Uncommon Surgical Causes Of Right Lower Quadrant Pain In Children. Single Center Experience.
Vassilis Lambropoulos1, Irene Papageorgiou2, Chrysostomos Kepertis3, Dimitrios Sfoungaris4, Ioannis Spyridakis5
1Pediatric Surgeon, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital “PAPAGEORGIOU”, Thessaloniki, Greece.
2Resident, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital “PAPAGEORGIOU”, Thessaloniki, Greece.
3Pediatric Surgeon, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital “PAPAGEORGIOU”, Thessaloniki, Greece.
4Assistant Professor, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital “PAPAGEORGIOU”, Thessaloniki, Greece.
5Assistant Professor, Chief of the Department of Pediatric Surgery 2nd Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital “PAPAGEORGIOU”, Thessaloniki, Greece.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vassilis Lambropoulos, General Hospital “Papageorgiou” Ring Road Efkarpia-Thessaloniki-56403, Greece.
E-mail: vasslamb@hotmail.com, kepertis@otenet.gr
Right lower quadrant pain is one of the major reasons of children reference at the emergency department. The most common surgical cause, which needs appropriate management, is acute appendicitis. The purpose of this study is to reveal uncommon surgical causes found during surgery in children who were misdiagnosed as acute appendicitis in our department during the last 10 y. Data of patients who have undergone appendicectomy during a ten year period (since Feb 2004 until Mar 2014) were collected retrospectively. Eight hundred twenty children have undergone appendicectomy in our department. In six children another uncommon cause of the symptoms was revealed during surgery. In one patient the cause was a duplication cyst of the terminal ileum, in two patients an omental torsion, in one patient a meckel diverticulum torsion, in one patient a splenic rupture and in one patient a retroperitoneal tumor. All of the patients were successfully managed during the first operation. The possibility of other uncommon causes of right quadrant abdominal pain should always be kept in mind, especially when there is a negative appendicitis. However, the transaction of further paraclinical examinations – ultrasonography or computed tomography- preoperatively is under discussion. Nevertheless a thoroughly taken case history is undoubtedly always necessary.
Acute abdominal pain, Children, Duplication cyst, Meckel diverticulum torsion, Omental torsion
Case Report
A large number of young patients visit a pediatric emergency department complaining of right lower quadrant abdominal pain. In most cases the pain is due to a non surgical cause such as constipation, urinary infections, mesenteric lymphadenitis or virus infections of the gastrointestinal system. However, the most common surgical cause of this condition is acute appendicitis. Other relatively common surgical causes that are mentioned in the literature are conditions relevant to the female genitals and complications of the presence of meckel’s diverticulum. Coming to a safe conclusion according the diagnosis may sometimes be difficult and the decision of leading a patient to the surgery should be a matter of great consideration. During the last ten years in our department 820 children have undergone an operation for acute appendicitis. The decision for the majority of patients was taken through the main symptom which was the abdominal pain, the localized tenderness and the accompanying symptoms such as anorexia, nausea, vomiting and low fever. In six of those 820 patients the cause of the symptoms was proved to be a very uncommon condition, different of the surgical conditions that are usually mentioned throughout bibliography.
Case 1
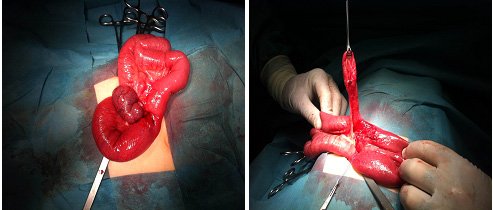
In the first case the young patient was a 9-year-old boy presented with the common symptoms of acute appendicitis. The plain abdominal X-ray which is a routine procedure in our department revealed no sign of intestinal obstruction. During surgery however a large ischemic meckel’s dicerticulum [Table/Fig-1,2] was found contorted around a string- a remnant of the omphalomesenteric duct. The diverticulum was excised but no intestinal excision was necessary and the postoperative course was uncomplicated for that patient.
