Sarcomatoid Carcinoma of Anterior Maxilla: A Case Report and Immunohistochemical Analysis
Vishwaprakash Shetty1, Anshum Datta2, Nidhi Marya3, Sahil Handa4, Vishesh Yadav5
1 Professor & HOD, Department of Oral & Maxillofacial Pathology, SGT Dental College, Gurgaon, India.
2 PG Student, Department of Oral Pathology, SGT Dental College, Gurgaon, India.
3 Senior Lecturer, Department of Conservative & Endodontics, Rajasthan Dental College, Jaipur, India.
4 PG Student, Department of Preventive and Community Dentistry, SGT Dental College, Gurgaon, India.
5 PG Student, Department of Preventive and Community Dentistry, SGT Dental College, Gurgaon, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anshum Datta, Professor Colony, Andora Road, Amb distt. Una (H.P.)-177203, India.
E-mail: anshum.dentist@gmail.com
Sarcomatoid carcinoma is a rare and peculiar biphasic malignant neoplasm that occurs mainly in the upper aerodigestive tract. Sarcomatoid carcinoma is an unusual biphasic tumor composed of both malignant epithelial and malignant mesesnchymal component in association with, and usually dominated by, an abundant dysplastic-appearing spindle cells. This tumor consistently poses a significant diagnostic challenge to pathologists. Despite of several immunohistochemical, electron microscopic and genetic studies, precise histogenesis of sarcomatoid carcinoma is quite controversial. Here we are describing a case of sarcomatoid carcinoma in a 40 yr old male patient with special emphasis on immunohistochemical analysis. Here, we are describing a case of sarcomatoid carcinoma in a 40-year-old male who presented with a small swelling & pain in hard palate along with immunohistochemical analysis.
Biphasic, Cytokeratin, Immunohistochemistry, Spindle cell carcinoma, Vimentin
Case Report
A 40-year-old male patient reported to the Department of Oral & Maxillofacial Surgery, SGT Dental College & Research Institute, Gurgaon, with a chief complaint of swelling & pain in the right anterior palatal region since 4 months. Patient already visited a private practitioner for the same complaint one-month back. He gave the history of aspiration done by dentist but due to absence of pus in aspirate the dentist decided to excise the lesion. After 1 month, patient again noticed recurrence of the mass in same area. The medical and family history of the patient was non-contributory. Extra-orally there were no changes and no lymphadenopathy. On intraoral examination a well-defined, reddish mass was present on right anterior palatal region extending from 12 to 15. Lesion was measuring 3 x 4 cm in size. The overlying mucosa was reddish in appearance. On palpation, lesion was firm, tender, non-fluctuant and non compressible. Hyperplastic gingival papilla was also seen wrt 12 & 15 [Table/Fig-1].
