A Study on Prevalence of Phenyl Thiocarbamide (PTC) Taste Blindness Among Obese Individuals
Deepika Veluswami1, B Ambigai Meena2, S. Latha3, I. Gayathri Fathima4, K Soundariya5, K Senthamil Selvi6
1 Assistant Professor, Department of Physiology, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India.
2 Professor, Department of Obstetrics and Gynecology, Sree Lakshmi Narayana Institute of Medical Sciences, Puducherry, India.
3 Assistant Professor, Department of Physiology, Sree Lakshmi Narayana Institute of Medical Sciences, Puducherry, India.
4 Assistant Professor, Department of Physiology, Sree Lakshmi Narayana Institute of Medical Sciences, Puducherry, India.
5 Associate Professor, Department of Physiology, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India.
6 Assistant Professor, Department of Physiology, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepika V, Assistant Professor, Department of Physiology, Sri Manakula Vinayagar Medical College and Hospital, Kalitheerthalkuppam, Puducherry – 605107, India.
E-mail: deepy843@gmail.com
Introduction
Taste blindness to the phenylthiocarbamide (PTC) is an inherited trait that is shown to influence our food and dietary preferences which in turn influence our body weight. Obesity is a global epidemic issue known to be on rise among the developing countries. Relating taste perception to obesity, the present study was undertaken to assess the prevalence of phenylthiocarbamide (PTC) taste blindness among obese individuals.
Materials and Methods
Three hundred and fifty individuals of age group 20-40 y were recruited from the local community for the present cross sectional study. Anthropometric measurements were taken and BMI was calculated. Subjects were classified as underweight, normal, overweight and obese based on their BMI. Normal, overweight and obese individuals were then asked to taste the commercially available PTC test papers and classified as non tasters and tasters of PTC.
Results
Out of 350 individuals, mean age group of 30±6.02 y, based on their BMI they were divided into 4 groups, Group A-underweight (16%), Group B-normal (35%), Group C-overweight (28%) and Group D-obese (21%) individuals. In group B, 28% were non tasters of PTC and 65% were tasters. In group C, 82% were non tasters and 13% were tasters and in Group D, 81% were non tasters and 19% were tasters of PTC. The PTC non taster phenotype individuals showed higher BMI as compared with the tasters’ phenotype.
Conclusion
Exploring the novel connections between taste perception and obesity would help us to gain a control over the global epidemic-Obesity, which is the crux factor for various other health problems. The study advocates the usage of PTC tasting as a reliable indicator of weight gain susceptibility.
Diet, Obesity, Taste perception
Introduction
The world health organization has described obesity as an escalating global epidemic [1] and a major nutritional problem in developing countries, affecting a substantial number of adults and resulting in an amplified burden of chronic diseases [2]. In India, 5% of the total population is affected by obesity [3]. Various studies from South India report an alarming increase in overweight and obesity among children [4–6]. The fundamental cause for obesity is overconsumption [7] and research indicates that the taste perception is altered in obese individuals, which in turn affect their consumption [8]. Understanding the associations between taste perception and obesity would help us to cope up with obesity, which is known to be the crux factor for myriad of medical health problems. Gustatory sense informs the body about the quality of ingested food. Sweet, sour, salty, bitter, and umami are documented as the basic taste stimuli. Bitter taste is aversive and identifies potentially harmful compounds to avoid [9]. It is found that obese individuals have significantly lower taste perception for salt, umami and bitter taste modalities as compared to non obese individuals [10].
A bitter chemical, phenylthiocarbamide (PTC), serendipitously discovered by Fox [11] has been widely used for various genetic and anthropological studies [12]. PTC, also known as Phenylthiourea (PTU) is an organosulfurthiourea containing a phenyl ring and possesses the chemical group N-C=S which is responsible for its characteristic bitter taste [13]. Glucosinolate compounds that occur naturally in cruciferous vegetables (broccoli, Brussels sprouts, cabbage, and kale) share this chemical grouping [14] and, in addition, a common taste quality: bitterness. Individuals with lower PTC taste thresholds appear to have more food dislikes than do less-sensitive individuals [15] and preference for sweet and high-fat food was observed to decrease with increasing perception of bitter taste [16].
