Introduction
The number of people with diabetes mellitus (DM) is increasing [1]. DM is one of the most common diseases globally, had affected 285,000,000 peoples in 2010 in the world. It is estimated that DM will affect 592,000,000 persons in 2035 [1,2]. In Iran, 8.43% of population aged 20 to 79 y (4395938 people) had DM in 2013 [2]. Diabetic Ketoacidosis (DKA) is one of emergency conditions caused by acute hyperglycemia which may be associated with both type 1 and 2 diabetes, mostly type 1 and is the cause for 10,000 to 160,000 hospitalizations in US [3-5]. DKA is a life-threatening condition in which the severe insulin deficiency causes hyperglycemia, severe lipolysis, uncontrolled oxidation of fatty acids and ketone bodies (beta-hydroxy-butyrate, acetoacetate and acetone) formation. The process results in metabolic acidosis, dehydration and loss of body electrolytes [6].
The basic treatment of DKA is injection of rapid-acting RI. Intravenous infusion of RI is the preferred method of treatment until recovery from DKA. Then, the treatment is continued with subcutaneous injection of insulin [5]. Intravenous RI has short half-life as a few minutes, requires the infusion pump and is associated with hospitalization and nursing costs [7].
GI is a long acting insulin which is injected subcutaneously once daily in patients with type 1 or 2 DM; its onset of action is about an hour and create a relatively stable concentration of insulin in 24 hour [7,8]. Given these pharmacodynamics of GI, it seems that addition of these long acting insulin to standard regimen my facilitated the transition from intravenous infusion of insulin to subcutaneous injection in the recovery of patients with DKA [9], so that the British Diabetes Association (BDA) recommends that in DKA patients using long-acting insulin (glargine o Detemir) prior to DKA, it must be continued with the same dosage in the phase of DKA [10].
Moreover it has been reported that subcutaneous injection of 0.2 unit/kg GI along with infusion of RI is safe [11]. Regarding the short half-life of intravenous insulin and risk of technical errors including transient pause of infusion pump which adversely affect the recovery process of DKA, it seems that adding long-acting insulin to the standard regimen of treatment can prevent these complications [7]. This study was aimed to investigate the effect of adding GI to the standard regimen on the recovery process of patients with DKA.
Materials and Methods
A randomized clinical trial (RCT) was conducted on 40 patients with DKA admitted in Endocrinology and Metabolism Ward of Tabriz Imam Reza Hospital since March 2013 to Jan 2014. Sample size was determined according to reference 4 data, using an online Sample size Calculator.
Inclusion criteria were definitive diagnosis of DKA according the American Diabetes Association criteria, age >12y, and consent to participate in the study. Exclusion criteria were persistent hypotension (SBP<80 mmHg in spite of receiving 1000cc saline normal), acute MI, progressive renal or hepatic failure, the need for emergency surgery, pregnancy, and the lack of consent for participation in the study. The laboratory diagnosis of DKA was made as blood sugar >13.9 mmol/l, serum bicarbonate <18 mmol/lit, pH<7.3, and presence of ketone bodies in serum or urine [5].
The recovery from DKA was documented by laboratory findings of blood sugar <13.9 mmol/l, serum bicarbonate >15 mmol/lit and pH>7.3. Rebound hyperglycemia was defined as BS >10 mmol/l up to 24 hours after discontinuation of RI, and hypoglycemia was defined as BS <3.9 mmol/l. The enrolled subjects were randomized according to their medical record number (odd vs. even) in one of Intervention or Control groups each encompassing 20 patients.
The patients in control group received the standard treatment regimen for DKA including continuous IV infusion of RI. The patients in intervention group received the standard regimen of DKA in addition with long-acting insulin Glargine (made by SANOFI®) subcutaneously (0.4 U/kg) within three hours after RI infusion, and the dose of GI was repeated every 24 h until recovery from the DKA [5].
In both groups, with approaching of BS to less than 13.9 mmol/l IV fluids changed to 150-250 ml/h of half normal saline and dextrose with a concentration that maintain BS in the range of 8.3– 13.9 mmol/l. The next steps of the treatment was same in both groups, including monitoring of laboratory and clinical findings using “modified DKA flow sheet”, and recording the related parameters in a questionnaire.
