The introduction of preformed archwires and new bracket designs in orthodontic practice has greatly changed orthodontic practice and reduced patient chair time. An increasing variety of new archwire materials have also become available. Nickel-titanium (NiTi) wires are now used in the majority of cases for initial leveling and aligning [1]. However, their super elastic property makes customization of arch form and size difficult. In order to maintain pre-treatment arch forms, it is more reasonable to have different types of preformed arch wires available that operator could choose to most closely match the patient’s pretreatment arch form.
A study of clinicians’ choices when selecting arch wires during the initial and latter stages of orthodontic treatment report that clinicians use available preformed NiTi archwire in the early stage and stainless steel in the latter stage of treatment for preservation of the pre-treatment arch form. In particular, maintaining of the initial intercanine and intermolar widths were considered important in stability [2–4].
Because the treatment philosophy in our clinic is to maintain pre-treatment arch forms throughout treatment, we match non-customized preformed NiTi archwires to individual patient archforms during treatment planning. This selection is usually made by visual comparison of archwires placed against the facial surfaces of both mandibular and maxillary dental casts. It has always been of interest to be more quantitative in this selection process. With this in mind, we designed a study to compare average dental arch forms of Class I and Class II div 1 malocclusions to those of the preformed NiTi archwires currently used which are the two most common malocclusion seen in our clinic.
Materials and Methods
Subject Selection
Groups of Angle Class I and Class II div 1 patients were selected from patient records at the Mahidol University Dental School Graduate Orthodontic Clinic.
Selection criteria for the Class I study group were: (1) meets all of Angle’s classification I criteria, (2) no cusp attrition, fractured teeth, or restorations extending to contact areas, cusp tips or incisal edges, (3) complete permanent dentition with normal size and shape including fully erupted 2nd molars, (4) arch length discrepancy less than 3 mm, (5) no history of prior orthodontic treatment.
Selection criteria for the Class II, division 1 study group were: (1) meets all of Angle’s classification II, division 1 criteria, (2) age 17–25 y at the start of treatment, (3) overjet between 4 and 9 mm, (4) complete permanent dentition with normal size and shape including fully erupted 2nd molars, (5) no cusp attrition, fractured teeth, or restorations extending to contact areas, cusp tips or incisal edge, (6) no previous adjunctive appliance treatment as part of their orthodontic treatment -- such as a quad helix appliance, functional appliance, or rapid palatal expander, (7) patients were to be treated by four 1st premolar extractions as part of a comprehensive orthodontic treatment plan, (8) post-treatment dental casts were available at least one year into retention.
Using the above criteria, 40 Class I (20 male, 20 female) and 22 Class II, division 1 (8 male, 14 female) were selected.
A third study group was defined comprised of the post-treatment Angle class II, division 1 patients (n=22). This group was added to the study because extraction cases are reported to show significant permanent arch form changes [3]. It was of interest to determine how well the non-customized preformed arch wires matched both early treatment and post-treatment arch forms.
Dental Arch form Landmark Definitions
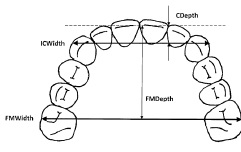
Dental arch form was described by four landmarks – arch width and depth (midline length) at canine and 1st molar locations from proximal first inter-incisal contact point [Table/Fig-1] [5].
Preformed Archwire Selection
Twelve preformed archwires from six manufacturers were selected. These companies were 3MUnitek, Highland, G&H, American Orthodontics, RMO, and Ormco. Five of the archwires have also been used in similar published studies of Caucasian, Japanese, and Indian Class I malocclusions [Table/Fig-2]. Identification numbers were assigned to each of the archwire forms tested. [Table/Fig-3] lists this information along the different types of wire material available. This particular set of archwires was selected because of their availability and common use in our clinic.
