Cadaveric Study of Profunda Femoris Artery with Some Unique Variations
Sangeeta Jitendra Rajani1, Minal K Ravat2, Jitendra K Rajani3, Amul N Bhedi4
1 Associate Professor, Department of Anatomy, Medical College, Baroda, Gujarat, India.
2 Tutor, Department of Anatomy, Medical college, Baroda, Gujarat, India.
3 Professor & Head, Department of Oral Pathology & Microbiology dept, Faculty of Dental Sciences, Nadiad, India.
4 Associate Professor, Department of Surgery, Medical College, Baroda, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sangeeta Jitendra Rajani, Sakhar Co-op Housing society, Harni warashia Ring road, Near shiv vatika, b/H omkar Hospital, Vadodara-390006, Gujarat, India. E-mail : sangeetarajani73@yahoo.co.in
Background
Profunda femoris artery is the largest branch of femoral artery and chief supply of the thigh. It is useful for various clinical procedures like arteriography, ultrasonography and Doppler imaging and haemodialysis. Hence, accurate anatomical knowledge is very important for the clinicians.
Materials and Methods
Thirty three properly embalmed cadavers (17 males and 16 females) were selected for the study. Femoral artery, Profunda femoris artery and its branches were exposed and their distances of origin were measured.
Results
In present study of profunda femoris artery, we found posterolateral and lateral aspect of origin was common (71.21%) than posterior and posteromedial aspect of origin (24.24%). The site of origin of profunda femoris artery was between 21-40 mm on right side and 11-40 mm on left side. In 14 limbs (21.21%), we found high origin of profunda femoris artery (distance < 10mm). In two limbs (3.03%) Profunda femoris artery was originating from medial side of femoral artery and it coursed superficial to femoral vein. As per various literatures this is rare. In one female cadaver, on left side, we noted high origin (5mm away from mid inguinal point) of profunda femoris artery and site of origin was from anterolateral aspect of femoral artery and all the superficial branches of thigh took origin from it, while on right side of same cadaver findings were normal. In 13 limbs (19.69%) profunda femoris artery took origin as a common stem along with one of circumflex arteries while in three limbs (4.54%) trifurcation was observed, that is origin of profunda femoris and two circumflex arteries from single site. In four limbs (6.06%), superficial branches of femoral artery took origin from profunda femoris artery instead of femoral artery.
Conclusion
In present study posterolateral and lateral side of origin is noted as common site of origin of profunda femoris artery. Rare variation like medial side origin of profunda Femoris artery was observed and it coursed on femoral vein. Very high incidence of high level of origin of profunda femoris artery was found. In one of the high origin limb profunda femoris artery originated from anterolateral side and all superficial branches of thigh took origin from it. Such variation is unique. Hence, this study will help the clinicians to avoid iatrogenic complications and also help them in various clinical procedures like puncture of femoral artery for interventional radiology.
Circumflex arteries, Femoral Artery, Variations
Introduction
Variation in pattern of femoral artery (FA) and its branches are clinically very important. Hence it has received attention from various anatomists and surgeons.
Profunda femoris artery (PFA) is the largest deep branch of FA, provides the principal supply to the extensors, adductors and flexors muscles of thigh [1]. It arises laterally from the FA about 3.5 cm distal to the inguinal ligament , then it spirals posterior to the artery and femoral vein (FV) to reach medial side of femur [2]. It gives muscular branches, circumflex femoral arteries, perforating arteries. Clinicians call FA as a common FA above the origin of PFA and superficial FA below the origin of PFA [3].
Interventional radiology opens new avenues for the study of variations of the courses of the PFA. Femoral angiography is the main line for the investigations in the peripheral occlusive arterial disease and its diagnosis of suspected congenital anomalies. For the same FA is commonly used for these procedures [4].
The anatomical knowledge of the level of origin of PFA is important in avoiding iatrogenic femoral arterio-venous fistula formed during puncture of femoral artery [5]. PFA used for haemodialysis, vascular reconstructive procedures and various Radio Imaging techniques like Ultrasound Doppler Imaging and MRI [6,7].
Hence, accurate knowledge of anatomical variations regarding origin of PFA and circumflex femoral arteries are very important for clinicians. Precise anatomy of PFA forms strong foundation to minimize complications. Aim of this study is to find out the site and level of origin of PFA and any variations related to site, distance and branching pattern of PFA.
Materials and Methods
Thirty three properly embalmed and formalin fixed adult cadavers (17 males and 16 females) were selected for the present study. Sixty six femoral triangles were dissected. FA, PFA and its branches were exposed and the site of origin of PFA from FA noted. The distance of origin of PFA from the midpoint of inguinal ligament was measured with the help of digital vernier caliper in mm.
