Mandibular foramen marks place of entry of inferior alveolar neurovascular bundle into the mandible. Mandibular foramen can be subject to injury during a vast spectrum of surgical procedures which involves ramus of mandible such as orthognathic surgery, pre-prosthetic surgery, vertico-sagittal osteotomy, mandibular trauma management, and treatment of benign and malignant tumours. The provision of dental treatment depends on achieving excellent local anaesthesia. There may be failure of inferior alveolar nerve block due to improper evaluation of location of mandibular foramen resulting in painful treatment procedures to the patient with obvious discomfiture to the operator [1]. The location of mandibular foramen shows considerable variation among different population, in different ages and even within the same individual on two sides. These variations occur due to craniofacial growth and anatomic variability [2]. Hence, mandibular foramen should be accurately located before initiating any surgical procedure.
Panoramic radiography is simple, relatively inexpensive, and widely available diagnostic imaging modality which offers significantly low radiation exposure. Kaffe et al., found panoramic radiographs to be beneficial in locating mandibular foramen on two different panoramic machines (Philips Orthoralix SD Ceph and Gendex Panelipse II) [3]. On the other hand few researchers suggest that quantitative measurements should not be performed on panoramic radiographs as object may not coincide with the shape and position of the focal plane and thus there is inherent distortion of object’s anatomy on the radiograph [4]. The anterior border of ramus of mandible, external and internal oblique ridges, coronoid notch and occlusal plane have been used in different studies to determine the position of mandibular foramen. The study conducted by Kositbowornchai et al., on Thai adult mandibles concluded that there is a high concordance between the measured distances on panoramic radiographs and dry mandibles [5].
The present study was designed to evaluate the accuracy and reliability of panoramic radiographs in the localization of mandibular foramen on dry Indian adult mandibles using parameters applied by Kositbowornchai et al., with additional standardization.
Materials and Methods
The study was designed and performed in Oral Medicine and Radiology department of JSS Dental College, Mysore from the period of June 2010 to September 2010. Twenty five Indian dry human male adult mandibles (age range of 20-55 y) which were collected from the Forensic Department of JSS Medical College constituted the study material. Only those mandibles with first and second molars or canine and first/second molar on same side were selected. The edentulous mandibles and mandibles with tilted occlusal plane of the molars were excluded from the study. After considering inclusion and extrusion criteria, a total of 40 sides were measured on 25 dry mandibles. The study methodology was divided in anatomic and radiographic parts.
Anatomic study
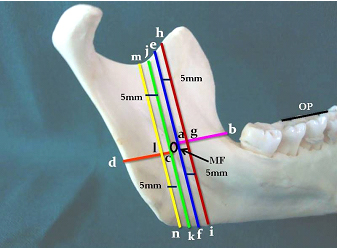
The teeth were used as reference plane for drawing imaginary occlusal plane. The position of mandibular foramen with respect to occlusal plane of teeth was noted. The location of mandibular foramen in relation to the midpoint of ramal width and height was also appreciated. Two points were marked on mandibular foramen i.e. antero-superior point as “a” and postero-inferior point as “c”. Ten distances were drawn with permanent black colour marker on the mandibles and later measured with the help of digital vernier calliper (Mitutoyo 500 series ± 0.001”/0.01mm calibration) similar to the study of Kositbowornchai et al., [5]. These distances were as follows
From point “a” to the anterior ramus (ab)
From point “c” to the posterior border of the mandible (cd)
From point “a” to the coronoid notch (ae)
From point “a” to the lower border of the mandible (af)
5 mm anteriorly from the point “a” to the coronoid notch (gh)
5 mm anteriorly from the point “a” to the lower border of the mandible (gi)
From point “c” to the coronoid notch (cj)
From point “c” to the lower border of the mandible (ck)
5 mm posteriorly from point “c” to the coronoid notch (lm)
5 mm posteriorly from point “c” to the lower border of the mandible (ln)
The lines ab and cd were parallel to each other and to the imaginary occlusal plane. The vertical lines were perpendicular to the horizontal lines ab and cd [Table/Fig-1]. All measurements were performed by the same observer twice to avoid inter observer inconsistency and mean was taken.