Preformed archwire sets tested in comparative dental arch form studies
| Manufacturer | Archwire Form Trade Name | Studies |
|---|
| White [6] 1978 USA n=24(I) | Felton [7] 1987 USA n=30(I) n=30(II) | Braun [8] 1999 USA n=15(I) | Oda [9] 2010 Japan n=30(I) | Bhowmik [10] 2012 India n=40(I) | Present study Thailand n=40(I) n=22(II) |
|---|
| AmOrth, USA | Natural Arch Form I | | | | x | x | X |
| Natural Arch Form II | | | | x | x | |
| Natural Arch Form III | | | | x | | |
| Dentsply-Sankin, Japan | Tynilloy (large) | | | | x | | |
| Tynilloy (small) | | | | x | | |
| Dentaurum, Gb | Proform Arch Shape | | | | | x | |
| GAC, USA | Accu Form | | | | x | | |
| Standard Form | | | | x | | |
| G&H, USA | True Form I | | | | | | X |
| Europa Form I | | | | | | X |
| Highland, USA | Mid size (maxillary only) | | | | | | X |
| Natural Arch Form | | | | | | X |
| Progressive Arch Form | | | | | | X |
| Lancer, USA | | | | | | x | |
| Libral T, India | Euroform | | | | | x | |
| Modern O, India | Natural Form | | | | | x | |
| Orthoform | | | | | x | |
| Oral Care, Japan | Smooth Arch Form | | | | x | | |
| Orange O, India | | | | | | x | |
| Ormco, USA | Broad Arch (large) | | | x | x | | |
| Broad Arch (small) | | | x | x | | X |
| Orthos (large) | | | x | x | | |
| Orthos (small) | | | x | x | | |
| Vari-Simplex (large) | | x | | x | | |
| Vari-Simplex (small) | | x | | x | | |
| Tru-Arch (medium) | | x | | x | | |
| Tru-Arch II (medium) | | | x | x | | |
| Par arch form | | x | | | | |
| Ortho Org, USA | Proform | | | | x | x | |
| Orthotec, USA | Nuform | | | | | x | |
| RMO, USA | Natural Arch Form | | | | | | X |
| Ideal Arch Form | | | | | | X |
| Pentamorphic | | x | | | | |
| SIAOrth, Italy | Standard Shape | | | | | x | |
| Natural Shape | | | | | x | |
| Template Forms | Bonwill-Hawley | x | | | | | |
| Brader | x | x | | | | |
| Cantenary curve | x | | | | | |
| RMDS | x | | | | | |
| 3MUnitek, USA | Orthoform I,(tapered) | | | x | x | x | X |
| Orthoform II,(square) | | | x | x | x | X |
| Orthoform III, (ovoid) | | | | x | x | X |
AmOrth = American Orthodontics, Lancer = Lancer Orthodontics , Libral T = Libral Traders, Modern O = Modern Orthodontics, Orange O = Orange Orthodontics, Ortho Org = Ortho Organizers, RMDS = Rocky Mountain Data Systems, RMO = Rocky Mountain Orthodontics, SIAOrth = SIA Orthodontics, n = sample size, I = Class I, II=Class II
Assignment of archwire identification numbers
| Archwire ID number | Manufacturer | Archwire Form Trade Name | Available Archwire Materials |
|---|
| 1 | 3M Unitek | Orthoform I, tapered | NiTi (superelastic and heat activated), beta-Titanium, and stainless steel(solid) |
| 2 | Orthoform II, standard |
| 3 | Orthoform III, ovoid |
| 4 | Highland | Mid size (only maxillary arch used) | NiTi (superelastic and heat activated) and stainless steel (solid and braided) |
| 5 | Natural arch form |
| 6 | Progressive arch form |
| 7 | G&H | True form I | NiTi (superelastic and heat activated), beta-Titanium, and stainless steel (solid and braided) |
| 8 | Europa form I |
| 9 | American Orthodontics | Natural arch form I | NiTi (superelastic and heat activated), beta-Titanium, and stainless steel (solid and braided) |
| 10 | RMO | Natural arch form | NiTi (superelastic and heat activated), Elgiloy,stainless steel (solid),CuNiTi, and TiMo (Natural arch form only) |
| 11 | Ideal arch form |
| 12 | Ormco | Broad arch, small | NiTi (superelastic and heat activated), stainless steel (solid and braided),CuNiTi, beta-Titanium, and Titanium-Niobium |
Digitizing Plaster Cast Landmarks
The desired bracket positions for each tooth were marked on casts with pencil [Table/Fig-4].