Case 2
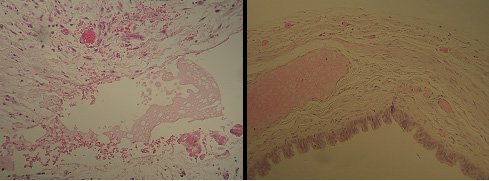
This case is referring to a 12-year-old boy who underwent an urgent operation as he came to our emergency department with an acute symptomatology of the lower abdomen, a combination of localized tenderness and intense rebound tendernes. The intraoperative findings were a normal appendix and a large extraperitoneal tumor which was totally excised by ligating the spermatic vessels and preserving the ipsilateral ureter. Histological examination showed that it was a non malignant pseudocyst, probably inflammatory, and the child didn’t require a second operation [Table/Fig-3,4]. Postoperative course was absolutely uncomplicated and follow up with an abdominal computed tomography three months after the excision revealed no pathological findings.
Case 3 and 4
The next two cases were of a 5-year-old and an 8-year-old boys. Both presented with abdominal pain, nausea and low fever. In both of them during operation hemorrhagic fluid was found into the peritoneal cavity and the appendix was normal. However, a thorough abdominal survey revealed a part of great omentum that was ischemic and necrotized due to omental torsion [Table/Fig-5]. The contorted omentum was excised and the peritoneal cavity was cleaned and drained. The postoperative course was normal for these two children.
Case 5
In the fifth case the patient was a 10-year-old boy who presented to our emergency department with the typical symptoms of right lower quadrant pathology. However laparotomy revealed hemorrhagic content in the abdominal cavity and a thorough control done after suction but without extending the incision showed no other pathological signs. Postoperatively a more detailed history was taken which exposed a blunt abdominal trauma that had taken place a week before. That detail led to the transaction of an abdominal computed tomography and a splenic rupture was found. The patient was managed conservatively as it is suggested and was dismissed a week after operation in a good general condition.
Case 6
Finally we present a case of a 9-year-old girl who was referred with a right lower quadrant symptomatology. A laparotomy was transacted with the diagnosis of acute appendicitis; therefore a terminal ileum duplication cyst was proved to be the reason of her symptoms [Table/Fig-6]. The cyst was removed through a limited excision of the terminal ileum with preservation of the ileocecal valve and a primary ileoileal anastomosis was done. In this case too the postoperative course was uneventful and the girl was dismissed on fifth postoperative day.
Discussion
Right-lower-quadrant (RLQ) abdominal pain is a common presentation in a pediatric emergency room, and acute appendicitis is the most common reason for urgent abdominal surgery in children [1]. The differential diagnosis for this symptom includes gastroenteritis, constipation, ovarian torsion, ovarian cyst, dysmenorrhea, ectopic pregnancy, tubo-ovarian abscess, nephrolithiasis, inflammatory bowel disease, and intussusceptions [1,2]. Most academic paediatric centers chose ultrasonography as the imaging choice for a patient with RLQ pain [3]. However, ultrasonography is an operator dependent examination. Overall the ultrasonography of abdomen was found to be diagnostic in 48% and supportive in further 18.6% [4]. In our center abdominal imaging with ultrasonography does not constitute a routine practice for the management of RLQ pain; it is transacted though in cases of female patients when a genital pathology is suspected. Regarding to the cases previously described it is not certain if an ultrasound would have been helpful for the diagnosis; nevertheless it is almost certain that those patients would have been operated anyway, even with a negative ultrasound, because of their acute symptomatology and signs of peritoneal irritation. It is obvious that finally only one of the presented patients underwent an unnecessary operation, the boy with the splenic rupture.
An abdominal computed tomography is obviously the most precise imaging choice for the investigation of the acute abdomen. However, because of the large amount of the radiation taken by the young patient and its relatively high cost, it cannot be used in every child presenting with abdominal pain. A carefully taken case history and a thorough clinical examination must suggest the cases where abdominal CT should be performed. It is possible that in the last case a more detailed history could help the patient to avoid the operation by leading to the performance of an abdominal CT before surgery.