The total required insulin and the time to recovery from DKA was assessed and compared between the study groups. The one hour overlaps between the first subcutaneous injection of RI and infusion of insulin was considered, and in order to regularity and equality of intervals of subcutaneous injections, the infusion was paused in one of hours 6, 12, 18, or 24. Up to 24 h, the patients received subcutaneous RI 0.5 to 0.8 U/kg/day divided in four doses (6-12 U/6h). BS was checked before each injection of insulin and if BS was above than7.8 mmol/l, 2 units of RI were added for any 2.2 mmol/l (up to 12 units). All patients or their relatives signed the informed consent before the study. All patients were treated according the therapeutic protocol for DKA. No further costs were paid by patients and the cost of GI was provided by researchers. This study was confirmed by local academic ethical committee (no: 9212; date: April 3, 2013) and registered in Iranian Registry of Clinical Trials website (IRCT2013050713258N1).
Statistical Analysis
SPSS-17 win software used for statistical analysis. The collected data were analysed using descriptive statistical methods including frequency, percent and average ± SD. The comparisons between the study groups were made by using Chi-square test or Fisher's exact test for comparison of qualitative variables and independent t-test for quantitative variables. The normal distribution of data was assessed by Kolmogorov Simonov test. The p-values less than 0.05 were considered as significant.
Results
[Table/Fig-1] shows basic patient characteristics of both groups. DKA precipitating factors: Of all patients, 16 (7 in intervention and 9 in control group) were newly identified cases of DM. In 17 patients (11 in intervention and 6 in control group), DKA was occurred due to non-adherence to DM control modalities and inappropriate use of insulin. In remaining 7 patients the reasons for DKA were acute pancreatitis and pyelonephritis in 2 subjects of intervention group; and pneumonia, infection of diabetic foot, common cold, sinusitis, pyelonephritis, and gastroenteritis in 5 of controls.
[Table/Fig-2] shows basic laboratory parameters in patients of both groups. Ketonuria was 1+ in two patients in control group and ≥2+ in all other patients.
The time needed for lowering BS to less than 13.9 mmol/l was 5.3±2.1 h in intervention and 5.2±2.2 h in control group (p=0.88). Hypokalemia during treatment was occurred in three patients in control group and in four of interventions. Hypoglycemia (BS<3.9mmol.l), was occurred as seven episodes in five patients in intervention group and four episodes in four patients in control group. The mean dosage of RI until recovery from DKA was 84.8±45.6 units in intervention group and 116.5±91.6 units in control group (p=0.17). The mean amount of intravenous fluid infusion was 5141.25±1245.76 ml in intervention group and 5592.50±1335.27 ml in control group (p=0.276).
The mean duration of correction of acidosis and recovery from DKA was 13.77±6.10 hours in intervention group and 16.91±6.49 h in control group (p=0.123).
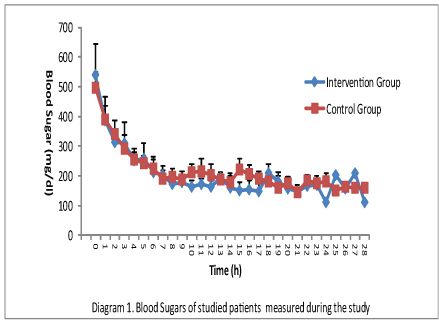
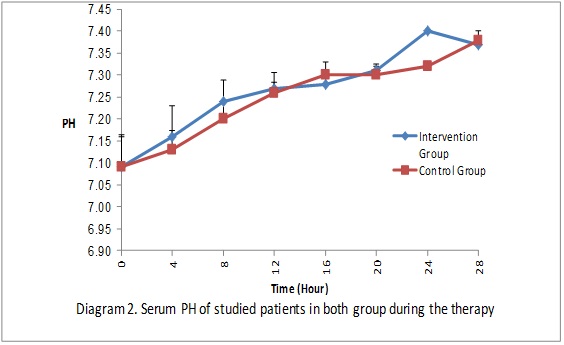
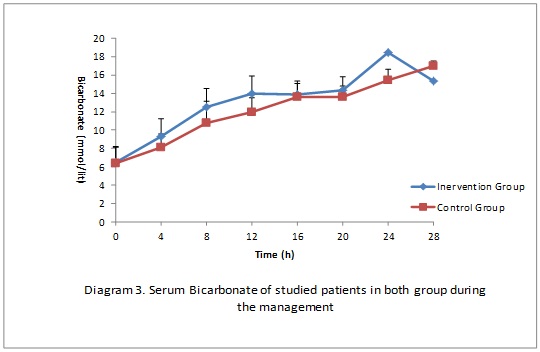
Occurrence of BS>8.3 mmol/l in first 24 hours after discontinuation of the insulin infusion (rebound hyperglycemia): Averagely, in 1.4±1.04 samples (35% of four checked samples) in intervention group and in 2.05±0.94 samples (51% of four checked samples), the BS was more than 8.3 mmol/l for 24 h after discontinuation of the insulin infusion (p=0.046). The mean duration of hospitalization was 5.1±1.88 days in intervention and 5.9±2.19 days in control group (p=0.225). Two patients in intervention group and one in control group received bicarbonate. The changes in serum bicarbonate, pH, and glucose during the management until recovery from DKA have been shown in [Table/Fig-3,4,5].
