The characteristic feature of axis is the presence of dens or odontoid process projecting superiorly from its body and specialized superior articulating facets. These facets do not form pillar with the inferior articulating facets, as these are present considerably anterior to inferior facets. Axis acts as a pivot or axle for rotation of the atlas and the head around the strong dens [1]. The atlas and axis vertebrae have unique shape and a complex vertebral artery relationship. Fracture of dens of axis accounts for 50-60% of all fractures of axis (C2) and 7-27% of all cervical spine fractures [2,3]. Anderson and D Alonzo [4] classified odontoid fracture into three subgroups and found type II being the most common (65-74%). Surgical treatment of odontoid fracture and other pathological process include anterior and posterior stabilization techniques, odontoid screw fixation and transoral odontoidectomy. Recently anterior screw fixation is preferred treatment for odontiod fracture [5]. Surgeries in these regions are highly risky because of complex vertebral artery relationship. Various authors have reported vertebral artery injury during surgeries in these regions. Pedicle screw can cause injury to vertebral arteries under the superior facets of axis during insertion. Gupta & Goel [6] recognized 2% rate of vertebral artery injury, Madawi et al., [7] recognized 8%, while Wright & Lauryssen [8] identified 4.1% rate of vertebral artery injury. These factors stress the importance of knowledge of morphometric anatomy of axis and surrounding region for surgeries in craniovertebral region especially anterior cervical surgeries. The aim of this study was to measure important anatomical parameters of the axis vertebrae with the objectives to establish the different anatomical parameters of human axis vertebrae of Indian subjects and to compare the results of present study with the results of others studies conducted by different authors in different populations. The knowledge of these parameters will help in surgical procedures to be performed safely in this region.
Materials and Methods
The present study was carried out on 30 human axis vertebrae used for teaching in the Department of Anatomy in Subharti Medical College Meerut (U.P) India. No identifiable information about the individual details of procured vertebrae was available. Only intact Indian axis vertebrae free from any bony abnormalities were included in the study. All linear parameters were measured using a digital caliper accurate to 0.01 mm for linear measurements. Angular parameters were measured using mini–inclinometer [9]. Different parameters of axis as described in [Table/Fig-1,2,3,4,5,6,7,8,9] were measured. The data obtained was analyzed statistically. Mean, standard deviation and range of different parameters was calculated.
Anatomic parameters of axis
| Sr No | | Parameter | Mean(mm)±SD | Range(mm) |
|---|
| 1. | Distance between tip of transverse process & midline- | Right(A-J [Table/Fig-2]) | 29.32 ±3.09 | 22.6-35.26 |
| Left(B-J [Table/Fig-2]) | 29.06±2.87 | 22.6-34.31 |
| 2. | Distance between SAF& Midline | Right(C-I [Table/Fig-2]) | 22.8 ±1.95 | 19.05-27.04 |
| Left(D-I [Table/Fig-2]) | 22.6 ±1.86 | 18.9-25.8 |
| 3. | Height of axis- | Anterior Height(G-K [Table/Fig-2]) | 34.33±2.69 | 29.21-40.5 |
| Posterior Height(L-M [Table/Fig-3]) | 30.56±2.78 | 23.9-35.84 |
| 4. | Body | Anterior body height(G-H [Table/Fig-2]) | 19.67±1.81 | 16.17-23.11 |
| Posterior body height(N-M [Table/Fig-3]) | 16.67±1.73 | 14.93-19.10 |
| A-P diameter of inferior surface (n-o [Table/Fig-5]) | 15.42±1.78 | 12.57-19.26 |
