It has always been a herculean task to prosthetically rehabilitate edentulous patients with severe resorption of the maxillary ridge. As resorption progresses, narrowing and constriction of residual ridge occurs which decreases the supporting tissues and result in increased restorative space between the maxillary and mandibular residual ridges.
The consideration of reducing the weight of the prosthesis has always been attempted and proved beneficial in obturators, which conversely holds true in complete dentures as well [1]. But whether reducing the weight of conventional complete denture also increases retention or not, is still very dubious. It is well documented fact that the weight of the denture contributes significantly to both the retention and stability of complete dentures. Additional retentive aids like springs or magnetic inserts were also used. Increasing the weight of a mandibular denture improved its retention [2]. Grunewald observed that the combined weight of the lost alveolar hard and soft tissue amounts to approximately 40 to 50 gm and should be consistent with denture replacing them [3]. Pertinent to the scenario, several eminent clinicians advocate conventional dentures for the rehabilitation of severely resorbed edentulous mandibular ridges [4,5]. Denture stability can usually be obtained without the hollowing of the denture, simply by improving the fit of the denture base and thus by creating an appropriate denture outline and occlusal relationship.
In contrary to Nakamura, who had conflicting dialect against the weighted denture method [6], Holt was of opinion that gouging reduced the excessive weight of a denture in patients with severely resorbed residual alveolar ridges [7]. The critics were also behind the fact that extra weight would hasten the resorption of the underlying ridge [8]. Till today, diverse opinions still persist about the weighted denture. It is quite apparent in the literature review that the study of the effect of denture weight has been neglected for quite some time. Denture stability has always been the epitome of various clinical studies [9–11] and patient’s satisfaction with dentures [12–15] but the concern of weight has still not been well scrutinized [16]. More-so-over, the amount of the weight in the mouth also remains an ambiguity.
This pilot study was aimed at determining the effect of maxillary denture weight on denture retention and stability for which consideration was also given to the parameters of patient’s preferences in terms of comfort and chewing with different denture weights.
Materials and Methods
For this study, the inclusion criteria for selection of the patients were good general health, healthy oral mucosa, adequate interarch space in completely edentulous mouths, with co-operative attitude and motivated patients. The exclusion criteria included patients with serious systemic illness like poorly controlled Diabetes Mellitus & neurological problems or bony disorders and locally any tori, exostosis or any flabby tissue. On the basis of these criteria, a total of 10 patients were considered for the pilot study (06 female and 04 male) with an average age of 70 y [Table/Fig-1]. Each patient was provided with two sets of maxillary complete dentures, one hollow labeled as A and one conventional maxillary denture labeled as B.
Showing the patients’ details
| S.No. | Age & Gender | No of years complete denture worn | Ridge resorption | Type of Maxillary Denture |
|---|
| 1 | 68/F | 5 | Moderate | Hollow (A) & Conventional Dentures (B) |
| 2 | 70/F | 2 | Moderate | Hollow (A) & Conventional Dentures (B) |
| 3 | 65/M | 1 | Moderate | Hollow (A) & Conventional Dentures (B) |
| 4 | 72/M | 3 | Moderate | Hollow (A) & Conventional Dentures (B) |
| 5 | 65/F | 6 | Severe | Hollow (A) & Conventional Dentures (B) |
| 6 | 65/F | 5 | Moderate | Hollow (A) & Conventional Dentures (B) |
| 7 | 69/F | 7 | Moderate | Hollow (A) & Conventional Dentures (B) |
| 8 | 67/F | 3 | Severe | Hollow (A) & Conventional Dentures (B) |
| 9 | 64/M | 2 | Moderate | Hollow (A) & Conventional Dentures (B) |
| 10 | 71/M | 1 | Moderate | Hollow (A) & Conventional Dentures (B) |
The study was conducted in the following design:-
Insertion of Hollow (A) and conventional dentures (B)
↓
Measurement of retention (5 times each) using Modified Kapur index
↓
Measurement of stability using Modified Kapur index
↓
Interview about comfort and chewing
Preparation of the Experimental Dentures
The following clinical and lab procedures were carried out for oral rehabilitation:- Maxillary and mandibular primary impressions were made with impression compound (Pinnacle, DPI). The special trays were fabricated with self cure Poly methyl methacrylate (PMMA) resin and final impressions were made with ZOE paste (Septodont). The impressions were poured with type III dental stone (Kalabhai). The master casts were retrieved and permanent denture bases were acrylized. Occlusal rims were fabricated using modelling wax. Face bow record was made and transferred onto a semi adjustable articulator Hanau H2 articulator. Jaw relation in centric was registered at desired vertical dimension of occlusion using bite registration paste (Coltene Whaledent). Teeth arrangement was done using semi-anatomic teeth and balanced occlusion was achieved, followed by try-in in the patient’s mouth.