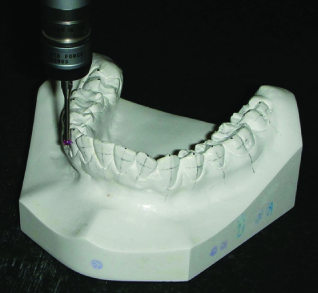
A LK Tools G-90C measuring instrument was used to digitize the plaster cast landmarks [Table/Fig-5a&b]. This coordinate measuring machine (CMM) uses a frictionless air bearing touch probe to record XYZ spatial coordinates. To digitize landmarks, dental casts were first positioned with all incisal edges and cusp tips in a fixed plane. The digitizing instrument allows one to measure arch depth and width by moving it between marked landmarks and recording the effective distance between points in the XY space. Moving the touch probe over a straight line showed it to have a linear accuracy of 6 microns and reproducibility of 4 microns.
(a) LK Tools G-90C Machine. (b) LK Tools G-90C Probe

All dental casts were measured by the same technician. A reproducibility study was conducted to evaluate measurement accuracy. Randomly at 4 weeks intervals, the technician repeated measurements on several sets of dental casts. Analysis of these results showed less than 0.5% measurement error.
Digitizing Preformed Archwire Landmarks
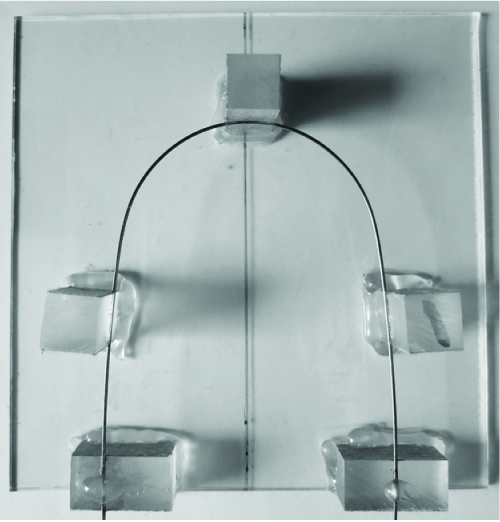
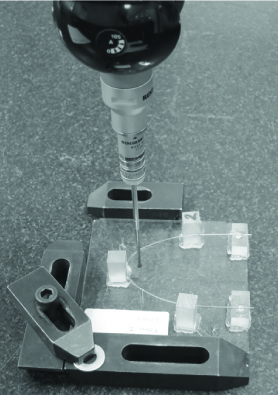
Although NiTi archwires are used for treatment, the arch forms actually measured were stainless steel 0.019 x 0.025 wires with the same arch form. They were used because of their greater rigidity and tensile strength for mounting. To digitize landmarks, wires were first mounted to a glass plate holding fixture [Table/Fig-6]. They were aligned over two reference lines marking the center of each glass plate. Once aligned, wires were held in place by five acrylic blocks (1x1x2 cm) glued with a structural acrylic adhesive (3M®, USA). The digitizing probe first measured the mean canine dental arch depth for each study group [Table/Fig-7]. It was then moved perpendicular to this landmark to measure the wire’s inter-canine width. The inter first molar width was measured in a similar fashion – using the mean first molar arch depth. Ten samples of each preformed archwire type were digitized. A reproducibility study was conducted by the technician on 24 maxillary and 22 mandibular different archwires. Analysis of these results showed less than 0.5% measurement error.