| Transverse diameter of inferior surface(p-q [Table/Fig-5]) | 17.7±2.22 | 13.65-25.9 |
| 5. | Dens | Anterior Height(G-H [Table/Fig-2]) | 14.66±1.37 | 13.04-17.39 |
| Posterior height(L-N [Table/Fig-3]) | 13.89±1.81 | 8.97-16.7 |
| A-P diameter(i-j [Table/Fig-6]) | 10.1±0.91 | 8.7-12.12 |
| Maximum trans diameter(X-Y [Table/Fig-2]) | 9.32±1.05 | 7.69-11.98 |
| Dens axis Sagittal angle (degree) (klm [Table/Fig-6,7]) | 13.230±4.36 | 40-210 |
| 6. | Superior articulating facet(SAF) | A-P diameter-Right([Table/Fig-4]) | 16.61±1.33 | 14.5-18.97 |
| A-P diameter- Left(a-b [Table/Fig-4]) | 16.7±1.49 | 13.13-19 |
| Transverse diameter-Right([Table/Fig-4]) | 14.92±1.76 | 11.1-17.28 |
| Transverse diameter- Left (c-d ) [Table/Fig-4]) | 14.79±1.95 | 11.49-17.8 |
| 7. | Inferior articulating facet(IAF) | A-P diameter-Right([Table/Fig-5]) | 11.75±2.33 | 8.22-18.6 |
| A-P diameter -Left(n-o ([Table/Fig-5]) | 12.02±2.29 | 7.6-16.13 |
| Transverse diameter-Right(Table/Fig-5) | 11.40±1.76 | 8.44-12.82 |
| Transverse diameter- Left (p-q) ([Table/Fig-5]) | 11.42±1.92 | 5.44-14.17 |
| 8. | Pedicle | Width-Right (x-y ) ([Table/Fig-4]) | 10.07±2.34 | 5.15-14.5 |
| Width-Left ([Table/Fig-4]) | 10.52±2.41 | 6.37-14.48 |
| 9. | Vertebral foramen | Transverse diameter (g-h) ([Table/Fig-4]) | 22.37±1.73 | 18.31-26.42 |
| A-P diameter at inlet (e-f) ([Table/Fig-4]) | 18.31±2.05 | 15.04-22.68 |
| A-P diameter at outlet (v-w) ([Table/Fig-5]) | 14.84±1.63 | 12.07-18.28 |
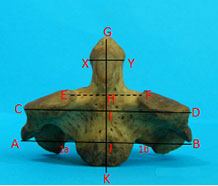
Description of different measurements from anterior aspect of axis. G-K represents Anterior height of axis. E-F is arbitrary line joining superior articulating facets of axis. H-K shows anterior body height of axis. G-H shows anterior height of dens. A-J and B-J are distances from midline to the tip of transverse process on right and left side respectively. C-I and D-I are distances from midline to the lateral most margin of superior articulating facet on right and left side respectively. X-Y is maximum transverse diameter of dens
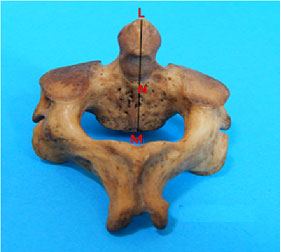
Description of axis measurements taken from posterior aspect. L-M is posterior height of axis. N-M is posterior body height. L-N is posterior height of dens
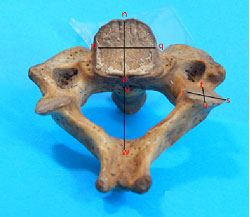
Description of axis measurements taken from superior aspect. a-b and c-d is showing anterio-posterior (A-P) diameter and transverse diameter of superior articulating facets respectively. g-h shows transverse diameter of vertebral foramen. e-f is showing anterio-posterior (A-P) diameter of vertebral foramen at inlet. x-y is pedicle width

Description of axis measurements taken from inferior aspect. n-o and p-q are anterio-posterior (A-P) and transverse diameter of inferior surface of body of axis respectively. r-s and t-u are transverse and anterio-posterior (A-P) diameter of inferior articulating facet respectively. v-w is anterio-posterior (A-P) diameter of vertebral foramen at outlet
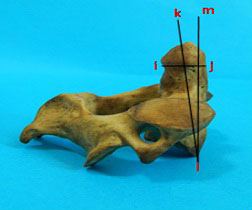
Description of axis measurements taken from lateral aspect. i-j is anterio-posterior (A-P) diameter of dens. klm is dens axis sagittal angle
Measurement of dens axis sagittal angle with mini inclinometer
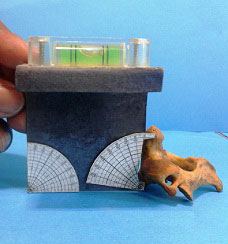
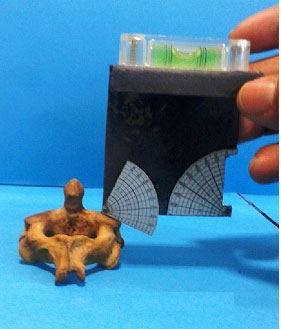
Frontal angle of superior articulating facet to be measured
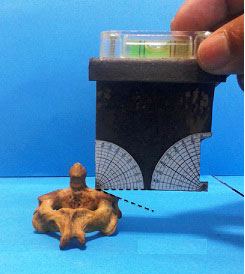
Method of measurement of Frontal angle of superior articulating facet
The different parameters of axis were measured as follows:-
(1) The distance from the midline of body to the tip of transverse process of axis on right side and left side was measured as shown in [Table/Fig-2].