The origin of medial and lateral circumflex arteries from PFA or FA noted and distance of their sites of origin from the origin of PFA (if originated from PFA) or from midpoint of inguinal ligament (if originated from FA) were measured in millimeters (mm). The observed variations were photographed and noted.
Results
Regarding the origin site and pattern of origin of PFA
Refer [Table/Fig-1,2].
In medial side origin PFA runs superficial to the FV [Table/Fig-3].
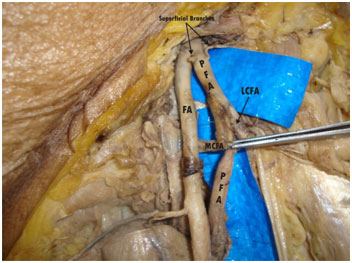
PFA lies superficial as compared to FA in antero-lateral aspect of origin. All superficial branches of thigh originated from PFA [Table/Fig-4].
In case of origin of MCFA from PFA origin site remains very close to PFA origin.
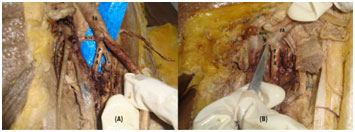
In three limbs, PFA and two circumflex arteries originating as a common stem from FA. Such cases labeled as trifurcation. In such cases course was typical. Horizontal medial running branch of common stump was continuing as MCFA, while main trunk was further dividing into lateral division and medial division. Lateral one was LCFA and medial division was PFA [Table/Fig-5a].
In one cadaver bilateral trifurcation seen. On left side toursous course of LCFA in proximal few mm [Table/Fig-5b].
Shows site of origin of PFA
| Site of origin of PFA from FA | No. of cases | Percentage (%) | Remark |
|---|
| Posterolateral side | 35 | Total 47 | 53.03 | Total 71.21 | Commonest site |
| Lateral side | 12 | 18.17 |
| Posteromedial side | 9 | Total 16 | 13.63 | Total 24.24 | Second Commonest site |
| Posterior side | 7 | 10.61 |
| Medial side | 2 | 3.03 | Rare variation |
| Anterolateral side | 1 | 1.51 | Unique finding |
| Total | 66 | 99.99 | --------- |
Shows pattern of origin of PFA
| Pattern of origin Of PFA | Total Cases | Percentage (%) | Origin of LCFA | Origin of MCFA |
|---|
| Common Origin with LCFA | 7 | 10.60 | From FA | 6 from PFA 1 from FA |
| Common Origin with MCFA | 6 | 9.09 | 4 from PFA 2 from FA | From FA |
| Common Origin with both of circumflex arteries (trifurcation) | 3 | 4.54 | From FA | From FA |
LCFA- Lateral circumflex femoral artery. MCFA – medial circumflex femoral artery
High origin of Profunda Femoris artery (PFA) from medial side of Femoral Artery (FA)

High origin of Profunda Femoris artery (PFA) from anterolateral side of Femoral artery (FA) with all superficial branches and circumflex arteries from PFA, MCFA (medial circumflex femoral artery) & LCFA (lateral circumflex femoral artery)
Common origin of Profunda Femoris artery (PFA) with two circumflex arteries (MCFA & LCFA) from femoral artery (FA), (A) Typical course of three arteries (B) Lateral circumflex femoral artery (LCFA) with tortuous course in initial part
Regarding distance of origin of PFA and superficial branches of thigh
Refer [Table/Fig-6,7].
Commonest range of origin of PFA was between 21mm to 40 mm on right side and between 11 mm-40 mm on left side.
When PFA is of equal in size to FA, both circumflex arteries originated from PFA.
Medial side origin of PFA is rare. In such case PFA was running for a short distance on medial side of FA superficial to FV and then passed deep to FA and then deep between the Pectineus and Adductor longus. In this case MCFA arose from PFA and LCFA from FA.
In 4 limbs (6.06 %) superficial branches arose from PFA.
In one cadaver bilateral origin of superficial circumflex iliac branch from PFA was seen and rest two superficial branches took origin from FA.
In high origin of PFA limb with anterolateral site of origin showed all superficial branches arose from PFA [Table/Fig-4].
