Aesthetic Rehabilitation of Subgingival Fractures with Forced Eruption: Case Reports
Juhi Ansar1, Prateek Jain2, Preeti Bhattacharya3, Deepak Kumar Agarwal4
1 Senior Lecturer, Department of Orthodontics and Dentofacial Orthopedics, Institute of Dental Sciences, Bareilly, India.
2 Jonior Resident, Department of Orthodontics and Dentofacial Orthopedics, Institute of Dental Sciences, Bareilly, India.
3 Professor, Department of Orthodontics and Dentofacial Orthopedics, Institute of Dental Sciences, Bareilly, India.
4 Professor, Department of Orthodontics and Dentofacial Orthopedics, Institute of Dental Sciences, Bareilly, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Juhi Ansar, Senior Lecturer, Department of Orthodontics and Dentofacial Orthopedics, Institute of Dental Sciences, Bareilly, India.
E-mail: Juhiortho10@gmail.com
Aesthetic rehabilitation of sub-gingival crown fractures of the maxillary anterior tooth present extreme challenges to the dental surgeon. The prognosis of traumatized tooth depends on accurate diagnosis and physiological status of the involved tooth. This paper discusses two different cases of subgingival fracture of maxillary anterior tooth that was managed by two different technique of forced eruption. After endodontic management and forced eruption, esthetic rehabilitation was completed by placing post and core, and all ceramic crown. The final result was successful and resulted in good esthetics and secured periodontal health.
Biological width, Orthodontic extrusion, Prosthetic restoration, Subgingival fracture
Case Report
In general practice, Dentist often encounter cases of subgingival fractures or grossly decayed tooth. A possible therapeutic option depends upon the clinical and radiographic status of the involved tooth. Treatment modalities either include extraction of fractured tooth followed by prosthetic rehabilitation or involve a multi–disciplinary approach including endodontics, periodontal crown lengthening or orthodontic extrusion followed by prosthetic rehabilitation. Problem associated with such fractures include compromised biologic width and inadequate remaining tooth structure for definite restoration. The prime objective of tooth extrusion or forced eruption is to provide both a sound tissue margin for definitive restoration and to create a periodontal environment (biological width) that will be easy for the patient to maintain [1]. The purpose of this paper is to discuss two different cases in which traumatized tooth was treated endodontically and extruded using two different technique of forced eruption.
Case Report 1
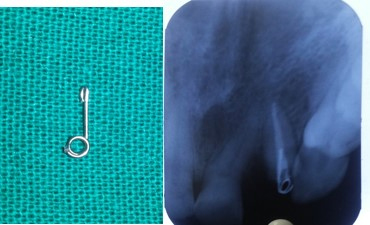
A 35-year-old female was referred to our Department of Orthodontic by her Endodontist, with a chief complaint of fractured maxillary right lateral incisor. Clinically no visible crown structure was seen and radiographic examination confirmed intact root with no periapical pathology [Table/Fig-1]. On the basis of clinical and radiographic findings a diagnosis of crown root fracture was made. As the patient was not ready for extraction, orthodontic extrusion of tooth segment was planned to allow sufficient tooth area available for core build up and crown preparation. As no visible crown structure was seen for bonding attachment, a helical pin fabricated from 23 gauze stainless steel wire was inserted into the prepared canal along with the thermo plasticised obturating material [Table/Fig-2]. A modified arch wire was designed such that more vertical activation could be achieved. The extrusive force of about 35 gm was delivered with the help of elastic threads, which were replaced every 15 days until 3 mm of extrusion was achieved [Table/Fig-3]. Prosthetic rehabilitation was done with composite after the tooth had been sufficiently extruded [Table/Fig-4]. Follow up photograph of the patient shows stable tooth position [Table/Fig-5].

Helical pin and radiograph



Case Report 2
A 20-year-old male patient was referred to the Department of Orthodontics by her Endodontist. The chief complaint of the patient was fractured maxillary left central incisor. Clinical examination showed horizontal coronal fracture of upper left central incisor with exposed pulp tissue. Around 2 mm of the buccal tooth structure was intact without any mobility. Radiographic examination revealed failed root canal therapy and a fully formed apex without any periapical lesion [Table/Fig-6]. Patient was given the option of extraction or a multi–disciplinary treatment. Patient opted for the latter. With patient’s consent, root canal therapy was carried out, and orthodontic extrusion was planned subsequently. As bonding area was insufficient, a small segment of wire was attached directly to tooth surface with composite [Table/Fig-7]. Extrusive force of about 35 gm was applied by elastic thread until desired extrusion of 4 mm was achieved [Table/Fig-8]. Finally the tooth was restored prosthodontically, with a post and core, and porcelain crown [Table/Fig-9]. Eight weeks later, after placement of permanent crown, the upper left central incisor showed stable result [Table/Fig-10].