(2) The methodology to measure distance from the midline of body to the lateral most edge of superior articulating facet of axis on right side and left side is shown in [Table/Fig-2].
(3) The anterior height of the axis was measured as the distance from the inferior edge of the body in the anterior midline to the tip of the odontoid process [Table/Fig-2].
(4) Dimensions of the body of axis- Anterior height of body of axis [Table/Fig-2] was measured at the anterior midline of the body from the inferior edge to the superior border, which was defined by a line drawn at the superior aspect of the superior articular processes [10]. Posterior vertebral body height [Table/Fig-3] was measured at the posterior midline of the body of the vertebra from the posterior inferior edge to the superior border [Table/Fig-4] [10]. The end plate lip height was calculated as the difference between the anterior body height and the posterior body height [11]. Anterio-posterior (A-P) and transverse diameter of inferior surface of axis [Table/Fig-5] were also measured.
(5) Odontoid process - The maximum transverse diameter [Table/Fig-2] and anterio-posterior (A-P) diameter of odontoid process [Table/Fig-6] were measured. The anterior height of the odontoid process was measured as the distance from tip of dens to the arbitrary horizontal line passing superior to the superior articular facet [Table/Fig-2]. Methodology to measure posterior height of dens is shown in [Table/Fig-3]. The dens axis sagittal angle was measured to be an angle [Table/Fig-6] between an axis that was imagined to pass longitudinally through the dens axis and the vertical line on a sagittal plane [5]. This angle was measured by mini-inclinometer [Table/Fig-7].
(6) Superior articulating facets (SAF). Both anterio-posterior (A-P) and transverse dimeters of SAF [Table/Fig-4] on right and left side were measured. The frontal angle of the superior articulating facet [Table/Fig-8] was an opening supposed to be the superior facet and the line which arbitrarily passed superior to them on the transverse plane [5]. To measure this angle mini inclinometer was used [9]. The right corner of the lower border of instrument was kept at highest point of the inclined surface of superior articulating facet and lower border of instrument was maintained in the horizontal plane with the help of bubble leveler. The protractor was moved downward till it touched the lowest point over the inclined surface and tilt of protractor was measured in degrees indicating the angle of inclined surface [Table/Fig-9].
(7) Inferior articulating facets (IAF).Transverse diameter and A-P diameter of IAF [Table/Fig-5] was measured on right and left side.
(8) Pedicle width [Table/Fig-4] was measured as the distance from the external surface of pedicle to its internal surface at the level of foramen transversarium [10].
(9) Vertebral canal:-The transverse diameter of vertebral canal [Table/Fig-4] was measured. The anterio-posterior (A-P) diameter of vertebral canal at inlet [Table/Fig-4] and outlet [Table/Fig-5] was measured.
Results
The results of this study are shown in [Table/Fig-1]. The mean distance from the midline of body to the tip of transverse process of axis was 29.32 mm on right side and 29.06mm on left side. The mean distance from the midline of body to the lateral most edge of superior articulating facet was 22.8 mm on right side and 22.6 mm on left side. The mean value of anterior and posterior height of axis was 34.33±2.69mm and 30.56±2.78mm respectively. The anterior and posterior height of body of axis was 19.67 mm and 16.67mm respectively. Mean A-P and transverse diameter of inferior surface of axis was 15.42mm and 17.7mm respectively. Mean transverse diameter and mean A-P diameter of odontoid process was 9.32mm and 10.1 mm respectively. Mean anterior and posterior height of the odontoid process was 14.66 mm and 13.89mm respectively. Mean of dens axis sagittal angle (angle between an axis that was imagined to pass longitudinally through the dens axis and the vertical line on a sagittal plane) was13.23 degree. The shape of superior articulating facets of C2 varies from oval to circular. In the present study, 84% of SAF were oval and 16% were circular. Inferior articulating facets were circular in shape in 90% cases, and oval in 10% vertebra. Mean pedicle width was 10.07mm on right side and 10.52mm on left side. Mean transverse diameter of vertebral canal was 22.37±1.73 mm. Mean of A-P diameter of vertebral canal at inlet was 18.31±2.05mm and mean of A-P diameter of vertebral canal at outlet was 14.84±1.63mm.