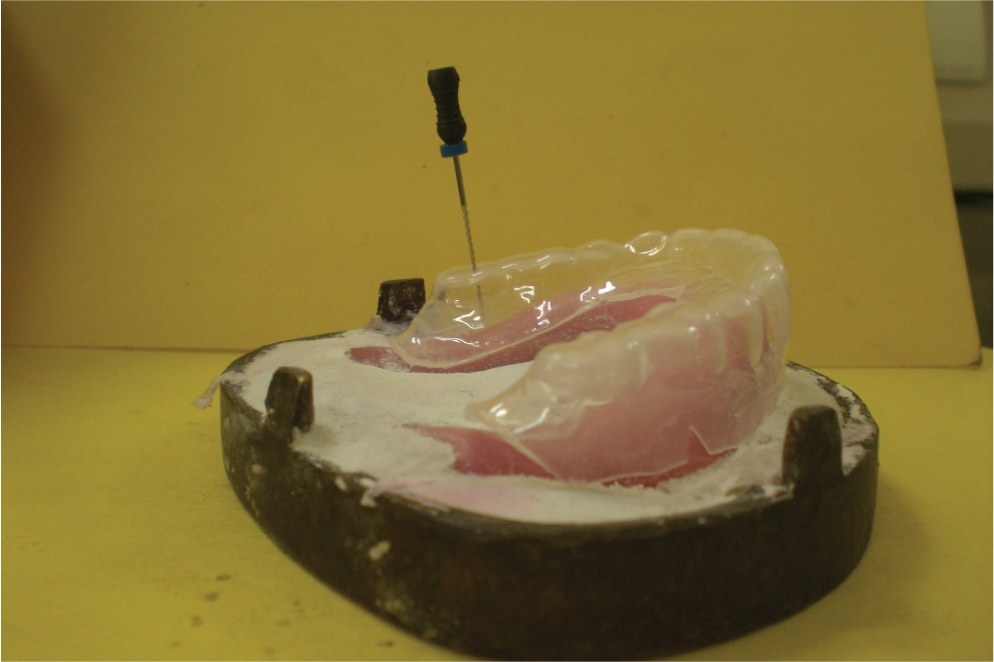
After the try in, the maxillary teeth arrangement along with denture base and cast was duplicated for conventional maxillary denture. A template was made in 2mm Biostar (Polyethylene) sheet. The casts with teeth were flasked and de-waxing was done. After the de-waxing, the template was placed on permanent maxillary denture base and a file was inserted to ensure that sufficient space is available between denture base and teeth [Table/Fig-2]. After confirming the space, rope shaped poly vinyl-siloxane putty was secured on maxillary permanent denture base with cyanoacrylate adhesive [Table/Fig-3]. In conventional way flasking and curing of denture were done for both hollow and conventional dentures. Once the dentures were fabricated, small holes were drilled in posterior and slightly palatal region of the denture, putty was removed and holes were closed with self cure PMMA resin [Table/Fig-4]. Another conventional maxillary denture was fabricated in conventional manner for the same patient by same doctor and technician to eliminate the denture processing errors.
Showing the availability of space

Space created for removal of putty

The maxillary hollow (A) and conventional dentures (B) were weighed. The weights were 20 gm and 30 gm respectively [Table/Fig-5,6]. There was a difference of 10 gm i.e. more than 25% reduction in weight between the hollow and conventional denture. The final prostheses were inserted in situ and occlusion was verified and corrected for both dentures.
Weight of denture after putty removal

Weight of denture made with conventional manner

Measurement of denture retention
The Modified Kapur Index Score (MKIS) for retention was used to assess the retention of the dentures. After insertion of maxillary hollow denture, the retention was assessed for maxillary hollow and conventional dentures and mandibular dentures using Modified Kapur index [Table/Fig-7]. According to Modified Kapur index for retention, the scores of maxillary and mandibular dentures are summed and based on scores, they were they were classified as excellent, good and poor dentures [Table/Fig-8] [9].