Ten distances measured on dry mandibles and later on traced panoramic images of the same
OP:- Occlusal Plane, MF:- Mandibular Foramen, ab:- Anterior ramus width, cd:- Posterior ramus width, ae:- Upper anterior ramus height, af:- Lower anterior ramus height, gh:- 5 mm anteriorly upper ramus height, gi:- 5 mm anteriorly lower ramus height, cj:- Upper posterior ramus height, ck:- Lower posterior ramus height, lm:- 5 mm posteriorly upper ramus height, ln:- 5 mm posteriorly lower ramus height
Radiographic study
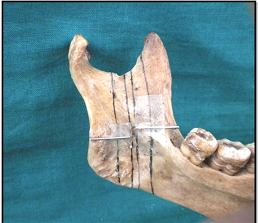
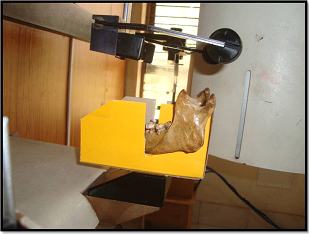
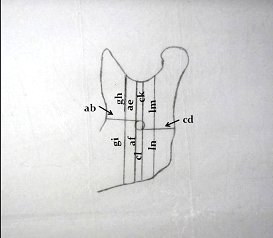
The stainless steel wire markers were placed over lines ab and cd with the help of adhesive [Table/Fig-2]. The dry mandibles were placed on a cardboard frame attached to chin of panoramic machine (magnification factor 1.25) in such a way that patient positioning in the clinical practice is maintained and the mandibles fall in the focal trough as far as possible [Table/Fig-3]. The mandibles were stabilised on the cardboard frame to reproduce the approximate soft tissue thickness in the chin region so that the base of the mandible was placed 6 mm above the chin rest [6]. Panoramic radiographs were made with 15x 30 cms T mat green sensitive films (Eastman Kodak, Rochester, New York), 15x 30 cms panoramic film cassette (Konica, Tokyo Japan) with green sensitive intensifying screens (Konica Minolta KR- II, Tokyo Japan), panoramic machine (Rotograph 230/EUR, ID: FIAD SpA – 20094, Trezzano S/Naviglio, Italy) and processed in automatic extraoral radiographic film processor (Promax 5 speed, Sl no. 04431030, Bangalore, India). The obtained radiographs were placed on Liquid Crystal Display view box, zinc acetate paper was placed over the radiograph and the images of the mandibles along with radiopaque horizontal lines reproducing lines ab and cd were traced on a zinc acetate paper with the help of lead pencil. The similar ten distances were drawn and then measured on the traced images with the digital vernier calliper [Table/Fig-4].
The stainless steel wires attached to lines ab and cd
The photograph showing positioning of dry mandibles in panoramic machine
Traced image of panoramic radiograph and distances measured on dry mandibles
Statistical Analysis
The magnification factor of the panoramic machine was subtracted from the distances measured. The obtained data was subjected to paired t-test to determine statistical significance. The p-value of less than 0.05 was considered significant. Pearson’s correlation analysis was also performed to evaluate and measure the strength of association between the distances measured on dry mandibles and radiographs.
Results
A total of 40 sides were measured on 25 mandibles. No statistically significant difference was noted between measurements on right and left side on both mandibles and radiographs. The mandibular foramen was found to be located in the line of occlusal plane on 15 sides (37.5%), below on 13 sides (32.5%) and above on 12 sides (30%). In anatomic study the mandibular foramen was found to be located posterior approximately by 1.76 mm and slightly superior on an average by 1.96 mm to midpoint of ramus. The average width of mandibular ramus (ab+cd) was 30.2 mm.
There was statistically significant difference between nine mean measurements of the distances performed on dry mandibles and radiographs. Those measurements were ab, cd, af, gh, gi, cj, ck, lm and ln. The distance ae did not show any statistically significant difference. The distribution of range, mean and standard deviation of all the ten distances carried is shown in [Table/Fig-5].