Discussion
DKA is one of acute and serious complications of diabetes mellitus has showed a global increase in incidence in past decades that may be greatly due to increase in the diagnosis of DM [12]. Two-thirds of patients with DKA have type 1 diabetes and 34% have type 2. In approximately 20-40% of children with DM, DKA occurs before the diagnosis of diabetes [5,12,13].
Management of DKA requires correction of dehydration, hyperglycemia, electrolyte abnormalities, diagnosis and treatment of precipitating factors and more importantly careful patient monitoring [5]. Due to fears of insulin resistance, until 1972, it was thought that high doses of insulin (greater than or equal to 100 units per hour, as IV or subcutaneous) to be necessary in the treatment of DKA [14-16]. In the 1970s, several reports were released about the effectiveness of low doses of insulin [17,18]. There are plenty of reports about effectiveness of analog insulins in management of DKA. Umpierrez et al., divided 40 patients with DKA into two groups of 20 patients; one group received intravenous RI and the other underwent subcutaneous injection of short-acting insulin Lispro. The time of recovery from DKA in two groups was not significantly different (11±4 and 10±3 h, respectively) [19]. In another trial Umpierrez et al., classified 45 patients with DKA in three groups of 15 patients to compare subcutaneous insulin aspartate every 1h and every 2h with infusion of insulin. There was no significant difference between the groups about the time of recovery from DKA, amount of needed insulin, hypoglycemia attacks (one attack in every group), and the duration of hospitalization were similar (6.9±4, 6.1±4 and 7.1±5 days) [20].
Eroz et al., divided 20 patients with DKA into two groups of 10 patients; one group received intravenous RI and the other underwent subcutaneous injection of insulin Lispro. The time of recovery from DKA were similar in both groups (13.2±7.5 h and 14.8±7 h) [21]. Della et al., evaluated the efficacy of short-acting insulin in DKA patients and suggested that it is effective, cost effective, and safe in the management of DKA [22].
Unlike short-acting analogues of insulin, there are few published studies about the impact of long-acting analogues in the treatment of DKA. Shankar et al., compared 12 children with moderate to severe DKA who received GI 6 h after initiation of intravenous RI, with 59 children who only received intravenous insulin, about variables such as time of recovery from DKA, amount of needed I.V. insulin, and suggested that adding GI to standard treatment reduced the time of recovery from DKA and amount of required insulin significantly. The time of recovery from DKA was 17.1±2.6 in standard group and 12.4±2.9 h in intervention group (p<0.001) [4].
In another study, Parker et al., analysed 27 DKA episodes in hospitalized patients, and concluded that patients who received long-acting insulin (glargine, Detemir) in addition to standard regimen had significant decrease in the duration of hospitalization (p=0.02) [8].
Hsia et al., conducted a prospective study on 61 patients with diabetes (25 with DKA) to assess if giving subcutaneous GI in addition to intravenous infusion of RI, may prevent rebound hyperglycemia after insulin discontinuation. Until 12 h after discontinuation of the insulin infusion, at least one BS>8.3 mmol/l (rebound hyperglycemia) was seen in 33.3% in intervention group (receiving intravenous RI plus glargine), and in 93.5% in control group (only intravenous insulin) (p<0.001). They concluded that addition of GI to intravenous insulin is a safe protocol that significantly prevent rebound hyperglycemia and do not increase the risk of hypoglycemia [11].