Shows level of origin of PFA from midpoint of inguinal ligament
| Distance In mm | Sides | Total in mm | Remark | Bilateral representation |
|---|
| Right (mm) | Left (mm) |
|---|
| 0-10 | 7 | 7 | 14 | High origin | 3 cadavers |
| 11-20 | 4 | 7 | T 18 | 39 | Commonest range of origin | 11 cadavers (+ 5 mm) |
| 21-30 | 8 | T 17 | 5 |
| 31-40 | 9 | 6 |
| 41-50 | 3 | 3 | 13 | Low origin | 3 cadavers |
| 51-60 | 2 | 4 |
| 61-70 | 0 | 1 |
| Total | 33 | 33 | 66 | -------- | 51.51% |
Regarding high origin of PFA
| Origin distance | No. of cases | Percentage (%) | Sides | Site of origin | Size of PFA in comparison with FA | Origin of superficial branches of thigh |
|---|
| Rt | Lt | Lat | Med | AL | PL | Normal | Half | Equal | Rt | Lt |
|---|
| Inferior to Ing. Lig | 7 | 10.60 | 4 | 3 | 4 | -- | 1 | 2 | 4 | --- | 3 | 1 | 2 |
| 5-10 mm | 7 | 10.60 | 3 | 4 | 4 | 1* | -- | 2 | 4 | 1* | 2 | -- | --- |
| Total | 14 | 21.20 | 7 + 7 = 14 | 8 + 1 + 1 + 4= 14 | 8 + 1 + 5 = 14 | 3 |
*same limb [Table/Fig-3] Lat – lateral, med – medial, AL- anterolateral and PL – posterolateral
Discussion
PFA shows variations in terms of point of origin, course and branches. These variations have received attention of surgeons, radiologists, cardiologists and anatomists [8].
Variations may not endanger the life of patients and they are usually subclinical, but knowledge of variation in the origin of PFA and its branches is of great significance for preventing flap necrosis, particularly tensor fascia latae, when used in plastic and reconstructive surgery and also important for the vascular surgeons and interventional radiologists [5,9]. This knowledge is also essential in the surgical repair of femoral hernias, in vascular reconstructive procedures in the proximal leg. Plastic surgeons use the muscular branches while incorporating myocutaneous flaps. This vessel is useful for the Doppler imaging ultrasonography, arteriography and angiography and MRI [6,7].
The knowledge of the site of origin of PFA is important while performing clinical procedures in the femoral region and in hip joint replacement and also for avoiding iatrogenic arterio venous fistula or severe secondary haemorrhage while performing femoral artery puncture [10]. The different anatomical relationships and lack of knowledge of variations of these vessels make the haemostasis difficult to manage [4].
In developmental process, some of the channels regress and some of them enlarge and form a definitive arterial pattern. The persistence of the channel that was supposed to disappear lead to various anomalies [9].
The normal distance of origin of PFA from the midpoint of inguinal ligament is about 30-40 mm. In present study this distance was between 21-40 mm on right side and 11-40 mm on left side. This distance is 31-40 mm on right side and 41-50 mm on left side [11] while it is between 21-40 mm [4].
The most common site of origin of PFA is posterolateral aspect of FA, in present study we found in 53.03 % cases PFA originated from posterolateral aspect of FA. But few authors consider posterolateral and lateral side origin is the most common pattern. It was found that almost 71.21% cases PFA originated on Posterolateral and Lateral aspect of FA. Lateral side origin is more common than posterolateral aspect [8]. In 24.24% of cases PFA originated on posteromedial and posterior aspect of FA and this was less than study by Dixit et al., (31.25%).
In two limbs (3.03%) medial side origin of PFA and it runs superficial to FV, as per various literature such variation is rare. It carries a risk of damage to the large and unexpected arterial channel while collecting blood in infants from FV and during exposure of saphanous veins for ligation its junction with the FV [11]. In one limb anterolateral origin of PFA from FA such origin has not been noticed earlier in any literature. This PFA originated just deep to inguinal ligament from lateral side of FA and superficial branches arose from PFA instead of FA. This anterolateral origin and superficial branches from PFA is unique and new in medical science. In 4 limbs (6.06 %) we noted superficial branches from PFA. Chances of superficial branches from FA are 83.3%, from deep circumflex artery in 6.6%, from LCFA in 6.6 % and from PFA in 3.3 % [12]. Our findings are more than the literatures records.
In 13 limbs (19.69%), we noted that PFA originated from FA as a common stump either with MCFA (in 6 limbs) or LCFA (in 7 limbs). Hence incidence of origin of PFA with any one of the circumflex artery is same. As per study done by Uzel et al., the origin of PFA with LCFA as a common trunk is seen in 0.9 % [13] While MCFA originated as a common stem with PFA is 2.5% [14]. But as per present study it was 10.60 % and 9.09 % respectively which is quite high than their study.
In three limbs (4.54%) we found PFA and two circumflex arteries (MCFA and LCFA) originated from FA as a common stump with typical course. Such trifurcation was seen either in very low origin of PFA (46 mm) or in a high origin (10 mm). PK Atulya et al., noted 0.9 % cases, as per study done by Uzel et al., Our findings are quite high.