PTC has remarkable property that some individuals report it to be incredibly bitter while others describe it to be tasteless, depending on the presence or absence of the PTC gene. The taste insensitivity to PTC is inherited as a Mendelian recessive trait [17] wherein the individuals with two recessive alleles (tt) are considered as “non tasters” for PTC and individuals with one dominant allele (Tt) or two dominant alleles (TT) are regarded as “tasters” for PTC. Genetic taste sensitivity may account for the development of dietary patterns and by extension, weight differences among individuals. PTC can be used as a genetic marker for gaining insight into individual’s risk of predisposition to obese trait. Vast genetic and molecular literature persist linking PTC tasting to various medical problems but data regarding prevalence of PTC taste blind status and obesity is insufficient and contradictory. Hence, the present study is based on the hypothesis that the PTC non-taster phenotype would be associated with higher BMI.
Materials and Methods
The cross-sectional study consisted of 350 individuals of age group 20-40 years, recruited from Madagadipet, Puducherry, India through house visits during the year 2012-2013. Written informed consent was obtained from all subjects and the protocol was approved by the Human Research Ethics committee.
The body weight was measured without shoes using a weighing scale, and height to the nearest centimeter was measured. Body Mass Index (BMI) was calculated as weight in kilograms divided by height (in meter squared). The subjects were classified into one of the four categories [18] as follows:
Group A –underweight individuals - BMI < 18.5 kg/m2;
Group B-normal individuals –BMI 18.5 to 24.9 kg/m2
Group C-overweight individuals– BMI 25 to 29.9 kg/m2;
Group D-obese individuals – BMI >= 30 kg/m2.
Selected normal, overweight and obese candidates were asked to describe the taste of commercially available PTC-impregnated test papers. Participants rinsed their mouth with water, and the paper was kept in the middle of their tongue. After tasting, they were asked “Do you taste anything?” If their response was no, they were classified as non- tasters that is they were regarded as taste blind to PTC. If they responded that it tasted bad or bitter, they were classified as tasters. If they responded ambiguously were retested later.
Statistical Analysis
Data entry and statistics were performed using the Microsoft Excel and results were expressed in percentages.
Result
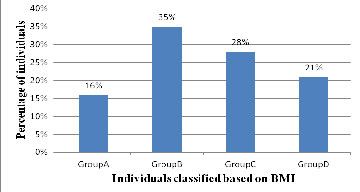
Out of 350 individuals, with mean age group of 30±6.02 years, based on BMI, [Table/Fig-1] Group A included 16% (56) of underweight individuals, Group B included 35% (123) normal subjects, Group C with 28% (97) of overweight individuals and Group D included 21% (74) of obese individuals.
Percentage distribution of individuals belonging to four groups
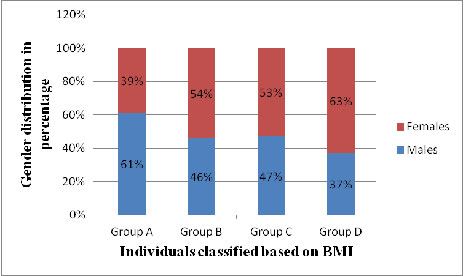
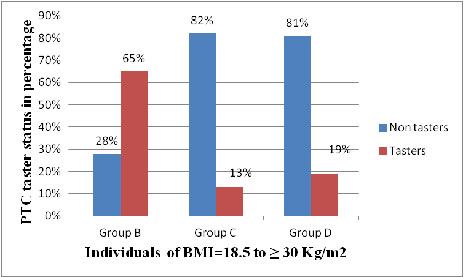
The percentage distribution of males and females included under the four groups. Among the 35% normal candidates (54% females and 46% males) 28% were non tasters of PTC, 65% were tasters and 6% of individuals provided an ambiguous response. Among 28% overweight individuals (53% females and 47% males) 82% were non tasters, 13% were tasters and 4% individuals provided an ambiguous response. Out of 21% obese candidates (63% females and 37% males), 81% were non tasters and 19% were tasters of PTC [Table/Fig-2].
Percentage distribution of males and females among the four groups
The prevalence rate of non taster and taster phenotype among normal, overweight and obese individuals is represented in. It indicates that non taster phenotype prevalence is increased among overweight and obese individuals as compared to their normal counterparts [Table/Fig-3].
Prevalence of non taster (NT) and taster (T) status among Group B (normal), group C (overweight) and group D (obese)
Discussion
In this study, we found that the prevalence rate of taste blindness to PTC among obese individuals was higher compared to normal individuals. The prevalence of taste blindness among normal individuals was 28% and among obese individuals it was reported to be 81%. Our study supports the findings that a strong correlation exists between non tasters and obesity [19]. It is reported that the prevalence of PTC taster trait is high in case of non obese children when compared to overweight/ obese [20]. Additionally fast/junk foods are low in fiber, micronutrients and antioxidants which are responsible for weight gain [21].