Marshall et al., studied on animal model with DKA to evaluate the effects of GI subcutaneously or intramuscularly in DKA, and suggested that GI is an effective medication in DKA [23]. In a study by Doshi et al., on 40 patients with DKA (21 patients in control and 19 in intervention group), both groups received standard treatment for DKA. The intervention group received GI 0.3 unit/kg subcutaneously in addition to standard treatment of DKA, in first two hours after the diagnosis of DKA. The main objective of this study was comparison of the time to reach to corrected anion gap and there was not a significant difference between the two groups (11.6±8.2 h in interventions and 13±8.5 h in control group, p=0.48) [24].
Most patients with DKA (56%) are between 18-44 y, 24% are between 45-65 y and 18% under 20 y [5]. In our study 55% of people aged 18-44 y, 25% between 44-65 y and 20% under 18 y, which is similar to the previously reported percentages.
Two-thirds of patients with DKA have type 1 diabetes and 34% type 2 diabetes; 50% are female [5,11,12]. DKA is the first leading cause of mortality in children and teenagers with type- I-DM, and constitute the cause of half of patients with diabetes mortality in ages less than 24 y [25,26]. In adult DKA patients, mortality from DKA is less than 1% [12], but mortality more than 5% has been reported in elderly individuals having a life-threatening disease [27,28]. As expected in this study, most of patients with DKA had type 1 diabetes (82%) and 17% had type 2 diabetes. Fifty five present of our studied patients were female, and fortunately none of the patients died, and the mortality rate was zero. The mean BMI was 21.06 kg/m2 in intervention and 22.29 kg/m2 in control group, and given that only 17.5% of patients had type 2 diabetes, low BMI is justified.In our series, 40% of patients had newly diagnosed diabetes and 42% had the history of poor compliance and inappropriate use of insulin. Diagnosis of Type-I-DM is made in 8.7 to 80% after the DKA occurs [29,30]. It seems that lack of obvious expression of symptoms in children, unawareness of parents and health care providers with DKA manifestations can increase the incidence of DKA before the diagnosis of DM [31].
Because we did not enrolled patients less than 12 y, difficulty in expression of symptoms cannot explain the relatively high percent of newly diagnosed DM. This problem is due to unawareness of parents with DKA manifestations and disability of medical personnel in the diagnosis of diabetes and DKA at appropriate time.
The use of low-dose insulin in DKA therapy is associated with fewer metabolic complications such as hypokalemia and hypoglycemia than with large, intermittent dose [32]. In none of three studies in which GI was used as the main insulin in the treatment of DKA [4,8,24], the incidence of hypokalemia during treatment has not been reported. In our study 15% of patients in control group and 20% of patients in intervention group affected by mild hypokalemia during the treatment. In this regard, it is obvious that Glargine is safe and does not increase the incidence of hypokalemia during DKA therapy.
Of three studies mentioned above, the incidence of hypoglycemia during treatment has been evaluated in two studies [4,24]. In the study of Shanker et al., there were not any hypoglycemic event during the management of DKA (either in group receiving regular infusion or group receiving regular infusions plus glargine) [4]. In the study by Doshi et al., four hypoglycemic episodes occurred in three patients in intervention group and two episodes in two patients in the control group [24]. In our study, seven episodes of hypoglycemia occurred in five patients in intervention group and four episodes in four patients in control group. We can conclude that adding glargine with dose of 0.4unit/kg to standard therapy of DKA does not increase significantly the incidence of hypoglycemia.
In our study, the mean total amount of intravenous insulin used until recovery from DKA was 84.8 units in intervention and 116.5 units in control group. We can explain the much higher intravenous RI requirement in our study in comparison with the study of Shanker et al., [4] in two way: our patients were adults but they performed that study on children and teenagers, and in our study, after reaching the blood sugar level of 250 mg/dl we gave 5-15% dextrose to prevent need for reduction of insulin dosage as much as possible till to recovery from DKA.
The average duration of correction of acidosis has reported as 12 h [5]. In the study Shanker et al., [4], this time was 12.4 h in intervention group and 17.1 h in controls (p<0.001). Doshi et al., [24] selected the time to reach the corrected anion gap as the primary objective which was 11.6 h in intervention group (group treated with infusion of RI plus glargine) and 11.7 h in control group (only regular infusions) (p=0.48).
