Agnathia Holoprosencephaly and Situs Inversus in A Neonate Born to an Alcoholic Mother
Dibyajyoti Goswami1, Giriraj Kusre2
1 Post Graduate Trainee, Department of Anatomy, Assam Medical College and Hospital, Dibrugarh, Assam, India.
2 Associate Professor, Department of Anatomy, Assam Medical College and Hospital, Dibrugarh, Assam, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Giriraj Kusre, Associate Professor, Department of Anatomy, Basic Science Building, Assam Medical College and Hospital, Dibrugarh, Assam-786002, India. E-mail : giriraj.kusre@rediffmail.com
Agnathia, holoprosencephaly and situs inversus complex is an extremely rare form of congenital malformation. Though a few cases have been reported from other parts of the world, to the best of our knowledge none has been reported from India so far. Maternal alcoholism is regarded as an important factor causing holoprosencephaly. Disruption of the Shh gene signaling pathway is also said to be a factor for the occurrence of holoprosencephaly as well as left right asymmetry. Though several factors are suspected as a cause of this deformity, the precise aetiopathogenesis is still under debate. Lack of knowledge might be due to paucity of data from cases due to its rarity. Hereby, we are presenting a case of agnathia, holoprosencephaly and situs inversus born at 32 wk of gestation by an alcoholic mother. Externally the child had agnathia and cyclopia. There was no mandible or any oral cavity. It was accompanied by noticeable limb deformity. Internally there was holoprosencephaly, situs inversus totalis with several visceral abnormalities. To the best of our knowledge this is the first case of agnathia, holoprosencephaly and situs inversus complex to be reported in an indexed literature from India. This report also strengthens the association of maternal alcoholism with occurrence of holoprosencephaly.
Alcohol, Birth defect, Congenital, Cyclopia, Maternal, Shh gene
Case Report
A male child was born after 32 weeks of gestation by a 30-year-old multigravid alcoholic mother in Assam Medical College and Hospital, Dibrugarh, India. The pregnancy was complicated by polyhydramnios and eclampsia necessitating delivery by emergency cesarean section. The mother belonged to a lower socioeconomic family who used to take locally prepared alcohol regularly. The child died five minutes after birth because of severe asphyxia. There was no history of consanguinity, exposure to any other teratogenic drug except for alcohol or any family history of dysmorphism. The child measured 39 cm in length with head circumference 20 cm and weight 1.8 kg. Externally, the most noticeable findings were agnathia, synotia with bilateral preauricular pits and a single median diamond shaped orbit containing single eyeball and two pairs of eyelids laterally [Table/Fig-1]. Medial puncta on both sides were absent. Anterior hairline was placed more anteriorly and posterior hairline was normal in absence of any palpable fontanelle. A single rounded protrusion with a dimple indicated the site of mouth. The neck was very short. Limb deformity was observed in the form of bilateral absence of thumb. The anus was perforate and external genitalia were of male.
External appearance of the baby

X-ray revealed presence of ten ribs bilaterally, four metacarpals on both hands and absence of right radius. Feature of situs inversus was indicated by a left sided liver shadow [Table/Fig-2a-d].
Internal findings. (a) Shows radiological findings. Note absence of radius on right side (RA) and liver shadow in left side. (b) Shows intra abdominal findings. Spleen is on left side where as inferior vena cava (IVC) is placed towards left to the abdominal aorta (AA). (c) Shows the presence of Double superior vena cava (SVC). (d) Shows appearance of brain. Note absence of gyrus and sulcus along with fusion of both cerebral hemispheres
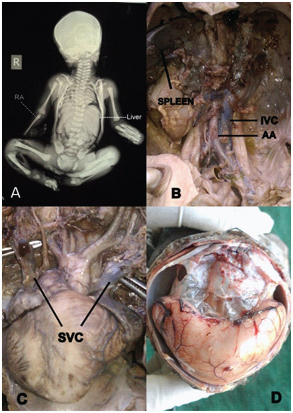
On autopsy, we found situs inversus totalis with reversed thoracic and abdominal contents. Liver, gall bladder, appendix and ascending colon were on left side where as spleen and descending colon was on right side. The heart was more towards right and the aortic arch descended on right side in presence of persistent ductus arteriosus which was much wider than its usual occurrence. Aorta was homed right to inferior vena cava. Another interesting finding was the presence of double superior vena cava without any connection. Both drained into the coronary sinus. The right lung was bilobbed whereas the left one was with three lobes.