Readings of Maxillary and Mandibular dentures using Modified Kapur Index for retention and stability
| Case No | Score with hollow maxillary denture (A) | Score with conventional maxillary denture (B) | Score with conventional mandibular denture (C) | Sum total of hollow maxillary and mandibular denture ( A+C) | Sum total of conventional maxillary and mandibular denture (B+C) |
|---|
| Retention | Stability | Retention | Stability | Retention | Stability | Retention | Stability | Retention | Stability |
|---|
| 1 | 5 | 4 | 5 | 4 | 4 | 3 | 9 | 7 | 9 | 7 |
| 2 | 4 | 4 | 5 | 4 | 5 | 3 | 9 | 7 | 10 | 7 |
| 3 | 4 | 3 | 4 | 4 | 3 | 3 | 7 | 6 | 7 | 7 |
| 4 | 3 | 3 | 5 | 4 | 3 | 3 | 6 | 6 | 8 | 7 |
| 5 | 4 | 3 | 4 | 3 | 3 | 2 | 7 | 5 | 7 | 5 |
| 6 | 3 | 3 | 4 | 4 | 4 | 3 | 7 | 6 | 8 | 7 |
| 7 | 5 | 3 | 5 | 4 | 5 | 4 | 10 | 7 | 10 | 8 |
| 8 | 4 | 2 | 3 | 2 | 4 | 2 | 8 | 4 | 7 | 4 |
| 9 | 4 | 3 | 4 | 3 | 3 | 3 | 7 | 6 | 7 | 6 |
| 10 | 4 | 3 | 5 | 4 | 4 | 3 | 8 | 6 | 9 | 7 |
| Mean Value | 7.8 | 6 | 8.2 | 6.5 |
Modified Kapur index for retention and stability
| Score | Retention Criteria |
|---|
| 5 | Excellent | When a denture offers excellent resistance to vertical pull and lateral force |
| 4 | Very Good | When a denture offers very good resistance to vertical pull and lateral force |
| 3 | Good | When a denture offers moderate resistance to vertical pull and lateral force |
| 2 | Fair | When a denture offers resistance to vertical pull and lateral force |
| 1 | Poor | When a denture offers moderate resistance to vertical pull and little or no resistance to lateral force |
| 0 | No Retention | When a denture seated in its place displaces itself |
| Score | Stability Criteria |
| 4 | Excellent | When a denture offers excellent stability, demonstrates no rocking on its supporting structures under pressure |
| 3 | Good | When a denture offers good stability, demonstrates very slight rocking on its supporting structures under pressure |
| 2 | Fair | When a denture offers sufficient stability, demonstrate slight rocking on its supporting structures under pressure |
| 1 | Poor | Some stability, demonstrate moderate stability on its supporting structures under pressure |
| 0 | No Stability | When a denture base demonstrate extreme rocking on its supporting structures under pressure |
Maxillary and mandibular dentures were scored separately for retention and stability criteria. The sum score is the total score for maxillary and mandibular dentures
Clinically poor dentures= sum score of <6
Clinically fair dentures= sum score of 6-9
Clinically good dentures= sum score of 10-14
Clinically very good dentures= sum score of >14
Measurement of denture stability
The stability was also measured for maxillary hollow and conventional dentures and mandibular dentures [Table/Fig-7]. According to modified Kapur index (MKIS) for stability also, the scores of maxillary and mandibular dentures are summed and based on scores they were they were classified as excellent, good and poor dentures.
Maxillary and mandibular dentures were scored separately for retention and stability criteria. The sum score is the total score for maxillary and mandibular dentures [17].
Clinically poor dentures= sum score of <6
Clinically fair dentures= sum score of 6-9
Clinically good dentures= sum score of 10-14
Clinically very good dentures= sum score of >14
All the data was analyzed using SPSS statistical package (Version 7.5, SPSS In). The paired t-test was done. The standard deviation and p-values were calculated.
Patients’ experience about comfort and chewing
After 04 weeks of the denture insertions, all 10 patients were assessed for comfort level and chewing efficiency with both hollow (A) and conventional dentures (B) without being aware of denture weight. After being told about the weight difference, the subjects were again assessed, to determine which, if either, they preferred for comfort and chewing.
