Extraskeletal Chondroma of the Gluteal Region Along with Sporadic Neurofibroma - An Unusual Presentation
Asmita Parihar1, Nirupma P. Khan2, Vivek Agrawal3
1Senior Resident, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
2Consultant Pathologist, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
3Professor, Department of Surgery, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Asmita Parihar, 8/3 Gulmohar Road, Shipra Sun City, Indirapuram, Ghaziabad, Uttar Pradesh-201014, India.
E-mail: dr.asmitaparihar@gmail.com
Extraskeletal or soft tissue chondroma is a benign cartilaginous tumour that predominantly involves the hands and feet. We present a rare case of gluteal extraskeletal chondroma in a 55-year-old Indian female. She presented with right gluteal mass measuring 5 cm in greatest dimension. The diagnosis was provided through histopathological examination of completely excised tumour mass. The patient also had sporadic neurofibroma in the supraclavicular region. Such a unique association has not been reported till date in the English literature. We describe the clinical and histopathological characteristics of our case, emphasizing the first reported association of extraskeletal chondroma and sporadic neurofibroma.
Buttock, Soft tissue tumour, Supraclavicular
Case Report
A 55-year-old female presented to the Department of Surgery with swelling in the right gluteal region for three years and another swelling in the left supraclavicular region for four months. The gluteal swelling was painless, gradually increasing in size and causing difficulty in sitting, while the supraclavicular one was tender. The patient had no other lump anywhere on her body. There were no systemic complaints and no family history of neurofibromatosis.
Local examination showed a 5 x 3 cms, firm to hard mass in the right gluteal region which was non-tender and not fixed to the underlying bone or to the overlying skin. In the left supraclavicular region, there was a 3 x 2 cms well defined mass, firm in consistency, tender and palpation elicited tingling sensation in her left arm. There were no freckles, café au lait macules or Lisch nodules on systemic and ophthalmologic examination. Patient was operated for the excision of both the large lumps. Per-operatively, an encapsulated mass was identified in the subcutaneous plane of right gluteal region. The mass was excised with the capsule. In the left supraclavicular region, an unencapsulated tumour was present involving the lateral cord of left brachial plexus. This tumour was excised with attempt to preserve nerve as much as possible. Both the specimens were sent to Department of Pathology for histopathological examination.
On gross examination, the specimen from right gluteal region measured 5 x 3 x 3 cms, was encapsulated and had a lobulated outer surface. On cutting, the tumour had gritty consistency, and cut section showed multiple variably sized grey-white nodules [Table/Fig-1]. The left supraclavicular specimen was received as two unencapsulated grey-white soft tissue pieces together measuring 2.5 x 1.5 x 1 cm.
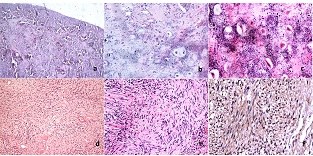
Microscopic examination of right gluteal tumour mass showed an encapsulated tumour mass composed of well defined lobules of mature hyaline cartilage. Calcification was identified as granular and floccular material surrounding the chondrocytes. No fibrosis, ossification or myxoid change was noted. There was absence of undifferentiated tumour cells, necrosis and demonstrable mitotic activity [Table/Fig-2a-c]. Based on these features, a histopathologic diagnosis of extraskeletal chondroma, right gluteal region was made. Microscopy of left supraclavicular specimen showed an unencapsulated tumour mass composed of interlacing bundles of spindle shaped cells in a myxoid matrix. The spindle cells had wavy nuclei and inconspicuous nucleoli [Table/Fig-2d,e]. On immunohistochemistry, the tumour cells were positive for S-100 protein, confirming the neural origin [Table/Fig-2f]. These features suggested the diagnosis of neurofibroma. Thus, a final diagnosis of right gluteal extraskeletal chondroma with left supraclavicular neurofibroma was given.
Postoperatively, patient developed grade 4 muscle weakness (movement against external resistance, but less than normal) in her left arm; this risk was explained to the patient before surgery.
Discussion
Extraskeletal chondromas are rare benign cartilaginous tumours of soft tissues [1,2]. Their exact aetio-pathogenesis is still unclear. It has been suggested that they develop from pleuripotent mesenchymal cells which differentiate along the lines of cartilage [3]. These tumours most commonly involve the fingers of middle aged adults, other sites being toes and feet [1,2]. Rarely it may involve parotid gland [4], fallopian tube [5] and scalp [6]. We present a rare case of soft tissue chondroma of the gluteal region. In our literature review, we found only one published case report of extraskeletal chondroma in the buttock of a Nigerian athlete. [7] This patient had recurrent lesions and their diagnosis was based on incisional biopsy, as the patient refused complete surgical removal of the recurrence [7].