The possible mechanism involved has genetic background, stating that the bitter taste receptors are encoded by 25-30 TAS2R genes, located on chromosomes 12p13, 7q34, and 5p15 [22]. The ligand specificity of TAS2Rs appears to be quite broad, consistent with their roles in detecting several bitter-tasting compounds [23]. One of these, TAS2R38 has been extensively characterized in human populations, and is responsive to the bitter stimuli of PTC. Single nucleotide polymorphisms (SNP) located within a linkage disequilibrium block of these genes account for the association of taste, food preference and increase in weight [23]. It is found that the tasters are also better in discriminating between high and low fat foods. Also in our study, we found more non tasters who are overweight/ obese compare to taster, which again lays emphasis on the choice of food and its relation with obesity.
Anatomical studies reported that tasters actually have more taste buds than non tasters [24] and another study has showed positive relationship between the bitter perception to the number of fungiform papillae [25] present on the anterior surface of tongue.
6-n propylthiouracil (PROP), a compound structurally and chemically similar to PTC is also being extensively studied. It is shown that PROP non-tasters showed higher preferences for dietary fat (such as full-fat milk, high-fat salad dressings and sweet-fat dairy mixtures) [16,26,27] and consumed more servings of discretionary fats and high-energy foods per day than did tasters [27,28]. Finally, PROP tasters gave higher taste intensity ratings for linoleic acid, an essential polyunsaturated fatty acid, compared with PROP non-tasters [29].
Interestingly, a recent study reported that normal weight non-tasters of PROP compared to normal weight super-tasters, had lower circulating levels of both anandamide and 2-arachidonoylglycerol suggesting that lower levels of circulating endocannabinoids may counteract the tendency of non-tasters to overeat as a consequence of their higher disinhibition, (defined as a loss of control over eating in response to various types of stress and negative emotional states). Thus, the differences in endocannabinoid levels between super-tasters and non-tasters may represent a mechanism to regulate energy intake and normalize impaired feeding behavior [30].
Hence this study indicates that a greater percentage of non tasters are obese/overweight individuals, and thus are the high risk candidates prone for development of enormous non communicable diseases in future.
Conclusion
This study implies that inherited sensitivity to bitter thiourea compounds, a stable and reliably measured trait, influences weight status in humans. Current studies raise more questions than they answer about the prospective role for genetic taste factors in medical health and disease, and the exact nature of this relationship remains to be elucidated. An improved understanding of the genetic basis of taste, including identification of the associated genes and DNA markers, will hasten up evolution in the field.
Hence, this simple PTC screening test could ultimately be used as part of a battery of tests to identify vulnerability factors and prevent obesity development and implement interventions and programs as early as possible.
[1]. Rohilla R, Rohilla J, Verma M, Adolescent obesity: a silent epidemicInternational Journal of Basic and Applied Medical Sciences 2013 3(2):320-24. [Google Scholar]
[2]. World Health Organization. Preventing chronic diseases: A vital investment. World Global Report. Geneva: World Health Organization; 2005 [Google Scholar]
[3]. Kumar NVRTP, Mohanta GP, Manna PK, Manavalan R, Body mass index-a diagnostic tool to assess obesityIndian Journal of Pharmacy Practice 2008 2:81-83. [Google Scholar]
[4]. Raj M, Sundaram KR, Paul M, Deepa AS, Kumar RK, Obesity in Indian children: time trends and relationship with hypertensionNatl Med J India 2007 20:288-93. [Google Scholar]
[5]. Kotian MS, Kumar GS, Kotian SS, Prevalence and Determinants of Overweight and Obesity among Adolescent School Children of South Karnataka, IndiaIndian J Community Med 2010 35:176-78. [Google Scholar]
[6]. Laxmaiah A, Nagalla B, Vijayaraghavan K, Nair M, Factors affecting prevalence of overweight among 12 to 17-year-old urban adolescents in Hyderabad, IndiaObesity (Silver Spring) 2007 15:1384-90. [Google Scholar]