All of the cases described before have something uncommon related to the diagnosis or the symptomatology. Talking about the first case the uncommon thing is not the presence of the diverticulum, but firstly the presence of the string and secondly the fact that despite the torsion and necrosis of the diverticulum the patient didn’t have any clinical or radiological signs of intestinal obstruction. Obviously preoperative diagnosis was difficult in that case and even if it had been done the management would be the same. As regards to the second patient the reason for the pain was proved to be a pseudocyst of unknown etiology and it was not clear why this tumor presented with an acute symptomatology. Primary omental torsion is a rare cause of the acute surgical abdomen in children. By 1981 fewer than 250 cases had been described in the literature, mostly in adults. Diagnostic imaging with ultrasonography and CT scanning may be useful but are not very reliable. Conservative treatment is an option for stable patients however it is a condition difficult to diagnose preoperatively and is usually detected during laparotomy for acute abdomen [5,6]. Finally, in the last case, the cause of the symptoms was a fetal remnant, a duplication cyst of the terminal ileum. Duplications of the GI tract are rare congenital anomalies and most reports in the literature are either case reports or small series. Localized duplications are common in the ileum and jejunum and can present with a variety of signs and symptoms [7-10]. In our case it presented with the symptoms of acute appendicitis. Excision was made during the same surgery along with appendicectomy and the patient required no further management.
Meckel’s diverticulum as it appears immediately after the reduction
Cyst wall without connective tissue epithelium, with fibroblastic reaction, relatively rich vascularization and scattered lymphocytic invasions
Torsion of the greater omentum

Terminal ileum duplication cyst

Conclusion
Acute appendicitis is undoubtfully the most common surgical cause of right lower quadrant pain in children. In rare cases however surgery leads to a surprise. It is obvious that in these cases the surgeon’s awareness and clinical suspicion is of great importance in order to find the real problem and give the right solution.
[1]. A Ross, NS LeLeiko, Acute abdominal painPediatr Rev 2010 31:135-44. [Google Scholar]
[2]. C Tejani, T Phatak, A Sivitz, Right Lower-Quadrant Pain-More Than One DiagnosisPediatr Emerg Care 2012 28(11):1224-26. [Google Scholar]
[3]. MM Abu-Yousef, Ultrasonography of the right lower quandrantUltrasound Q 2001 17:211-25. [Google Scholar]
[4]. B Balachandran, S Singhi, S Laln, Emergency Management of Acute Abdomen in ChildrenIndian J Pediatr 2013 80(3):226-34. [Google Scholar]
[5]. I Papageorgiou, A Hatzigeorgiadis, J Papadopoulos, K Andreou, K Blouhos, Always think about omental torsion when the appendix looks normalAm J Case Rep 2010 11:138-41. [Google Scholar]
[6]. C Kepertis, G Koutsoumis, Primary torsion of the greater omentumIndian Pediatrics 2005 42(1):613-14. [Google Scholar]
[7]. MH Atalar, L Cankorkmaz, H Ozer, G Koyluoglu, A huge duplication cyst of the ileumPol J Radiol 2013 78(3):70-73. [Google Scholar]
[8]. K Sakamoto, S Hasegawa, Y Yamazaki, T Makino, T Suda, T Imada, Ileal duplication presenting as perforation: report of a caseSurg Today 2000 30:445-47. [Google Scholar]
[9]. I Karnak, T Ocal, ME Senocak, FC Tanyel, N Buyukpamukcu, Alimentary tract duplications in children: report of 26 years’ experienceTurk J Pediatr 2000 42:118-25. [Google Scholar]
[10]. SC Tong, M Pitman, SA Anupindi, Best cases from the AFIP. Ileocecal enteric duplication cyst: radiologic-pathologic correlationRadiographics 2002 22:1217-22. [Google Scholar]