Range, mean and standard deviation of ten distances measured on dry mandibles and radiographs. (N=25)
| Measurement site | Panoramic radiographs (mm) | Dry mandibles (mm) |
|---|
| Range | Mean | SD | Range | Mean | SD |
|---|
| Anterior ramus width (ab) | 12.72 – 18.85 | 15.27 | 1.57 | 13.77-19.64 | 16.93 | 1.54 |
| Posterior ramus width (cd) | 9.94-16.67 | 13.73 | 1.73 | 9.43-15.54 | 13.33 | 1.57 |
| *Upper anterior ramus height (ae) | 11.01- 29.63 | 21.43 | 4.01 | 12.72-28.52 | 21.12 | 3.5 |
| Lower anterior ramus height (af) | 26.25-36.88 | 31.49 | 3.02 | 23.64-33.42 | 27.89 | 2.6 |
| 5 mm anteriorly- upper ramus height (gh) | 12.37-32.02 | 22.38 | 4.58 | 16.53-32.10 | 23.65 | 3.91 |
| 5 mm anteriorly – lower ramus height (gi) | 27.2-38.42 | 33.13 | 3.29 | 25.7-35.8 | 30.14 | 2.69 |
| Upper posterior ramus height (cj) | 14.21-34.39 | 25.59 | 4.33 | 16.9-31 | 23.67 | 3.45 |
| Lower posterior ramus height (ck) | 21.12-32.36 | 27.48 | 2.97 | 20.2-29.34 | 24.36 | 2.31 |
| 5 mm posteriorly upper ramus height (lm) | 18.51-35.06 | 27.63 | 4.03 | 18.9-33 | 25.44 | 3.47 |
| 5 mm posteriorly- lower ramus height (ln) | 19.75-30.06 | 25.66 | 3.15 | 18-28 | 22.73 | 2.34 |
There was strong positive correlation between all the measurements between dry mandibles and radiographs. The strongest correlation was found with distance ae (upper anterior ramus height) and the lowest with distance the distance ab (anterior ramus width). The correlation coefficient of all measurements is shown in [Table/Fig-6].
Correlation coefficient (r) of panoramic radiographs and dry mandible measurements
| Measurement site | Correlation coefficient (r) |
|---|
| * Anterior ramus width (ab) | 0.653 |
| Posterior ramus width (cd) | 0.872 |
| * Upper anterior ramus height (ae) | 0.975 |
| Lower anterior ramus height (af) | 0.922 |
| 5 mm anteriorly- upper ramus height (gh) | 0.873 |
| 5 mm anteriorly – lower ramus height (gi) | 0.885 |
| Upper posterior ramus height (cj) | 0.950 |
| Lower posterior ramus height (ck) | 0.936 |
| 5 mm posteriorly upper ramus height (lm) | 0.967 |
| 5 mm posteriorly- lower ramus height (ln) | 0.928 |
Discussion
The determination of the accurate anatomic location of mandibular foramen is essential to avoid any untoward outcomes such as haemorrhage and permanent neurologic damage caused by the transection of the neurovascular bundle during surgical procedures involving ramus of the mandible. It is not possible to palpate mandibular foramen intraorally, hence different anatomic landmarks such as occlusal plane, sigmoid notch, coronoid notch, external and internal oblique ridges have been used for localising it. Similarly, different conventional and advanced imaging modalities such as cephalometry, panoramic radiography, computed tomography and cone beam computed tomography are being used for the same [2].
The panoramic radiography was used in localization of mandibular foramen in the current study as oral surgeons routinely use panoramic radiography in evaluating the surgical sites before orthognathic and reconstructive surgeries as well as during trauma management. Though inherent distortion and magnification of the image are limitations with the use of panoramic radiography but still it can serve as a guide in locating mandibular foramen as Kaffe et al., reported that distortion and magnification were constant for two studied panoramic machines [3].
In the current study, the mandibular foramen was found to be located in the line of occlusal plane on 15 sides (37.5%), below on 13 sides (32.5%) and above on 12 sides (30%). Our findings indicate that majority of the mandibular foramen are located in occlusal plane. Similarly, in the anatomic study conducted by Mbajiorgu EF on 38 dry mandibles, 47.1 % mandibular foramen were found in occlusal plane, 29.4% above and 23.5% below the occlusal plane [7]. Thangavelu K et al., stated that mandibular foramen was found either in line or few mm below the occlusal plane of mandibular molars [8]. Moreover, the study conducted by Poonacha KS et al., support this finding as they reported that inferior alveolar nerve anaesthesia given at occlusal level rendered good results [9]. On the contrary Movahhed et al., reported that the location of mandibular foramen varies according to sex and age [10].