In studies comparing intravenous RI with rapid-acting subcutaneous insulin analogues [28-31] the duration of acidosis correction was 10-18 h in intervention group (rapid-acting insulin only) and 11-13.2 h in control group (only intravenous RI).
In our study, the duration of acidosis correction and recovery from DKA was 13.77 h in intervention and 16.91 h in control group. As mentioned earlier, the initial value of pH and HCO3 in our patients was lower than previously reported values [5] and this justify that the duration of acidosis correction to be more than 12 h. Although in our study, the patients in intervention group were recovered 3.1 h earlier from DKA, this difference was not statistically significant (p=0.123). In the study of Doshi et al., [24] also the time of reaching to the anion gap correction point was not significantly different between two groups (p=0.48).
It seems that the difference between the findings of Doshi et al., [1], and our study and results of Shanker et al., [4] to be related to the sample size. Both in our study and the study of Doshi et al., [24], 40 subjects were enrolled in comparison with 71 subjects in the study of Shanker et al., [4]. Furthermore, in our and Doshi et al., study, the number of patients in both groups was equal while in the study of Shanker et al., [4] the intervention group constitutes 12 and the control group had 59 patients.
The study of Hsia et al., up to12 h after discontinuation of the insulin infusion, at least one BS>8.3 mmol/l (rebound hyperglycemia) was seen in 33.3% in intervention group (receiving intravenous RI plus glargine), and in 93.5% in control group (only intravenous insulin) (p<0.001) [11].
In our study, in 24 h after discontinuation of the insulin infusion, at least one BS>8.3 mmol/l (rebound hyperglycemia) was seen in 85% in intervention and in 95% in control group. However, the mean rate of rebound hyperglycemia was 35% in intervention and 51% in control which is statistically significant (p=0.045). This is attributable to long half-life of GI and continuation of its effect for many hours after discontinuing of RI.
Duration of hospitalization has reported 3.4 to 4.8 days in most studies [19,20] without significant difference between intervention and control groups. In our study, the mean duration of hospitalization was 5.1 days in intervention and 5.9 days in control group (p=0.2).
| Patient Characteristics | Group | p |
|---|
| Intervention | Control |
|---|
| Age*(y) | 29.65±13.60 | 29.25±15.69 | 0.932 |
| Sex(M/F) | 9/11 | 9/11 | - |
| Weight*(kg) | 55.90±10.41 | 59.17±13.75 | 0.401 |
| BMI*(kg/m2) | 21.06±2.92 | 22.29±3/42 | 0.32 |
| T1DM | 17 | 16 | - |
*:Data are means± SD
Laboratory findings of patients in admission
| Laboratory findings | Group | p-value |
|---|
| Intervention | Control |
|---|
| Blood Sugar (mmol/l) | 30±11.6 | 27.63±5.7 | 0.413 |
| Serum PH | 7.09±0.15 | 7.09±0.14 | 0.974 |
| HCO3 (mmol/l) | 6.51±3.34 | 6.37±3.49 | 0.901 |
| Creatinine (μmol/l) | 12.9±2.56 | 12.53±3.26 | 0.742 |
| BUN (mmol/l) | 7.38±2.46 | 7.29±3.4 | 0.919 |
| K (mmol/l) | 4.65±0.74 | 4.59±0.59 | 0.795 |
| Na (mmol/l) | 136.95±3.59 | 137.10±4.73 | 0.911 |
| HbA1c (%) | 12.31±2.40 | 12.78±2.41 | 0.574 |
*The variables has been showed as means± SD
Blood sugars of studied patients measured during the study
Serum pH of studied patients in both goup during the therapy
Serum bicarbonate of studied patients in both group during the management
Limitations of Study
This was a RCT conducted on two study groups with the same demographic variables, laboratory parameters and covered the patients with any severity of DKA (mild, moderate and severe), in which for the first time, the highest dose of GI (0.4unit/kg) along with intravenous injection of RI was used and it was concluded that this dose is safe. Previous studies had reported use of maximum 0.3unit/kg. However, this study has some limitations such as small sample size, non-using placebo for control group and lack of blinding.