Top view of holding fixture
Statistical Analysis
Means, standard deviations, and medians of the measured dental arch widths and depths were calculated with SPSS software (version 17; SPSS, Chicago Ill). The confidence intervals for inter-canine and inter first molar widths were calculated with Microsoft Excel. The distributions of mean preformed archwire widths at the canine and first-molar levels were graphically compared with the corresponding confidence intervals for the untreated Class I and II div 1 and post-treatment Class II div 1 groups.
Results
[Table/Fig-8] shows the mean dental arch depths for the three Thai populations studied. Both maxillary and mandibular canine arch depths were found to be statistically the same for all groups. First molar arch depths were the same in both arches for untreated Class I and Class II div 1 groups only. However, the post-treatment Class II mean 1st molar depth was significantly shorter in both the maxilla and mandible. This difference is estimated to be between 4 to 9 mm in the maxillary and 1 to 8 mm in the mandibular arch.
Mean dental arch depth at the canine and first molars for thai sample populations
| [1] Class I Untreated (n=40) |
|---|
| Maxillary Arch | Mandibular Arch |
|---|
| Mean ±(SD) | CI(0.99)† | Mean ±(SD) | CI(0.99) |
|---|
| Canine Arch Depth | 9.0± (2.1) | 8.2 - 9.8 (mm) | 5.1± (2.3) | 4.2–60 (mm) |
| First Molar Arch Depth | 31.3 ±(2.0) | 30.5– 32.1 (mm) | 26.4± (2.0) | 25.6– 27.2 (mm) |
| [2] Class II division 1 Untreated (n=22) |
|---|
| Maxillary Arch | Mandibular Arch |
|---|
| Mean± (SD) | CI(0.99) | Mean± (SD) | CI(0.99) |
|---|
| Canine Arch Depth | 8.6± (1.9) | 7.6–96 (mm) | 5.0 ±(1.9) | 4.0–60 (mm) |
| First Molar Arch Depth | 31.7± (1.9) | 30.7–327 (mm) | 26.4± (1.7) | 25.5–273 (mm) |
| [3] Class II division 1 Post-Treatment Four 1st Premolar Extraction (n=22) |
|---|
| Maxillary Arch | Mandibular Arch |
|---|
| Mean± (SD) | CI(0.99) | Mean± (SD) | CI(0.99) |
|---|
| Canine Arch Depth | 9.0± (2.0) | 8.0–100 (mm) | 5.5± (1.8) | 4.5–65 (mm) |
| First Molar Arch Depth | 24.9± (2.1) | 23.8–260 (mm) | 20.4± (2.2) | 19.2–216 (mm) |
†CI(0.99) = confidence interval of measurement’s mean value at 99% probability
[Table/Fig-9] shows both the maxillary and mandibular dental inter-canine and 1st molar arch widths were statistically the same in all three study groups.
