cases diagnosed with dengue fever.
During the dengue epidemic, number of cases are quite high so atypical presentations of dengue may be suspected by an alert clinician in any patient who presents with high degree of fever with thrombocytopenia. Dengue can on occasions present with atypical presentations like acute abdominal pain, diarrhea, severe GI bleed, severe headache, convulsions, altered sensorium, encephalitis, intracranial hemorrhage, irregular pulse or heart rate, severe respiratory distress, fulminant hepatic failure, obstructive jaundice, acute renal failure, disseminate intravascular coagulation [3].
A number of patients also manifest symptoms and sign that are not commonly seen and close monitoring in these cases is required. Among the rare cardiac manifestations atrial fibrillation, type 1 AV block, myocarditis have been reported. Type 2 AV block during dengue illness has not been reported till date [4–7]. In our patient causes of reversible AV block like hyperkalemia, hypermagnesimia, hypothyroidism, drug history were ruled out. As patient was not having history of any chronic illness and had recovered completely on the conservative management chances of other infectious disease like Tuberculosis, Lyme’s disease, Chaga’s disease, Syphilis, were ruled out and it was concluded that the block was due to dengue illness that could have produced some kind of conduction abnormality in the AV node [8]. Therefore, extensive clinical and experimental studies are required to understand the pathological mechanism of AV node dysfunction.
Cardiac arrhythmias in patients of dengue fever are seen in cases of myocarditis and have lead to episodes of syncope and even sudden death therefore careful monitoring and evaluation of conduction abnormality is must during the illness [9]. In a case series reported by Wali et al., the mean ejection fraction was 47.06% in patients with dengue hemorrhagic fever and was 39% in patients with dengue shock syndrome. They also reported multiple ST and T wave changes in ECG which reverted back to normal within 3 months of follow-up along with ejection fraction [10]. Mobitz type 1 AV block has been reported by Khongphatthallayothin et al., from Thailand during the recovery phase of Dengue fever [11]. Sharma et al., reported variable atrio-ventricular block in an 18-year-old male with dengue fever who developed Mobitz type 1 AV block and AV dissociation that had a spontaneous resolution [12]. Our patient had Mobitz Type 2 AV block and recovered completely on third day and shows that dengue illness can cause reversible conduction abnormality in the AV node.
Conclusion
Mobitz Type II AV block in Dengue Hemorrhagic Fever can be benign and careful monitoring alone in these patients may suffice. Awareness about this condition and its course may prevent unnecessary evaluation and referral of these patients to tertiary centers. The clinical differentiation between dengue hemorrhagic fever and myocarditis can be difficult in certain patients, and patients presenting in shock with heart block must be assessed carefully and closely monitored. This phenomenon has rarely been reported in the past and still there is lack of data which makes further follow-up and reports of cardiac conduction defects in dengue hemorrhagic fever a necessity.
[1]. Malavige GN, Fernando S, Fernando DJ, Dengue viral infectionsPostgrad Med J 2004 80:588-601. [Google Scholar]
[2]. Deen JL, Harris E, Wills B, The WHO dengue classification and case definitions: time for a reassessmentLancet 2006 368:170-73. [Google Scholar]
[3]. Gulati S, Maheshwari A, Atypical manifestations of dengueTrop Med Int Health 2007 12:1087-95. [Google Scholar]
[4]. Veloso HH, Ferriera JA, De Paiva JMB, Acute atrial fibrillation during dengue hemorrhagic feverBrazilian Journal of Infectious Diseases 2003 7:418-22. [Google Scholar]
[5]. Punja M, Mark DG, McCoy JV, Electrocardiographic manifestations of cardiac infectious-inflammatory disordersAm J Emerg Med 2010 28:364-77. [Google Scholar]
[6]. Donegani E, Briceno J, Disorders of atrio-ventricular conduction in patients with hemorrhagic dengueMinerva Cardioangiol 1986 34:477-80. [Google Scholar]
[7]. Chuah SK, Transient ventricular arrhythmia as a cardiac manifestation in dengue hemorrhagic fever – a case reportSingapore Med J 1987 28:569-72. [Google Scholar]
[8]. Vijayaraman P, Ellenbogen KA, Bradyarrhythmias and pacemakers, in Hurst's The Heart 2008 12th edNew YorkMcGraw-HillV Fuster et al (eds) [Google Scholar]
[9]. Promphan W, Sopontammarak S, Pruekprasert P, Dengue myocarditisSoutheast Asian J Trop Med Public Health 2004 35:611-13. [Google Scholar]
[10]. Wali JP, Biswas A, Chandra S, Malhotra A, Aggarwal P, Handa R, Cardiac involvement in dengue haemorrhagic feverInternational Journal of Cardiology 1998 64(1):31-36. [Google Scholar]
[11]. Khongphatthallayothin A, Chotivitayatarakorn P, Somchit S, Mitprasart A, Sakolsattayadorn S, Thisyakorn C, Morbitz type I second degree AV block during recovery from dengue hemorrhagic feverSoutheast Asian J Trop Med Public Health 2000 31(4):642-45. [Google Scholar]
[12]. Sharma JK, Zaheer S, Variable atrio-ventricular block in dengue feverJIACM 2014 15(3-4):252-54. [Google Scholar]