Conclusion
Adding GI to the standard treatment regimen of DKA reduced the average time of recovery from DKA to 3.1 h, without incurring episodes of hypoglycemia and hypokalemia, however this change was not statistically significant. This also significantly reduced BSs above 8.3 mmol/l up to 24 h after discontinuation of insulin infusion, but did not affect the duration of hospitalization. It seems that the non-significant difference in the time of recovery from DKA be related to the small sample size and close monitoring of DKA patients in both groups which resulted in fine adjustment of insulin and fluid intake.
It seems that adding GI to treatment protocol of DKA in non-RCT setting (without the direct involvement of researcher in the treatment) in general wards may show more pronounced effects. It is recommended that studies with larger sample size to be conducted in multiple centers about the effect of GI in the management of DKA patients.
*:Data are means± SD
*The variables has been showed as means± SD
[1]. S Wild, G Roglic, A Green, R Sicree, H King, Global prevalence of diabetes: estimates for the year 2000 and projections for 2030Diabetes Care 2004 27(5):1047-53. [Google Scholar]
[2]. International Diabetes Federation. 2014 [ cited 2014 April 15] Available from: http://www.idf.org/diabetesatlas/introduction [Google Scholar]
[3]. GE Umpierrez, S Jones, D Smiley, P Mulligan, T Keyler, A Temponi, Insulin analogs versus human insulin in the treatment of patients with diabetic ketoacidosis: a randomized controlled trialDiabetes Care 2009 32(7):1164-69. [Google Scholar]
[4]. V Shankar, A Haque, KB Churchwell, W Russell, Insulin glargine supplementation during early management phase of diabetic ketoacidosis in childrenIntensive Care Med 2007 33(7):1173-78. [Google Scholar]
[5]. AE Kitabchi, GE Umpierrez, JM Miles, JN Fisher, Hyperglycemic crises in adult patients with diabetesDiabetes Care 2009 32(7):1335-43. [Google Scholar]
[6]. G Eisenbarth, J Buse, Type 1 Diabetes Mellitus. In: Melmed SH, Kenneth SP, Larsen PR, Kronenberg HM. Williams Textbook of Endocrinology 2011 12th EditionPhiladelphiaSaunders Elsevier:1453-61. [Google Scholar]
[7]. M Mazer, E Chen, Is subcutaneous administration of rapid-acting insulin as effective as intravenous insulin for treating diabetic ketoacidosis?Ann Emerg Med 2009 53(2):259-63. [Google Scholar]
[8]. V Parker, Outcomes in adult patients with diabetic ketoacidosis treated on sliding scale insulin with and without supplemental background long acting subcutaneous insulinAbstracts from 8th Congress of the European Federation of Internal Medicine / European Journal of Internal Medicine 2009 20S:S1-S283. [Google Scholar]
[9]. L Barski, L Kezerle, L Zeller, M Zektser, A Jotkowitz, New approaches to the use of insulin in patients with diabetic ketoacidosisEur J Intern Med 2013 24(3):213-16. [Google Scholar]
[10]. MW Savage, K Dhatariya, A Kilvert, G Rayman, JA Rees, CH Courtney, Joint British Diabetes Societies Guideline for the management of diabetic ketoacidosis Diabetes Medicine 2011 28:508-15. [Google Scholar]
[11]. E Hsia, S Seggelke, J Gibbs, RM Hawkins, E Cohlmia, N Rasouli, Subcutaneous Administration of Glargine to diabetic patients receiving insulin infusion prevents rebound hyperglycemiaJ Clin Endocrinol Metab 2012 97(9):3132-37. [Google Scholar]
[12]. V Greet, Acute Endocrinology: From Cause to ConsequenceTetracyclineTeratology 2008 New YorkHumana Press:123-24. [Google Scholar]
[13]. R Alemzadeh, O Ali, Type 1 Diabetes Mellitus (Immune Mediated). In: Kleigman RM, Stanton BF, Gem JW, Schor NF, Behrman RE, editors. Nelson text book of Pediatric 2011 19th EditionPhiladelphiaSaunders Elsevier:1969-90. [Google Scholar]
[14]. JM Malinsn, The management of diabetic comaJ R Coll Physicians Lond 1971 6(1):75-82. [Google Scholar]