Mean dental arch widths at the canine and first molars for thai sample populations
| [1] Class I Untreated (n=40) |
|---|
| Maxillary Arch | Mandibular Arch |
|---|
| Mean ±(SD) | CI(0.99)† | Mean± (SD) | CI(0.99) |
|---|
| Inter Canine Width | 39.8± (1.9) | 39.0–406 (mm) | 31.0± (1.5) | 30.4–316 (mm) |
| Inter First Molar Width | 59.5± (2.3) | 58.6–604 (mm) | 53.4± (2.0) | 52.6–542 (mm) |
| [2] Class II division 1 Untreated (n=22) |
|---|
| Maxillary Arch | Mandibular Arch |
|---|
| Mean± (SD) | CI(0.99) | Mean± (SD) | CI(0.99) |
|---|
| Inter Canine Width | 39.4± (2.5) | 38.1– 40.7 (mm) | 30.6± (2.5) | 29.3–319 (mm) |
| Inter First Molar Width | 58.2± (2.9) | 56.7– 59.7 (mm) | 53.6± (2.5) | 52.3–549 (mm) |
| [3] Class II division 1 Post-Treatment Four 1st Premolar Extraction (n=22) |
|---|
| Maxillary Arch | Mandibular Arch |
|---|
| Mean± (SD) | CI(0.99) | Mean± (SD) | CI(0.99) |
|---|
| Inter Canine Width | 40.1± (1.8) | 39.1–411 (mm) | 31.4± (1.7) | 30.5–323 (mm) |
| Inter First Molar Width | 55.8± (2.5) | 54.5–571 (mm) | 50.6± (2.0) | 49.5–517 (mm) |
†CI(0.99) = Confidence interval of measurement’s mean value at 99% probability
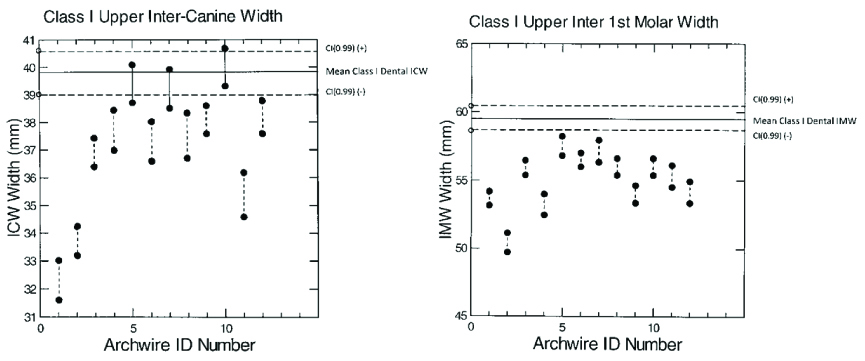
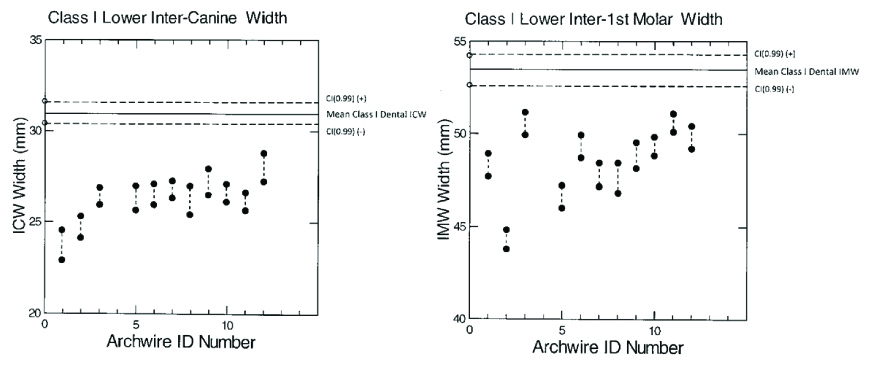
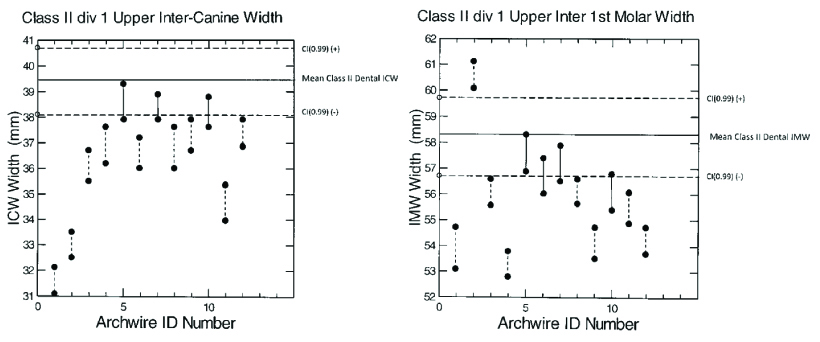
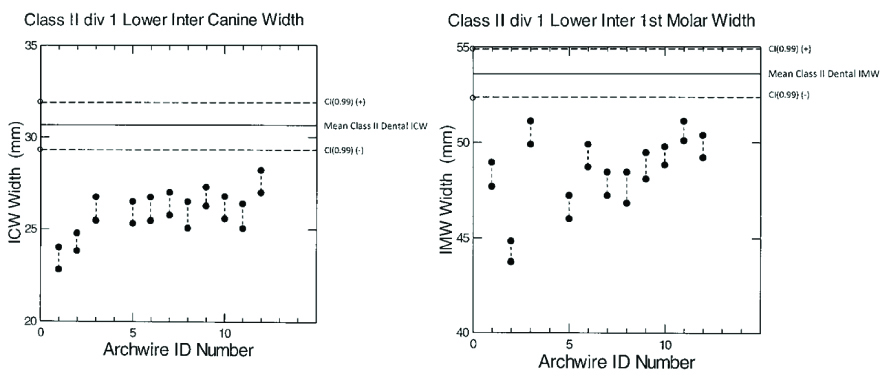
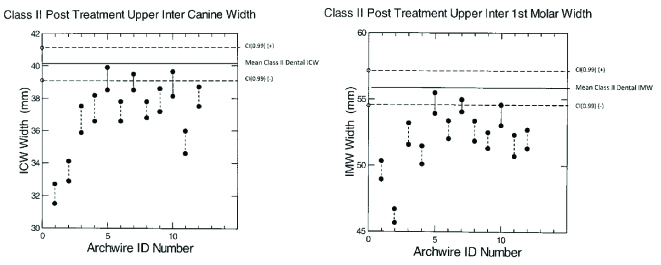
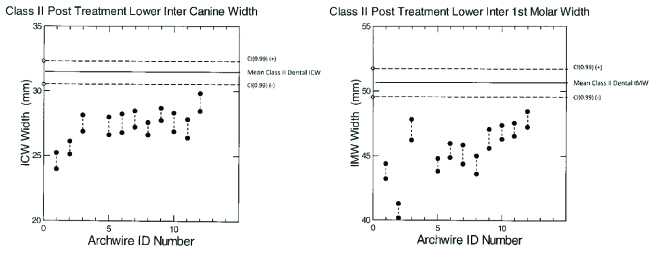
[Table/Fig-10,11,12,13,14,15] compare the mean inter-canine and 1st molar widths for group dental arches and the 12 preformed archwire forms studied. [Table/Fig-16] summarizes this information.
Comparison of class I dental inter-canine (left) and first molar widths (right) to maxillary preformed archwires
Comparison of class I dental inter-canine (left) and first molar widths (right) to mandibular preformed archwires
Comparison of class II div 1 dental inter-canine (left) and first molar widths (right) to maxillary preformed archwires
Comparison of Class II div 1 dental inter-canine (left) and first molar widths (right) to mandibular preformed archwires
Comparison of Class II div 1 post-treatment dental inter-canine (left) and first molar widths (right) to maxillary preformed archwires
Comparison of Class II div 1 post-treatment inter-canine (left) and first molar widths (right) of mandibular preformed archwires
Comparison of non-customized preformed archwire and dental inter-canine and 1st molar arch widths for thai class I and class II div1 malocclusions
| Archwire ID | Company | Class I untreated (n=40) | Class II div 1 untreated (n=22) | Class II div 1 post treatment (n=22) |
|---|
| Maxillary | Mandibular | Maxillary | Mandibular | Maxillary | Mandibular |
|---|