Clinical picture of lesion on right anterior palatal region extending from 12 to 15

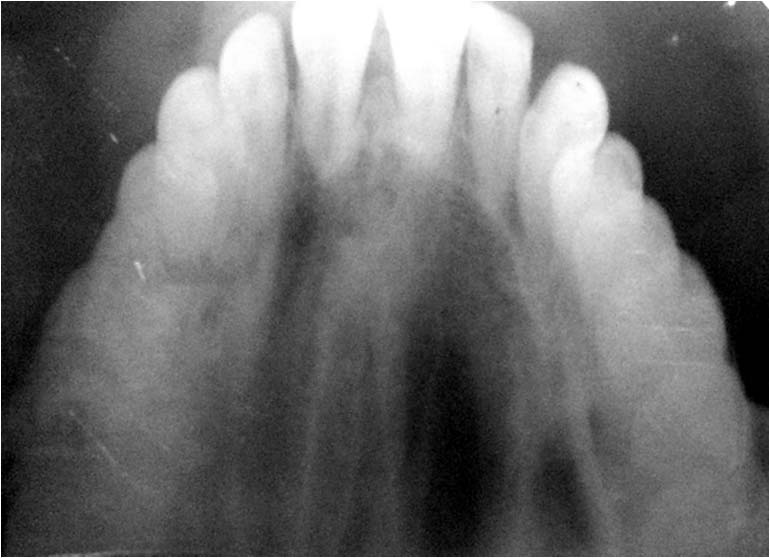
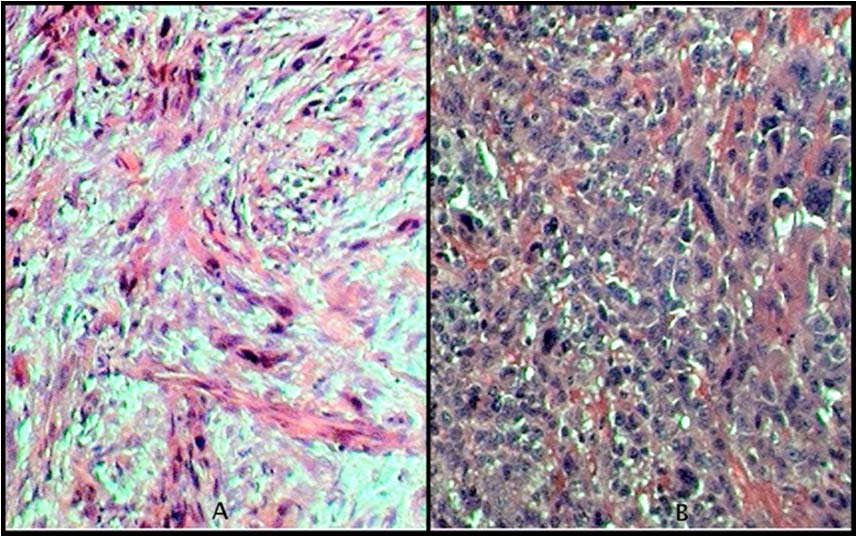
On radiographic examination, an ill defined radiolucency with destruction of trabecular pattern, widening of pdl space and break in the continuity of lamina dura is seen wrt 11,12,21. No evidence of root resorption resorption or displacement of the teeth was found [Table/Fig-2]. On the basis of clinical and radiographic examination a provisional diagnosis of pyogenic granuloma or oral malignancy was made. Later Incisional biopsy was performed and sent to Department of Oral and Maxillofacial Pathology for further examination. On histopathological examination it showed connective tissue stroma exhibiting sheets of atypical round and spindle shaped cells. The cells exhibited pleomorphism with altered nuclear cytoplasmic ratio, nuclear hyperchromatism, abnormal mitosis along with fibrovascular stroma & chronic inflammatory cell infilterate. The overlying epithelium was dysplastic stratified squamous type [Table/Fig-3]. Histopathologically, features were suggestive of Spindle cell carcinoma. For confirmatory diagnosis immunohistochemistry was adviced.
Ill defined radiolucency wrt 11,12 region
Connective tissue stroma showing sheets of atypical round and spindle shaped cells. (A)H& E stain 20x (B) H& E stain 40x
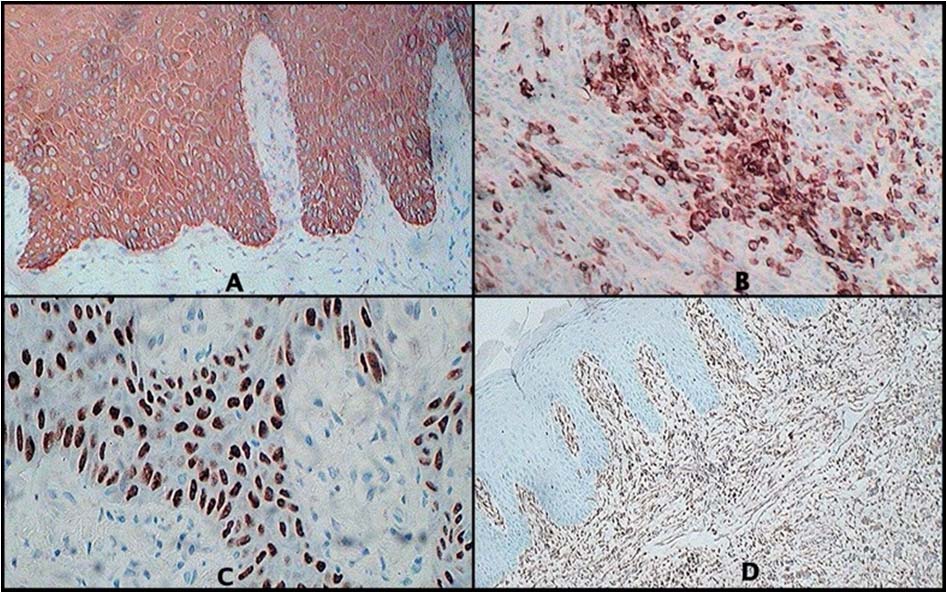
Immunohistochemical examination showed positivity for AE1/AE3 and EMA, pancytokeratin/CK 7, vimentin with focal individual cell immunoreactivity for CK 5 and 6. The tumour is immunonegative for Ck14, smooth muscle actin, desmin, CD31, CD34, S100 protein, HMWCK [Table/Fig-4]. All laboratory investigations carried out and found to be within normal limits before surgical procedure. Patient underwent segmental resection (hemi-maxillectomy) under general anesthesia in the Department of Oral & Maxillofacial Surgery of right side of maxilla measuring approx. 2.5x2.5cm extending from 12 to 15 [Table/Fig-5,6]. The patient was kept on a regular follow-up. He was free of any complication after 8 months of surgical resection.