Discussion
The characteristic feature of axis is the presence of dens or odontoid process projecting superiorly from its body and specialized superior articulating facets [1]. The knowledge of the exact dimensions and shape of this bone is required for the evaluation of many clinical problems [11]. Surgical correction of the instability of the atlanto-axial complex or occipito-cervical junction because of numerous traumatic and non-traumatic conditions requires several surgical techniques, such as interlaminal clamping, interspinous wiring, and plate and screw fixation. In spite of the benefits conferred by transpedicular screw fixation in the cervical column, controversy exists regarding its potential risk. Incorrect insertion of a pedicle screw can cause damage to adjacent vital structures such as the spinal cord, nerve roots, cranial nerves and vertebral arteries [5]. As new internal fixation methods evolve, some authors have found clear indications of better understanding of the geometry and dimensions of the axis [11].
Morphometric anatomy of the axis vertebra is important for different surgical procedures. [Table/Fig-10,11] compare the different parameters of the axis in the present study and those reported in previous studies by other authors. The anterior C2 body may be used for anterior cranio-vertebral fixation. In the present study, the mean value of the anterior height of the C2 vertebral body was 19.67 mm. Lang [12] measured the same parameter with its value 22.1mm and Lu et al., [13] found this parameter as20.4 mm. The mean value of the posterior height of C-2 body was found to be 16.67mm. Naderi et al., [14] measured this height as 17.2±2.2mm, while Schaffer et al., [15] found this value as 19.7mm.Kandziora et al., [16] reported this parameter to be 17.8±1.45mm. In our study, the anterio-posterior (A-P) and transverse diameter of the C2 body were found to be 15.42±1.78mm, and 17.7±2.22mm respectively. This is in line with results reported by Naderi et al., [14]. They reported these parameters as 15.8mm and 18.1mm respectively. They stated that these parameters can be taken into consideration during the anterior plating of the C2 body using screws to detect the screw length.
Comparison of parameters of axis of present study with other studies
| Parameter | | Naderi et al., [14] | Xu et al., [20] | Doherty & Heggeness [11] | Senegul & Kodiglu [5] | Gosavi S, Swamy [10] | Present study |
|---|
| Distance between tip of Transvese Process & midline | Right (mm) | - | - | - | 27.3 | 26.68 | 29.32 ±3.09 |
| Left (mm) | - | - | - | 27.2 | 26.66 | 29.06±2.87 |
| Distance between Superior Articulating Facet & Midline- | Right (mm) | - | - | - | 21.0 | 20.92 | 22.8 ±1.95 |
| Left (mm) | - | - | - | 21.9 | 21.75 | 22.6 ±1.86 |
| Height of axis- | Anterior Height (mm) | 38.7±2.9 (33.0-46.6) | - | - | - | 34.17 | 34.33±2.69 |
| Posterior Height (mm) | 33.2±2.9 (27.5-42.4) | - | ----- | ----- | ----- | 30.56±2.78 |
| Body | Anterior body height (mm) | 23.2±2.4 (17.8-34.5) | Female 19.5±1.7(17-23) Male 21.1±1.7 (18-24) | 23.3 | 22.1 | 20.49 | 19.67±1.81 |
| Posterior body height (mm) | 17.2±2.2 (13.6-27.5) | Female 15.3±1.1(14-18) Male 16.5±1.6 (14-20) | - | - | 16.07 | 16.67±1.73 |
| A-P diameter of inferior surface (mm) | 15.8±1.7 (12.5-20.2) | Female 15.0±1.7(12-18) Male 16.1±1.5(14-20) | 16.2 | - | 14.77 | 15.42±1.78 |
| Transverse diameter of inferior surface (mm) | 18.1±1.8 (14.7-24.7) | Female 18.7±2.5(15-25) Male 19.0±2.0(14-23) | 18.7 | - | 15.99 | 17.7±2.22 |
| Dens | Anterior Height (mm) | 15.5±1.8 (11.5-19.8) | Female 14.6±1.5 (12-17) Male 15.5±1.8 (11-18) | - | 14.5 | 14.86 | 14.66±1.37 |
| Posterior height(mm) | 15.4±1.9 (11.5-20.7) | _______________ | ----- | ----- | ----- | 13.89±1.81 |