| ICW | FMW | ICW | FMW | ICW | FMW | ICW | FMW | ICW | FMW | ICW | FMW |
|---|
| 1 | 3MUnitek | L | L | L | L | L | L | L | L | L | L | L | L |
| 2 | L | L | L | L | L | L | L | L | L | L | L | L |
| 3 | L | L | L | L | L | L | L | L | L | L | L | L |
| 4 | Highland | L | L | L | L | L | L | L | L | L | L | L | L |
| 5 | EQ | L | L | L | EQ | EQ | L | L | EQ | EQ | L | L |
| 6 | L | L | L | L | L | EQ | L | L | L | L | L | L |
| 7 | G&H | EQ | L | L | L | EQ | EQ | L | L | EQ | EQ | L | L |
| 8 | L | L | L | L | L | L | L | L | L | L | L | L |
| 9 | AmOrtho | L | L | L | L | L | L | L | L | L | L | L | L |
| 10 | RMO | EQ | L | L | L | EQ | EQ | L | L | EQ | EQ | L | L |
| 11 | L | L | L | L | L | L | L | L | L | L | L | L |
| 12 | Ormco | L | L | L | L | L | L | L | L | L | L | L | L |
Key: ICW=inter-canine width, FMW=inter first molar width, EQ=archwire and dental arch widths are statistically equal, G=archwire width is greater than dental arch width, L=archwire width is less than dental arch width
The maxillary arch Class I group shows 3 of the 12 selected archwires have inter-canine widths statistically the same as the dental inter-canine widths. These particular wires are Highland Natural arch form, G&H True form I, and RMO Natural arch form. All archwire 1st molar widths are significantly less than the dental 1st molar widths. These differences range between 1 to 11 mm. In both the Class II untreated and post-treatment groups, the same three archwires above showed both inter-canine and 1st molar widths statistically the same as the dental arch measurements. An additional archwire showed the same 1st molar width as the untreated Class II group. This was the Highland Progressive arch form wire. All other preformed archwires tested showed canine and molar widths significantly narrower than the dental widths.
The mandibular dental arches for all malocclusion study groups showed both dental inter-canine and 1st molar widths statistically wider than all of the preformed archwires tested. These differences ranged between 2 and 10 mm.
Discussion
[Table/Fig-17] compares our results for Class I patients to those of three earlier studies of comparative arch form width. Braun reports 3MUnitek’s Orthoform I and II wires and Ormco’s Broad arch form have significantly larger inter-canine and first molar widths compared to dental arch forms in both maxillary and mandibular arches of Caucasian patients [8]. Comparing the mandibular arch of Japanese Class I patients to common archwire forms, Oda reports 3M Unitek Orthoform I and III wires have significantly smaller inter-canine and first molar widths [9]. In contrast, 3M Unitek’s Orthoform II and Ormoco small Broad arch form wires had inter-canine