Results
The mean values of dentures retention using MKIS for retention were calculated and it was shown that mean values for retention using MKIS for retention for hollow dentures (A) was 7.8 and for conventional dentures (B) it was 8.2. This showed that retention with conventional maxillary dentures (B) was slightly more than the hollow maxillary dentures (A) but it was insignificant as p-value was 0.168 (>.1).
The mean values of denture stability using MKIS for stability for hollow dentures (A) was 6 and for conventional dentures (B) it was 6.5 .This showed that the stability for maxillary dentures was more with conventional dentures (B) than hollow maxillary dentures (A) and it was significant as p-value was 0.015 (p<.1).
Interviews about comfort and chewing
The results of their denture selection based on comfort and chewing are presented in [Table/Fig-9]. In selecting a denture for comfort, 05 of the patients preferred conventional dentures (B), 04 patients preferred hollow dentures (A) and only 01 could not make out the difference between the two. When asked about chewing, 05 patients preferred the conventional dentures (B), 03 preferred patient hollow dentures (A), but 2 patients did not indicate a preference for either type of denture.
Showing the preferences of patients based on comfort and chewing
| Case No | Comfort | Chewing |
|---|
| 1 | C | C |
| 2 | C | C |
| 3 | H | H |
| 4 | H | H |
| 5 | C | C |
| 6 | C | C |
| 7 | H | C |
| 8 | H | Δ |
| 9 | C | Δ |
| 10 | Δ | H |
C- Conventional denture, H- Hollow Maxillary denture, Δ- No preferences
Discussion
The prosthetically driven treatment of severely resorbed ridges has always posed a serious challenge to the clinician, even though, the pertinent choice of rehabilitation can be tooth-supported overdentures, implant retained and tissue supported over-dentures with ridge augmentation. It is quite often that most of the geriatrics with such glitch are associated with systemic illnesses. Hence, the more predictable way out is to rehabilitate them with conventional complete dentures. Use of an innovative impression technique to get maximum denture bearing area, along with recording of requisite extensions of denture may also deliver superior results to such patients.
In our study, since the differences of denture weight did not affect the masticatory efficiency for the patients, therefore reducing the denture weight suddenly may not be good for masticatory efficiency. However, as patients become accustomed to the conventional weight of the denture during their chewing cycles so reducing the denture weight may not be required since masticatory movements tend to become smooth again with time. On the basis results in both the groups, it was not significant that decreasing the denture weight would improve maxillary denture retention in resorbed maxillary ridges as p>.1(.168). Many subjects did not notice the change in denture weight, even after chewing. Several studies have demonstrated that patients’ judgment of a complete denture can be predicted by information related to patients’ perception and previous experiences. Thus, much effort has been made to study the threshold and senses in the mouth, such as pain, touch, pressure, taste, and temperature.
There is a statement that patients over 60 y of age are less sensitive than those under [18]. Therefore, the from the age distribution, the subjects in this study would not be expected to have sharp senses in the mouth. Since the patients were likely to be influenced by a preconceived idea about denture weight, they were not made aware of the denture weights. The patients could not discriminate the difference of denture either by the sense of pressure to the underlying alveolar tissues or with the bite force to control masticatory movements.
On analyzing the patients’ data of selection of a denture for comfort from among both groups of dentures, A and B, 05 subjects had preferred conventional dentures, 04 subjects preferred hollow dentures and 01 had no preference. All 4 subjects who selected light hollow dentures gave their reason that it was comfortable. Regarding chewing, 5 subjects preferred conventional dentures and 3 subjects preferred hollow dentures. No subjects were able to discriminate the difference of denture weight, but after being made aware of the weight change, most of them could definitely appreciate the differences in weight of dentures. On the basis of the results of this study, there is no reason to unnecessarily reduce denture weight, especially if suitable retention and stability of maxillary dentures are maintained.
Limitations of The Study
The sample size was small and bigger sample size is required.
Additional methods to measure retention and stability should have been used.
Conclusion
The denture retention and stability values of conventional dentures and hollow dentures were not found to be significantly different. However they were slightly better for conventional dentures. In selecting a denture for comfort, 05 subjects preferred conventional dentures and 04 subjects preferred hollow dentures and only 01 who could not make out the difference. For chewing, 05 subjects answered that they were satisfied with conventional dentures, 03 subjects preferred the hollow dentures, but 02 subjects did not indicate a preference for one denture over the other.