On opening the skull, we found alobar holoprosencephaly where the two cerebral hemispheres were fused medially. There was no gyrus and sulcus. Ventricles were mal developed and were replaced by a large cyst filled with clear fluid. Corpus callosum, pituitary fossa, dural sinuses and olfactory nerves were absent in presence of a single optic nerve that had emerged posteriorly from the single orbit. Other cranial nerves were in normal position.
Discussion
Holoprosencephaly (HPE) is the most common developmental disorder of developing forebrain that results from incomplete cleavage of the prosencephalon into right and left hemispheres, occuring between the 18th to 28th days of gestation [1]. Prevalence of this condition is about 1/16000 live birth [2–4]. In the severest form it is known as alobar HPE which is characterized by a single brain ventricle and no interhemispheric fissure [5]. This class of HPE is generally associated with facial anomalies like anophthalmia, cyclopia or proboscis [6,7]. In addition to the defect in the cerebral structures, some sufferers also presents in association with agnathia which is another extremely rare anomaly with a prevalence of less than 1 in 70,000 births [8]. A situs abnormality, on the other hand is a condition where disturbance of left right embryonic pattern occurs showing unusual spatial arrangements of thoracic and/or abdominal organs in relationship to one another. Patients with agnathia and HPE may present with situs inversus, though this association is very rare. In the sufferers of agnathia HPE and situs inversus, the associated visceral anomalies are usually incompatible with life. Leech described the first reported child with this spectrum [9]. Leech also proposed the most acceptable anatomic sub classification of agnathia. It consists of 1) agnathia alone, 2) agnathia with holoprosencephaly, 3) agnathia, situs inversus and visceral anomalies and 4) agnathia, holoprosencephaly and situs inversus with visceral anomalies. Thus, the present case belongs to the fourth category. Agnathia, HPE and situs inversus complex represents a developmental field defect that involves midline embryonic structures [9]. Both hereditary as well as environmental insult has been proposed to be responsible to explain association of HPE as well as agnathia though precise aetiology is still unclear [10–12]. Kauver et al., reviewed six previously reported cases of this spectrum with addition of a new case [13]. Cardiac abnormality in some form was found in all except one of the seven of these cases [14–17]. The same findings appeared in our case in the form of dextrocardia, double superior vena cava and patent ductus arteriosus. To the best of our knowledge, our case represents the first one of this rare entity from India. Establishment of the vertebrate axial midline is a highly conserved developmental process [18]. Disturbance in this process results in laterality disturbances, including cardiac defects with inadequately developed face and brain. Cohen suggested an association between cytogenetically normal holoprosencephaly and maternal alcohol consumption during early pregnancy [19]. Besides environmental insult certain genes are found to be associated with holoprosencephaly. One such gene is Sonic Hedgehog (Shh) found in the chromosome 7q36 [20]. In addition to signaling the development of brain and mandible, Shh gene signaling pathway is also important for left-right orientation during developmental period of vertebrates. Mouse embryos lacking Shh gene display a variety of laterality defect including pulmonary left isomerism, alteration of cardiac looping and randomization of axial turning [21]. Thus all the three components of our case namely agnathia, holoprosencephaly and situs inversus may be attributed to Shh gene mutation. Mutation of Shh gene exacerbates the teratogenic effect of alcohol [22]. As already mentioned, the mother in our case was also alcoholic. Because of causal heterogeneity, the portrait elaborating pathogenesis of this spectrum is still blurred. Further research is required to better illustrate the causal and pathogenic basis of this association. For that we need gathering of information from more and more cases. We believe our report will put more light to the existing knowledge pertaining to this rare yet interesting form of birth defect.
Conclusion
The triad of agnathia, holoprosencephaly and situs inversus is a rare but very interesting congenital malformation. Very little is known about the factors responsible for its occurrence. Our report strengthens the possible association between this birth defect and maternal alcoholism.