widths equal to the mean dental width. However, the first molar width in these two particular wires was significantly less than the dental measurements. Bhowmik studied 3M Unitek Orthoform I,II, and III and American Orthodontics Natural arch preformed archwires in male and female patients from India [10]. With few exceptions, all archwires had significantly larger inter-canine and first molar widths in both the maxilla and mandible. An exception was the Orthoform II standard archwire. It had significantly smaller arch inter-canine and first molar widths in male mandibular arches.
Summary of preformed archwire inter-canine and first molar widths compared to dental class i measurements
| Archwire ID | Company | Archwire Trade Name | Study | Race | Maxillary | Mandibular |
|---|
| ICW | FMW | ICW | FMW |
|---|
| 1 | 3MUnitek | Orthoform I tapered | Braun [8] | Caucasian | GT | GT | GT | GT |
| Oda [9] | Japanese | | | LT | LT |
| Bhowmik [10] | India | M/F | GT | GT | GT | GT |
| Thailand | Thai | LT | LT | LT | LT |
| 2 | 3MUnitek | Orthoform II standard | Braun | Caucasian | GT | GT | GT | GT |
| Oda | Japanese | | | EQ | LT |
| Bhowmik | India | F | GT | GT | GT | GT |
| M | GT | GT | LT | LT |
| | | Thailand | Thai | LT | LT | LT | LT |
| 3 | 3MUnitek | Orthoform III, ovoid | Oda | Japanese | | | LT | LT |
| Bhowmik | India | M/F | GT | GT | GT | GT |
| Thailand | Thai | LT | LT | LT | LT |
| 9 | AmOrtho | Natural arch form | Oda | Japanese | | | EQ | LT |
| Bhowmik | India | M/F | GT | GT | GT | GT |
| Thailand | Thai | LT | LT | LT | LT |
| 12 | Ormco | Broad arch, small | Braun | Caucasian | GT | GT | GT | GT |
| Oda | Japanese | | | EQ | LT |
| Thailand | Thai | LT | LT | LT | LT |
Key: ICW=inter-canine width, FMW=inter first molar width, EQ=archwire and dental arch mean widths are statistically equal, GT=archwire width is greater than dental arch width, LT=archwire width is less than dental arch width, M=male, F=female
Our results confirm previously published works [8–10] indicating that preformed archwires are available matching both the inter-canine and first molar widths of dental arches. However, the need to stock many different commercial archwires to find a few such wires matching a particular dental arch form is not economical. Rather, there remains a need to customize wires. If not for the difficulty adjusting NiTi type materials, some of the current discussion on whether to use non-customized preformed NiTi archwires would be unnecessary [11,12]. Rather, individualization of super-elastic wires could begin early in treatment during initial leveling. Instead, such adjustments generally begin after progression to heavier wires in later treatment [13].