| A-P diameter (mm) | 11.3±1.0 (9.3-13.8) | Female 9.6±0.9(8-11) Male 10.3±0.7(7-11) | 11.2 | - | 9.92 | 10.1±0.91 |
| Maximum trans diameter (mm) | 10.5±0.9 (8.0-12.5) | Female 9.6±0.9(8-11) Male 10.0±0.9(8-15) | 10.8 | 11.2 | 9.28 | 9.32±1.05 |
| Dens axis Sagittal angle (degree) | ----- | ----- | ----- | 9.7 | ----- | 13.230±4.36 |
Comparison of parameters of axis of present study with other studies
| Parameter | | Xu et al., [20] | Doherty & Heggeness [11] | Senegul & Kodiglu [5] | Gosavi S, Swamy [10] | Present study |
|---|
| Superior articulating facet(SAF) | A-P diameter (mm) -Right | ----- | ------ | 17.5 | 16.64 | 16.61±1.33 |
| A-P diameter(mm) Left | ------ | -------- | 16.66 | 16.7±1.49 |
| Transverse diameter(mm)-Right | ----- | ------ | 14.0 | 14.44 | 14.92±1.76 |
| Transverse diameter (mm)-Left | ------ | ------ | 14.64 | 14.79±1.95 |
| Shape-Oval | ------ | ------ | 86% | 63% AP diameter>Transverse diameter | 84%- 60% AP diameter>Transverse diameter 24%-Transverse diameter>AP diameter |
| Circular | ------ | ----- | 14% | 37% | 16% |
| Frontal angle-Right (degree) | ---- | ------ | 26.2 | ------- | 21.770±4.46 |
| Left(degree) | ----- | ----- | 28.2 | ----- | 20.80±4.96 |
| Inferior articulating facet | A-P diameter(mm)-Right | 20mm Male 19 mm Female | ------ | 11.6 | 9.74 mm | 11.75 mm |
| A-P diameter (mm) –Left | ------ | ------ | 9.61 | 12.02±2.29 |
| Transverse diameter(mm)-Right | ------ | ------ | 9.5 | 9.93 | 11.40±1.76 |
| Transverse diameter(mm) -Left | ------ | ------ | 9.92 | 11.42±1.92 |
| Shape -Oval | ------ | ------ | 4% | _ | 10% |
| Circular | ------ | ------ | 96% | _ | 90% |
| Pedicle | Width(mm)-Right | 8.6 | ----- | 9.5 | 7.19 | 10.07±2.34 |
| Width(mm)-Left | ----- | 7.73 | 10.52±2.41 |
| Vertebral foramen | Transverse diameter(mm) | 21.9 | 23.6 | 24.7 | 21.59 | 22.37±1.73 |
| A-P diameter at inlet(mm) | 18 | 16.5 | 20.8 | 18.47 | 18.31±2.05 |
| A-P diameter at outlet(mm) | 15.3 | - | - | 15.11 | 14.84±1.63 |
There is controversy regarding the best approach for treatment of fracture of odontoid process, when the fracture occurs at the base of the odontoid process at its junction with the body of axis. In routine, the surgeon performs surgical procedure involving posterior fusion of the arches of the atlas and axis. But this technique may require an additional period of external immobilization for the stabilization to be successful. Although this technique provides better stabilization of spine, but there is an important limitation of this approach. This approach restricts the normal rotation between atlas and axis, which usually account for more than one half of the normal axial rotation of the cervical spine [5]. Alternative approach to the odontoid process is anterior trans-oral approach. Anterior screw fixation allows direct fixation of fracture, provides stability, but in addition to this, it preserves normal movements of the cervical spine. In this anterior screw fixation technique, one or two screws are inserted from the inferior edge of the axis through the body of axis and into the odontoid process to its apex. The trajectory of the screw for anterior screw fixation of odontoid is parallel to the vertical axes of the odontoid [5]. So surgery in this region requires information regarding the odontoid process and the C2 body. In the present study, the mean of widest transverse diameter of odontoid process was 9.31±1.05mm. The mean value of the height of anterior aspect of axis measured from the inferior aspect of the anterior surface of body of axis to the tip of its odontoid process was 34.33±2.69mm and anterior height of the odontoid process, measured as a distance from tip of dens to the horizontal line passing superior to the superior articular facet, ranged from 13.04mm-17.39mm (mean 14.66mm). The mean value of the height of posterior aspect of axis measured from the inferior aspect of the posterior surface of body of axis to the tip of its odontoid process was 30.56±2.78mm and posterior height of the odontoid process was 13.89mm. Mean Dens axis sagittal angle was13.23 degree (4-21 degree)