Post Extrusion Intraoral and Radiograph



Discussion
Extensive caries or crown fracture may create a situation where placement of the restoration may be difficult. The major problem with subgingival fracture is absence of adequate coronal ferrule and a compromised biological width. Ingber suggested that a Minimum distance of 3 mm is required from the restorative margin to the alveolar crest to permit adequate healing and restoration of the tooth [2]. Orthodontic extrusion is also indicated in angular bone defects, isolated periodontal pockets [3] and in patients when surgical extraction is contraindicated (e.g., in patients receiving chemotherapy or radiotherapy) [4].
If the fracture line is positioned below free gingival margin and, if the length of the root is sufficient, then the root can be endodontically treated and orthodontically extruded above the gingival margin. This procedure enables more favorable prosthodontic coronal restoration by preserving a good periodontal tissue health [5]. The movement of the teeth in the direction of eruption in the absence of gingival inflammation leads to elongation of periodontal fibres and also deposition of bone at the alveolar crest [6].
Several extrusion techniques are available, depending on the clinical conditions encountered. Fixed and removable orthodontic appliances can be used for extrusion, which include conventional fixed appliances, section fixed appliances, and removable plates.A fixed orthodontic appliance require minimal patient co-operation and is well tolerated by the patient. Orthodontic brackets can be directly placed on the buccal aspect of the tooth to be extruded. If the dental tissue is inadequate for bonding bracket, traction can be applied from attachment inserted into the prepared canal of the tooth after endodontic therapy [7].
Authors have recommended that the maximum force for a slow movement should not exceed 30 gm, whereas for rapid extrusions, forces higher than 50 gm are applied [8,9]. After a latency period of a few days to a few weeks, including a period of hyalinization, slow extrusion occurs at a rate of approximately 1 mm or less per week [8]. Brown and Welbury reported that in practice there is always some movement of the surrounding bone and gingival tissue when the tooth is extruded, but these changes were less prominent when the extrusion was carried out with light forces and at a slower rate [10]. Prior to final restoration, it is important to retain the root in its new position to prevent relapse [11]. Authors have also recommended circumferential supracrestal fibrotomy around the exposed tooth after orthodontic extrusion to cut the stretched periodontal fibers and prevent relapse [12,13]. In the present cases, slow orthodontic extrusion was performed using different techniques of forced eruption. Follow up of patients’ showed good periodontal health and stable result.
Although orthodontic extrusion requires a prolonged treatment time [10], this treatment is preferred over crown lengthening which removes alveolar bone and may become the reason for pocket formation [14]. However, other risk associated with this technique like ankylosis, root resorption, mobility and relapse may result in failure of treatment. The informed consent form must be obtained from patient before going for orthodontic extrusion.
Calikan et al., [15] instead of performing orthodontic extrusion and fibrotomy suggested alternative treatment of crown root fracture. They extruded the tooth surgically by conventional extraction and then stabilized it in the new position. This procedure is more traumatic as it requires extraction of tooth and then repositioning. Although orthodontic forced eruption requires more visits than surgical extrusion, it is considered to be a better option because orthodontic forces allow the biological way of erupting the tooth, with no removal of alveolar bone and better final aesthetics [13].
Conclusion
Different clinical techniques can be employed for orthodontic extrusion depending on the scenario of the case. A multidisciplinary approach is necessary for the restoration of tooth fractured at subgingival level. In these case reports placement of the final restoration after orthodontic extrusion resulted in good esthetics and function postoperatively.
[1]. Mittal R, Gupta S, Singla A, Gupta A, Managing sub–gingival fracture by multi–disciplinary approach: Endodontics–forced orthodontic extrusion and prosthetic rehabilitationSaudi Endodontic Journal 2013 3(2):82-86. [Google Scholar]
[2]. Ingber JS, Rose LF, Coslet JG, The “biologic width”: A concept in periodontics and restorative dentistryAlpha Omegan 1977 70:62-65. [Google Scholar]
[3]. Mantzikos T, Shamus I, Case report: forced eruption and implant site developmentAngle Orthod 1998 68(2):179-86. [Google Scholar]
[4]. Buskin R, Castellon P, Hochstedler JL, Orthodontic extrusion and orthodontic extraction in preprosthetic treatment using implant therapyPract Periodontics Aesthet Dent 2000 12(2):213-19. [Google Scholar]
[5]. Bielicka B, Bartkowiak M, Urban E, Tomasz M, Holistic Approach in the Management of Subgingivally Fractured Premolar Tooth – Case ReportDent. Med Probl 2008 45(2):211-14. [Google Scholar]
[6]. Bach N, Baylard JF, Voyer R, Orthodontic extrusion: Periodontal considerations and applicationsJ Can Dent Assoc 2004 70:775-80. [Google Scholar]
[7]. Durham TM, Goddard T, Morrison S, Rapid forced eruption: a case report and review of forced eruption techniquesGen Dent 2004 52(2):167-75. [Google Scholar]
[8]. Minsk L, Orthodontic tooth extrusion as an adjunct to periodontal therapyCompend Contin Educ Dent 2000 21(9):768-70.:72:74 [Google Scholar]
[9]. Bondemark L, Kurol J, Hallonsten AL, Andreason JO, Attractive magnets for orthodontic extrusion of crown-root fractured teethAm J Orthod Dentofacial Orthop 1997 112(2):187-93. [Google Scholar]
[10]. Brown GJ, Welbury RR, Root extrusion, a practical solution in complicated crown–root incisor fracturesBr Dent J 2000 189:477-78. [Google Scholar]
[11]. Ingber JS, Forced eruption: Alteration of soft tissue cosmetic deformitiesInt J Periodontics Restorative Dent 1989 9:416-25. [Google Scholar]
[12]. Arhun N, Arman A, Ungor M, Erkut S, A conservative multidisciplinary approach for improved aestheticresults with traumatized anterior teethBr Dent J 2006 201:509-12. [Google Scholar]
[13]. Poi WR, Cardoso Lde C, de Castro JC, Cintra LT, Gulinelli JL, de Lazari JA, Multidisciplinary treatment approach for crown fracture and crown root fracture – A case reportDent Traumatol 2007 23:51-55. [Google Scholar]
[14]. Heda CB, Heda AA, Kulkarni SS, A multi-disciplinary approach in the management of a traumatized tooth with complicated crown-root fracture: A case reportJ Indian Soc Pedod Prev Dent 2006 :197-200. [Google Scholar]
[15]. Calişkan MK, Türkün M, Gomel M, Surgical Extrusion of Crown–Root–Fractured Teeth: A Clinical ReviewInt Endod J 1999 32:146-51. [Google Scholar]