[1]. Dubourg C, Bendavid C, Pasquier L, Henry C, Odnet S, David V, HoloprosencephalyOrphanet J Rare Dis 2007 2:8 [Google Scholar]
[2]. Cohen MM, Perspectives on holoprosencephaly: Part III. Spectra, distinctions, continuities, and discontinuitiesAm J Med Genet 1989 34(2):271-88. [Google Scholar]
[3]. Cohen MM, Perspectives on holoprosencephaly: Part I. Epidemiology, genetics, and syndromologyTeratology 1989 40(3):211-35. [Google Scholar]
[4]. Roach E, Demyer W, Conneally PM, Palmer C, Merritt AD, Holoprosencephaly: Birth data, benetic and demographic analy- ses of 30 familiesBirth Defects Orig Artic Ser 1975 11(2):294-313. [Google Scholar]
[5]. Demyer W, Zeman W, Alobar holoprosencephaly (arhinen- cephaly) with median cleft lip and palate: clinical, electroen- cephalographic and nosologic considerationsConfin Neurol 1963 23:1-36. [Google Scholar]
[6]. Demyer W, Zeman W, Palmer CG, The Face Predicts the Brain: Diagnostic Significance of Median Facial Anomalies for Holoprosencephaly (Arhinencephaly)Pediatrics 1964 34:256-63. [Google Scholar]
[7]. Delezoide AL, Narcy F, Larroche JC, Cerebral midline developmental anomalies: spectrum and associated featuresGenet Couns 1991 1(3-4):197-210. [Google Scholar]
[8]. Stevenson AC, Johnston HA, Stewart MIP, Congenital malformation: A report of a report of a study of series of consecutive births in 24 centresBull WHO 1966 34(Suppl):1-27. [Google Scholar]
[9]. Leech RW, Bowlby LS, Brumback RA, Schaefer GB, Agnathia, holoprosencephaly, and situs inversus: report of a caseAm J Med Genet 1988 29:483-90. [Google Scholar]
[10]. Wright S, On the genetics of subnormal development of the head (otocephaly) in the guinea pigGenetics 1933 19:471-503. [Google Scholar]
[11]. Wright S, Wagner K, Types of subnormal development of the head from inbred strains of guinea pigs and their bearing on the classification and interpretation of vertebrate monstersAm J Anat 1934 54:383-447. [Google Scholar]
[12]. Hersh JH, McChane RH, Rosenberg EM, Powers WH, Corrigan C, Pancratz L, Otocephaly-midline malformation Hersh JH associationAm J Med Genet 1989 34:246-49. [Google Scholar]
[13]. Kauvar EF, Solomon BD, Curry CJ, Essen AJ, Janssen N, Dutra A, Holoprosencephaly and Agnathia Spectrum: Presentation of Two New Patients and Review of the LiteratureAm J Med Genet C Semim Med Genet 2010 154C(1):158-69. [Google Scholar]
[14]. Faye-Petersen O, David E, Rangwala N, Seaman JP, Hua Z, Heller DS, Otocephaly: report of five new cases and a literature reviewFetal Pediatr Pathol 2006 25:277-96. [Google Scholar]
[15]. Özden S, Bilgiç R, Delikara N, Baaran T, The sixth clinical report of a rare association: agnathia-holoprosencephaly-situs inversusPrenat Diagn 2002 22:831-42. [Google Scholar]
[16]. Meinecke P, Padberg B, Laas R, Agnathia, holoprosencephaly, and situs inversus: a third reportAm J Med Genet 1990 37:286-87. [Google Scholar]
[17]. Robinson HB, Lenke R, Agnathia, holoprosencephaly, and situs inversusAm J Med Genet 1989 34:266-67. [Google Scholar]
[18]. Roessler E, Ouspenskaia MV, Karkera JD, Vélez JI, Kantipong A, Lacbawan F, Reduced NODAL signaling strength via mutation of several pathway members including FOXH1 is linked to human heart defects and holoprosencephalyAm J Hum Genet 2008 83:18-29. [Google Scholar]
[19]. Cohen M, Shiota K, Teratogenesis of HoloprosencephalyAm J Med Genet 2002 109:1-15. [Google Scholar]
[20]. Ming JE, Muenke M, Holoprosencephaly: from Homer to HedgehogClin Genet 1998 53:155-63. [Google Scholar]
[21]. Tsukui Tohru, Multiple left-right asymmetry defects in Shh−/− mutant mice unveil a convergence of the Shh and retinoic acid pathways in the control of Lefty-1Proceedings of the National Academy of Sciences 1999 96(20):11376-81. [Google Scholar]
[22]. Kietzman HW, The Teratogenic Effects of Prenatal Ethanol Exposure Are Exacerbated by Sonic Hedgehog or Gli2 Haploinsufficiency in the MousePlos one 2014 9(2):e89448 [Google Scholar]