Most of the extraskeletal chondromas are solitary and present as gradually enlarging, painless mass [1]. Their confirmed diagnosis can only be offered on histopathological examination of the excised tumour.
On gross examination, these tumours are firm, well-circumscribed and lobulated. They rarely exceed three centimetres in greatest dimension [2]. In our patient, the tumour was large measuring five centimetres in greatest dimension. Microscopic examination of a typical chondroma shows a well-delineated tumour mass composed of lobules of mature hyaline cartilage. Calcification outlines the contours of chondrocytes in a lace-like pattern [1,2]. The indexed case confirmed to these findings
Morphologically, the differential diagnoses which need to be considered are tumoural calcinosis, synovial chondromatosis and extraskeletal mesenchymal chondrosarcoma [2]. In tumoural calcinosis, there is dense calcification and histiocytic response to the calcified material, but it lacks cartilage [2]. Synovial chondromatosis occurs usually in large joints and consists of numerous cartilaginous nodules [2]. Extraskeletal mesenchymal chondrosarcoma is a malignant cartilaginous tumour occurring most commonly in the head and neck region. Microscopically, it shows well-defined nodules of well-differentiated hyaline cartilage, with an abrupt transition to sheets of undifferentiated round, oval or spindle-shaped cells. They frequently show central calcification [2]. Diagnostic problems may arise if small incisional biopsy is submitted. In the present case, tumour was completely excised and microscopy did not show crowding of chondrocytes, mitosis or necrosis on thorough sampling of the specimen.
Extraskeletal chondromas have a 15-25% risk of local recurrence [2]. Therefore, wide local excision is advised. Our patient has not shown any evidence of recurrence on three month follow up, postoperatively.
The left supraclavicular neurofibroma appears to be sporadic in nature as it did not fulfil any of the criteria of neurofibromatosis [8]. The concurrence of sporadic neurofibroma and extraskeletal chondroma has not been reported till date in the available English literature.
Gross photograph of gluteal mass showing multiple variably sized grey-white nodules

Histopathologically, gluteal tumour showed hyaline cartilage with benign chondrocytes and floccular calcification (a) (H&E stain x40), (b) (H&E stain x100), (c) (H&E stain x400); supraclavicular tumour consists of spindle cells with wavy nuclei, (d) (H&E stain x40), (e) (H&E stain x100), (f) S-100 immunopositive (x400)
Conclusion
Whether such an occurrence is a chance finding or has a pathogenic basis, remains to be determined. This article is presented to create awareness among clinicians and pathologists regarding an unusual concurrence of rare gluteal extraskeletal chondroma with sporadic neurofibroma.
[1]. EB Chung, FM Enzinger, Chondroma of soft partsCancer 1978 41:1414-24. [Google Scholar]
[2]. MJ Kransdorf, JM Meis, From the archives of the AFIP. Extraskeletal osseous and cartilaginous tumours of the extremitiesRadiographics 1993 13:853-84. [Google Scholar]
[3]. T Yasuoka, Y Handa, F Watanabe, N Oka, Chondroma of the tongue. Report of a case Journal of Maxillofacial Surgery 1984 12:188-91. [Google Scholar]
[4]. MB Aslam, MT Haqqani, Extraskeletal chondroma of parotid glandHistopathology 2006 48:465-67. [Google Scholar]
[5]. JY Han, HS Han, YB Kim, JM Kim, YC Chu, Extraskeletal chondroma of the fallopian tubeJ Korean Med Sci 2002 17:276-78. [Google Scholar]
[6]. Y Choi, WS Lim, AY Lee, SH Lee, Extraskeletal chondroma of the scalp: an atypical location Indian J Dermatol Venereol Leprol 2013 79:435-36. [Google Scholar]
[7]. VJ Ekanem, II Adeoye, TT Marchie, Recurrent Extra Skeletal Soft Tissue Chondroma in a Black African Female: Report of a Case and Review of LiteratureJournal of Medicine and Biomedical Research 2006 5(2):18-21. [Google Scholar]
[8]. KP Boyd, BR Korf, A Theos, Neurofibromatosis type 1J Am Acad Dermatol 2009 61:1-14. [Google Scholar]