In 14 limbs, we found PFA originated at a higher level (distance between 0-10mm). Advantage of such a high origin is that it can be used for catheterization and further investigation of any arterial system. Sabnis noted in 1.6 % cases origin is just below the inguinal ligament and in 3.01% cases it was originating half inch below the inguinal ligament. High origin of PFA is always a threat to procedures like femoral vessel puncture and nerve block. The injury caused by percutaneous FA cannulation can cause pseudo-aneurysm. This usually happens when the puncture site is PFA or FA distal to origin of PFA [6]. In present study incidence of high origin is very high (21.21 %). According to present study bilateral high origin of PFA is seen in 3 cadavers (6 limbs) while unilateral high origin seen in rest 8 limbs (4 left sided and 4 right sided limbs). Hence incidence of high origin is same on both the sides but more common in females. But as per various literatures left side is rare for high origin. Incidence of high origin was 10% [4]. Interventional radiology in cardiac patients’ femoral arteriography is the main line for investigation in peripheral occlusive arterial disease and in diagnosis of suspected congenital anomalies. In such cases origin of PFA and its branches in front of thigh are of clinical significant [4]. This high origin of PFA can become matter of concern to orthopaedic surgeons, radiologists, plastic surgeons and general surgeons any of whom may perform surgical procedures in this area [10].
Conclusion
According to present study the most common site of origin of PFA was from posterolateral and lateral side of FA. A very rare variation was also observed that PFA arising from medial side of FA with superficial course on FV. We also noted high origin of PFA from anterolateral site of FA and all the superficial branches of thigh took origin from PFA. Such finding is also very rare. Finally we found very high incidence of high origin of PFA. All these information is very important for the surgeons working in this locality.
[1]. Mamatha H, Antony Sylvan D’souza, Jessica S, Suhani S, A cadaveric study on the variations in the origin, course and branching pattern of the profunda femoris arteryInternational Journal of Current Research and Review 2012 4(19):137-45. [Google Scholar]
[2]. Standring S, Gray’s anatomy. The Anatomical Basis of the Clinical Practice 2008 40th editionSpainChurchill Livingstone Elsevier:1379-80. [Google Scholar]
[3]. Hollinshead HW, Textbook of Anatomy 1974 3rd EdHagerstown, MarylandHarper & Row:407 [Google Scholar]
[4]. Baptist M, Sultana F, Hussain T, The origin of profunda femoris artery, its branches and diameter of the femoral arteryProfessional Med J 2007 14:523-27. [Google Scholar]
[5]. Prakash KJ, Kumar BA, Jose BA, Yadav Kumar S, Singh G, Variations in the origins of the profunda femoris and the medial and the lateral femoral circumflex arteries: a cadaver study in the Indian populationRom J Morphol Embryol 2010 51(1):167-70. [Google Scholar]
[6]. Phalgunan V, Srinivasan B, Variation of lateral circumflex femoral artery and profunda femoris artery:a case reportInternational journal of anatomical variations 2013 6:213-15. [Google Scholar]
[7]. Chitra R, A rare variational anatomy of the profunda femoris arteryFolia Morphol (Warsz) 2008 67(2):157-58. [Google Scholar]
[8]. Sabnis AS, Anatomical variations of profunda femoris arteryJournal of clinical research letters 2013 4(1):54-56. [Google Scholar]
[9]. Shetty AS, Shetty S, Rakesh G, Narendra P, Raghu J, An atypical outsized lateral circumflex femoral artery and its clinical implicationsJCDR 2012 6(7):1284-45. [Google Scholar]
[10]. Dimri P, Deshwal AK, Bilateral high origin of profunda femoris artery-case report and embreological reviewInternational journal of scientific research 2014 3(1):375-76. [Google Scholar]
[11]. Daksha Dixit, Kubavat Dharati M, Rathod Suresh Bhai P, Patel Mittal M, Singel Tulsi Bhai C, A study of variation in origin of profundafemoris artery and its circumflex branchesInt J Biol Med Res 2011 2(4):1084-89. [Google Scholar]
[12]. Mergu P, Prasad VS, Unique variation in origin and branching pattern of profundafemoris artery: a case reportOA Anatomy 2014 2((1)5):1-3. [Google Scholar]
[13]. Atulya PK, Variation in origin and branching pattern of lateral circumflex femoral artery: a rare case reportInternational Journal of Health and Rehabilitation science 2013 2(1):72-75. [Google Scholar]
[14]. Lalović N, Mališ M, Korica M, Cvijanović R, Simatović M, Ilić5 M, Origin of the medial circumflex artery – A cadaveric studyMedicinski Glasnik 2013 10(2):198-202. [Google Scholar]