Karaikovic et al., [17] found that approximately 92% of their 53 specimens had isthmus widths more than 4 mm. In the study of Mandel et al., [18], who used both anatomic and computed tomographic measurements in 205 human cadavers' C2 vertebrae, only 2.4% had one or both isthmus widths of less than 5mm. Gupta & Goel [6] reported that the mean screwable thickness of C2 pedicle was 7.8 mm, and that the mean height of the pedicle was 8 mm. Sengul & Kadioglu [5] found that the width of C2 pedicle ranged from 4 to 12.5 mm; 7.5% of specimens had isthmus widths of less than 5 mm [18] expressed their views by stating that its technically difficult to place a 3.5 mm screw in a patient with C2 isthmus dimensions (smaller than 5 mm in either the height or width). In the presence of a small C2 isthmus width and/or height, approximately 10% of patients may be at risk for a vertebral artery injury with placement of C1-C2 transarticular screws. In the present study, the width of axis pedicle ranged from 5.15-14.5mm (mean 10.07mm) on right side and 6.37-14.48mm (mean 10.52mm) on left side. No vertebrae were found with pedicle width less than 5mm.
Cacciola et al., [19] worked on the vertebral artery in relation to C1-C2 vertebrae and studied the detailed anatomy of vertebral artery. They found that after the artery exit from the foramen transversarium of C3 vertebra, it loops medially towards SAF of C2, making a deep loop within the vertebral artery groove on the inferior surface of SAF of C2 and then it exits from the foramen transversarium of C2 vertebrae. They also pointed out two important observations regarding superior articulating facet of axis. First point is that these facets of axis are present in close proximity to the body and medial aspect of pedicle as compared with other vertebrae where they are located close to the junction of pedicle and lamina. Secondly; the foramen transversarium of the axis is present partially or completely on the inferior surface of superior articulating facets as compared to other cervical vertebrae, where this foramen is located entirely in relation to the transverse process. This unusual location of vertebral artery can make the artery prone to injury if the screw is directed straight ahead anteriorly in a sagittal plane. The shape of superior articulating facets of C2 varies from oval to circular. In the present study, 84% of SAF were oval and 16% were circular. Further in the oval facet, the AP diameter was more than transverse diameter in 60% cases and in other 24% cases transverse diameter was more than AP diameter. Frontal angle of superior articulating facet was 21.77±4.46 degree and 20.8 ±4.96 degrees on right and left side respectively. Inferior articulating facets were circular in shape in 90% cases, and oval in 10% vertebrae. Xu et al., [20] also measured the inferior articulating facets in male and females, and the values of these parameters are shown in [Table/Fig-11].
The variations seen in the parameters in different studies are perhaps due to the difference in the ethnicities to which these vertebrae belonged in various studies.
Conclusion
From the present study, we obtained the vital anatomical data on different parameters of the axis of Indian origin which may be helpful for the surgeons in avoiding and minimizing complications such as vertebral artery injury, cranial nerve damage and injury to other vital structures while performing any surgical or interventional procedure around cranio-vertebral region.