[15]. HF Rooth, The use of insulin and abuse of glucose in the treatment of diabetic comaJAMA 1945 127(10):557-64. [Google Scholar]
[16]. AB Kitabchi, Low-dose insulin therapy in diabetic ketoacidosis: fact or fiction?Diabetes Metab Rev 1989 5(4):337-63. [Google Scholar]
[17]. HS Sacks, M Shahshahani, AE Kitabchi, JN Fisher, RT Young, Similar responsiveness of diabetic ketoacidosis to low-dose insulin by intramuscular injection and albumin-free infusionAnn Intern Med 1979 90(1):36-42. [Google Scholar]
[18]. KM Piters, D Kumar, E Pei, AN Bessman, Comparison of continuous and intermittent intravenous insulin therapies for diabetic ketoacidosisDiabetologia 1977 13(4):317-21. [Google Scholar]
[19]. GE Umpierrez, K Latif, J Stoever, R Cuervo, L Park, AX Freire, Efficacy of subcutaneous insulin lispro versus continuous intravenous RI for the treatment of patients with diabetic ketoacidosisAm J Med 2004 117(5):291-96. [Google Scholar]
[20]. GE Umpierrez, R Cuervo, A Karabell, K Latif, AX Freire, AE Kitabchi, Treatment of diabetic ketoacidosis with subcutaneous insulin aspart 2004 27(8):1873-78. [Google Scholar]
[21]. HO Ersöz, K Ukinc, M Köse, C Erem, A Gunduz, AB Hacihasanoglu, Subcutaneous lispro and intravenous RI treatments are equally effective and safe for the treatment of mild and moderate diabetic ketoacidosis in adult patientsInt J Clin Pract 2006 60(4):429-33. [Google Scholar]
[22]. MT Della, L Steinmetz, PR Campos, SC Farhat, C Schvartsman, H Kuperman, Subcutaneous use of a fast-acting insulin analog: an alternative treatment for pediatric patients with diabetic ketoacidosisDiabetes Care 2005 28(8):1856-61. [Google Scholar]
[23]. RD Marshall, JS Rand, MN Gunew, VH Menrath, Intramuscular glargine with or without concurrent subcutaneous administration for treatment of feline diabetic ketoacidosisJ Vet Emerg Crit Care (San Antonio) 2013 23(3):286-90. [Google Scholar]
[24]. PB Doshi, AJ Potter, D Santos, BF Darger, V Patel, V Chathampally, Prospective Randomized Trial of GI in Acute Management of Diabetic Ketoacidosis in the Emergency Department: A Pilot StudyAnnals of Emergency Medicine 2013 62(4):133 [Google Scholar]
[25]. J Wolfsdorf, N Glaser, MA Sperling, Diabetic ketoacidosis in infants, children, and adolescents: a consensus statement from the American Diabetes AssociationDiabetes Care 2006 29(5):1150-59. [Google Scholar]
[26]. NH White, Diabetic ketoacidosis in childrenEndocrinol Metab Clin North Am 2000 29(14):657-82. [Google Scholar]
[27]. EJ Graves, BS Gillium, Detailed diagnoses and procedures, National Hospital Discharge Survey, 1995Vital Health Stat 1997 13(130):1-146. [Google Scholar]
[28]. ML Malone, V Gennis, JS Goodwin, Characteristics of diabetic ketoacidosis in older versus younger adultsJ Am Geriatr Soc 1992 40(11):1100-04. [Google Scholar]
[29]. V Sadauskaite-Kuehne, U Samuelsson, E Jasinskiene, Z Padaiga, B Urbonaite, H Edenvall, Severity at onset of childhood type 1 diabetes in countries with high and low incidence of the conditionDiabetes Res Clin Pract 2002 55(3):247-54. [Google Scholar]
[30]. J Punnose, MM Agarwal, A El Khadir, K Devadas, IT Mugamer, Childhood and adolescent diabetes mellitus in Arabs residing in the United Arab EmiratesDiabetes Res Clin Pract 2002 55(1):29-33. [Google Scholar]
[31]. M Rodacki, JR Pereira, AM Nabuco de Oliveira, B Mac Dowell, R Perricelli, Ethnicity and young age influence the frequency of diabetic ketoacidosis at the onset of type 1 diabetesDiabetes Res Clin Pract 2007 78(2):259-62. [Google Scholar]
[32]. J Wyckoff, M Abrahamso, Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in: Kahn RC, Weir GC, King G, Moses AC, Smith RJ, Jacobson AM. Joslin’s Diabetes Mellitus 2005 14th EditionPhiladelphiaLippincott Williams and Wilkins:887-901. [Google Scholar]