Immunohistochemistry showing Spindle-shaped cells positive for (A) Cytokeratin 5&6 (B) Cytokeratin 7 (C) p63 & (D) Vimentin
Intra-operative image showing hemi-maxillactomy extending from 12 to 15

Postoperative image of patient

Discussion
Sarcomatoid carcinomas are biphasic tumour that exhibits prominent spindle cell morphology. It is a rare variant of SCC, which has both malignant squamous cells, and malignant spindle cells of epithelial origin. The histologic transition from squamous cells to spindle cells has been recognized in some cases with ultrastructural examinations showing transition from cells with epithelial features to those with increasingly more mesenchymal characteristics [1]. It has been linked to cigarette smoking, alcohol abuse, and previous radiation exposure to the affected area [2].
In the present case a differential diagnosis of pyogenic granuloma, periapical abscess or giant cell granuloma was given on the basis of clinical examination. This might be the reason for the excision of lesion by private practitioner. But on radiographical examination due to presence of radio-opacity with ill-defined margins it can be differentially diagnosed as osteomyelitis, osteonecrosis, odontogenic tumour or any metastatic tumour. Histopathologically the microscopic features show two-distinct epithelial-derived components: a carcinomatous component showing dysplastic features and sarcomatoid spindle cell component. Both these features were evident in sarcomatoid carcinoma. So a final diagnosis of Sarcomatoid carcinoma was given and later confirmed with immunohistochemistry.
Immunohistochemically the most sensitive and reliable epithelial markers to be used for demonstration of the epithelial phenotype are keratin (AE1/AE3) and epithelial membrane antigen. AE1 / AE3 and EMA, on the spindle cell component, can be useful in the differential diagnosis of Sarcomatoid carcinoma with other sarcomatous lesions [2]. It is important to remember that SpCC should not be ruled out of the differential diagnosis by a positive reaction for vimentin in sarcomatoid tumour cells. Absence of staining for keratin in the sarcomatoid tumour cells does not always exclude SpCC because some SpCC show immunoreactivity of keratin in their sarcomatoid components only with some anti-keratin antibodies. Different kinds of anti-keratin antibodies should be applied in the differential diagnosis of SpCC. IHC analysis of this case shows expression of cytokeratin (CK) and vimentin to various degrees. In this study Pan cytokeratin has been used which includes wide range of cytokeratin antibodies.
The vimentin positivity reflects that these bizarre fibroblast-like cells are carcinoma cells with true mesenchymal metaplasia. The results may indicate that these cells have acquired mesenchymal properties both morphologically and functionally through metaplastic changes and simply correlated to the concept of a malignant epithelial cell undergoing alterations, resulting in a loss of keratin and acquiring vimentin as the cytoskeleton protein. Along with these p63 has also been reported as a useful marker for spindle cell carcinoma [1].
Prakash et al., also reported a case of spindle cell carcinoma. All necessary investigations were done to reach the final diagnosis. To confirm the diagnosis, immunohistochemistry was performed. They found that the epithelial cells were strongly positive for cytokeratin and the spindle cells were focally positive for cytokeratin and epithelial membrane antigen [3].
Although it is difficult to predict biologic behavior in every case, patients whose tumours are deeply invasive tend to have a poor prognosis, whereas those with early-stage tumours usually have an excellent prognosis. Distant metastases and depth of tumour invasion into underlying structures were found to be reliable prognostic features, together with their polypoid configuration [4].
Conclusion
Sarcomatoid carcinomas will continue to be diagnostically challenging for the surgical pathologist. Due to limited number of studies in literature related to sarcomatoid carcinoma, the exact pathogenesis, clinical behavior, and long-term prognosis with a systematic approach is critical for its accurate diagnosis which also aids in correct patient management.
[1]. Su HH, CHU ST, Hou YY, Chang KP, Chen CJ, Spindle cell carcinoma of oral cavity and oropharynx: Factors affecting outcomeJ Chin Med Assoc 2006 69(10):478-83. [Google Scholar]
[2]. Parikh N, Desai N, Spindle Cell Carcinoma of the oral cavity: A case report of a rare entity and review of literatureJ. Academy Adv Dental Research 2011 2(2):31-6. [Google Scholar]
[3]. Prakash N, Kumar H, Sharada P, Pradeep GL, Spindle cell carcinoma of the oral cavity: a case report of a rare entity and review of literatureWorld Journal Of Dentistry 2010 1(1):55-8. [Google Scholar]
[4]. Cardesa A, Zidar N, World Health Organization Classification of TumoursHead and Neck Tumours: Oral Cavity and Oropharynx 2005 LyonIARC Press:127-28. [Google Scholar]