There was no statistical difference in the right and left side position of mandibular foramen. The finding is in harmony with the studies of Mbajiorgu EF, Movahhed et al, Hayward et al., Narayana K, Altunsoy M and co-workers [7,10–13].
The average mandibular ramus width was 30.2 mm in the present study. In the study conducted by Kositbowornchai et al., it was 35 mm [5]. This difference may be attributed to racial variation. However, the results can vary if the study is performed on a larger sample size.
In our study the mandibular foramen was found to be located posterior and slightly superior to midpoint of ramus on an average by 1.76 mm and 1.96 mm respectively. Similar finding has been reported by Kositbowornchai and co-workers [5]. The superior position of mandibular foramen has been supported by various authors [7]. Majority of the researchers support posterior to midpoint of rameal width presence of mandibular foramen [1,7,11]. Interestingly, Kanno et al., found no statistical differences in the distance of foramen to anterior and posterior borders [14].
In our study, we furthermore standardized the placement of dry mandibles in the panoramic machine as compared to study of Kositbowornchai et al., [5]. As per the study conducted the thickness of soft tissue below chin was found to be 6.16 mm whereas in the study by Kollman and Buchly on European white cadavers it was found to be 5.98 mm [6]. In the absence of any Indian standards, the above mentioned cardboard frame was designed so that the base of the chin of the dry mandible was placed 6 mm above the chin rest of panoramic machine.
In the present study, there were statistically significant differences between distances measured on dry mandibles and radiographs except for the upper anterior ramus height (ae). Thus antero-superior point of the mandibular foramen (a) was precisely located on the panoramic radiographs. This finding is not in unison with Kositbowornchai et al., as they didn’t report any point which could be accurately located on radiographic images owing to standardization of dry mandibles placement in our study. These differences may be attributed to the fact that the distances measured on panoramic radiographs may be different from those on dry mandibles due to the effect of radiographic angulation [5]. Moreover, the findings of one panoramic machine cannot be applied on other as there are differences in technical characteristics leading to differences in resolution of the image layer, and variations in degree of distortion and vertical and horizontal magnification [3].
Statistically, strong positive correlation between distances measured on dry mandibles and panoramic radiographs was found which is in accordance with the study conducted by Kositbowornchai and co-researchers [5]. The strongest correlation was found with upper anterior ramus height (ae) and lowest with anterior ramus width (ab). In the study by Kositbowornchai et al., strongest positive correlation was noted with upper anterior ramus height which is comparable to current study but the lowest correlation was noted 5 mm posterior- upper ramus height (ln). In the study performed by Varma et al., on south Indian mandibles, the distance of mandibular foramen was roughly 16 mm from the anterior border of ramus [15]. In our study (distance ab) the mandibular foramen was found to be 16.9 mm (mean) from anterior border of ramus on the mandibles. On the panoramic radiographs the distance was 15.27 mm (mean) and thus was not reliable. This disparity in the results may be attributed to different panoramic systems used, variation during placement of dry mandibles in OPG machines and racial variations.
The authors postulate that the precise distances can be derived by formulating ratio between measurements on dry mandibles and on panoramic radiographs to locate the boundary and thus the position of mandibular foramen. However, it is advisable that the study should be performed on larger sample size, different panoramic systems, on different age groups, both the genders and various populations. Whenever it is possible, advanced imaging modality like computed tomography should be sought to localize vital anatomic landmarks before initiating any surgical procedure.
Conclusion
In the present study the distances measured on dry mandibles and radiographs showed statistically significant difference except the upper anterior ramus height. Hence, antero-superior point on mandibular foramen was accurately located. This landmark can guide oro-maxillofacial surgeons during surgical procedures. The result however should be confirmed on a larger sample size considering sex variability and different age groups. In a developing country like India where majority of population cannot afford costly imaging modalities, the exploration of cost effective panoramic radiography in localizing anatomic landmarks such as mandibular foramen may be a welcoming thought.