[7]. Ackroff K, Bonacchi K, Magee M, Yiin YM, Graves JV, Sclafani A, Obesity by choice revisited: effects of food availability, flavor variety and nutrient composition on energy intakePhysiol Behav 2007 92:468-78. [Google Scholar]
[8]. Bartoshuk LM, Duffy VB, Hayes JE, Moskowitz HR, Snyder DJ, Psychophysics of sweet and fat perception in obesity: problems, solutions and new perspectivesPhilos Trans R Soc Lond B Biol Sci 2006 361:1137-48. [Google Scholar]
[9]. Lindemann B, Taste receptionPhysiol Rev 1996 76:718-66. [Google Scholar]
[10]. Overberg J, Hummel T, Krude H, Wiegand S, Differences in taste sensitivity between obese and non-obese children and adolescentsArch Dis Child 2012 97:1048-52. [Google Scholar]
[11]. Fox AL, Taste blindnessScience 1931 73:14 [Google Scholar]
[12]. Kim V, Jorgenson E, Coon H, Leppert M, Risch N, Drayna D, Positional cloning of the human quantitative trait locus underlying taste sensitivity to phenylthiocarbamideScience 2003 299:1221-25. [Google Scholar]
[13]. Drewnowski A, Rock CL, The influence of genetic taste markers on food acceptanceAm J Clin Nutr 1995 62:506-11. [Google Scholar]
[14]. Kalmus H, Genetics of taste. In: Beidler LM, edHandbook of sensoryphysiology 1971 Vol 4(2)New YorkSpringer-Verlag:165-79. [Google Scholar]
[15]. Fischer R, Griffen F, “Taste blindness” and variations in taste threshold in relation to thyroid metabolismJ Neuropsychol 1961 3:98-104. [Google Scholar]
[16]. Duffy VB, Bartoshuk LM, Food acceptance and genetic variation in tasteJ Am Diet Assoc 2000 100:647-55. [Google Scholar]
[17]. Merton BB, Taste sensitivity to PTC in 60 Norwegian families with 176 children. Confirmation of the hypothesis of single gene inheritanceAda Genet 1958 8:114-28. [Google Scholar]
[18]. CDC growth charts: United States Advance data from vital and health statistics. No.314 National Center for Health Statistics: Atlanta. 2000 [Google Scholar]
[19]. Shivaprasad HS, Chaithra PT, Kavitha P, Malini SS, Role of Phenylthiocarbamide in predicting the predisposition of disease traits in humansJ Nat Sc Biol Med 2012 3:43-47. [Google Scholar]
[20]. Saraswathi YS, Najafi M, Vineeth VS, Kavitha P, Suttur S, Malini SS, Association of phenylthiocarbamide taste blindness trait with early onset of childhood obesity in MysoreJournal of Paramedical Sciences (JPS) Autumn 2011 2(4):6-11. [Google Scholar]
[21]. Bevely J, Tepper BJ, 6 n-Propylthiouracil: A genetic marerfor taste with Implication for Food Preference and dietary habitsAm J Hum Genet 1998 63:1271-76. [Google Scholar]
[22]. Grimm ER, Steinle NI, Genetics of eating behavior: established and emerging conceptsNutrition Reviews 2011 69(1):52-60. [Google Scholar]
[23]. Sausenthaler S, Rzehak P, Wichmann HE, Heinrich J, Lack of relation between bitter taste receptor TAS2R38 and BMI in adultsObesity (Silver Spring) 2009 17:937-38. [Google Scholar]
[24]. Volkers N, Gene For Bitter Taste Could Be Due To Smoking And Eating BehaviorInteli Health News Service 2003 [Google Scholar]
[25]. Hayes JE, Bartoshuk LM, Kidd JR, Duffy VB, Supertasting and PROP bitterness depends on more than the TAS2R38 geneChemical Senses 2008 33:255-65. [Google Scholar]
[26]. Hayes JE, Duffy VB, Revisiting sugar-fat mixtures: Sweetness and creaminess vary with phenotypic markers of oral sensationChem Senses 2007 32:225-36. [Google Scholar]
[27]. Keller KL, Steinmann L, Nurse RJ, Tepper BJ, Genetic taste sensitivity to 6-n-propylthiouracilinfluences food preference and reported intake in preschool childrenAppetite 2002 38:3-12. [Google Scholar]
[28]. Tepper BJ, Neilland M, Ullrich NV, Koelliker Y, Belzer LM, Greater energy intake froma buffet meal in lean, young women is associated with the 6-n propylthiouracil (PROP) non-taster phenotypeAppetite 2011 56:104-10. [Google Scholar]
[29]. Ebba S, Abarintos RA, Kim DG, Tiyouh M, Stull JC, Movalia A, The examination of fatty acid taste with edible stripsPhysiol Behav 2012 106:579-86. [Google Scholar]
[30]. Tepper BJ, Banni S, Melis M, Crnjar R, Barbarossa IT, Genetic Sensitivity to the Bitter Taste of 6-n-Propylthiouracil (PROP) and Its Association with Physiological Mechanisms Controlling Body Mass Index (BMI)Nutrients 2014 6:3363-81. [Google Scholar]