Our study has several limitations. The sample size is relatively small – 40 Class I and 22 Class II patients. However, this is a common problem found in other studies as well. The average sample size for the prior five studies ranged from 15 to 40 patients. Also, our methodology does not take into consideration bracket thickness and variable slot depth. The anteroposterior repositioning of archwires at the incisors because of bracket thickness changes width measurements at the canine and first molar levels. Oda et al report the average bracket thicknesses in their study was 0.8 mm. Finally, our conclusions are based on showing only statistically similarity of the inter-canine and 1st molar widths. Comparison of continuous archwire and dental arch forms is not possible with the methodology used [14,15].
Conclusion
The primary objective of this study was to determine whether the arch forms of a particular set of non-customized preformed orthodontic archwires differ significantly from those of untreated Class I and Class II division 1 malocclusions. In addition, whether four first premolar extraction treatment changes dental arch form in the group of Class II div 1 patients was also observed.
In all three study groups, the mandibular arch preformed archwires had canine and molar widths significantly less than the dental arch measurements. If used unadjusted, they would be expected to narrow the dental arch form.
With few exceptions, maxillary preformed archwires also had both inter-canine and first molar widths significantly less than dental arch measurements for both Class I and Class II div 1 patients. A few exceptions were found in all three study groups. In the Class II groups, three archwires had both inter-canine and first molar widths statistically equal to the mean dental arch values. These archwires were Highland Natural arch form, G&H True form I, and American Orthodontics Natural arch form I. Additionally, the untreated Class II first molar width was also matched by Highland’s Progressive archwire molar width. The maxillary Class I dental arch was significantly wider than all preformed archwires with three exceptions. These were also Highland Natural arch form, G&H True form I, and American Orthodontics Natural arch form I archwires. However, in these cases, only the inter-canine widths were equal to dental mean widths. Inter first molar widths were all significantly less than dental measurements.
Without adjustment, neither the maxillary nor mandibular preformed archwires studied will produce a significant expansive force in Thai patients. Rather, they are all as a group either constrictive or neutral in form.
Three maxillary preformed archwires can be used in Class I and Class II div 1 malocclusions without affecting the dental arch form significantly. These are Highland Natural arch form, G&H True form, and American Orthodontics Natural arch form I.
†CI(0.99) = confidence interval of measurement’s mean value at 99% probability
†CI(0.99) = Confidence interval of measurement’s mean value at 99% probability
Key: ICW=inter-canine width, FMW=inter first molar width, EQ=archwire and dental arch widths are statistically equal, G=archwire width is greater than dental arch width, L=archwire width is less than dental arch width
Key: ICW=inter-canine width, FMW=inter first molar width, EQ=archwire and dental arch mean widths are statistically equal, GT=archwire width is greater than dental arch width, LT=archwire width is less than dental arch width, M=male, F=female