Splenic Injury in Situs Inversus Totalis – A Surgical Challenge
Bharat Kamath1, Ambarish S Chatterjee2, ITI Chandorkar3
1 Assistant Professor, Department of Surgery, Seth V.C. Gandhi & M.A. Vora Municipal General Hospital, Rajawadi, Ghatkopar (E), Mumbai, India.
2 Registrar, Department of Surgery, Seth V.C. Gandhi & M.A. Vora Municipal General Hospital, Rajawadi, Ghatkopar (E), Mumbai, India.
3 Registrar, Department of Surgery, Seth V.C. Gandhi & M.A. Vora Municipal General Hospital, Rajawadi, Ghatkopar (E), Mumbai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ambarish S Chatterjee, H-223 & 224, 7th Floor, Mulund Darshan, Mulund Colony, Mulund (west), Mumbai-400082, Maharashtra, India. E-mail : ambarish_5@yahoo.com
Situs inversus totalis is a rare congenital anomaly in which position of the heart and all abdominal viscera is reversed. Situs abnormalities usually go unnoticed but may be recognized by radiography or ultrasonography as an incidental finding or during evaluation for congenital heart diseases. We present such an extremely rare and to the best of our knowledge the third reported case of an injured spleen in the right hypochondrium, following seemingly trivial blunt trauma in a patient with situs inversus totalis who underwent splenectomy. The presence of associated congenital heart defects, visceral anatomical variations and mirror imaging makes the anaesthetic management as well as the surgical exercise a challenging one in such cases.
Blunt abdominal trauma, Congenital anomaly, Splenectomy
Case Report
A 24-year-old female patient came to the surgical outpatient department with history of pain in her right upper quadrant of abdomen which was referred to the right shoulder. On further elucidating the history she revealed a trivial blunt trauma to her abdomen four days earlier, as she slipped and got hit by the kitchen table. On examination the patient was hemodynamically stable. Her abdomen was soft, not distended with mild tenderness in the right hypochondrium. There was no evidence of thoracic or abdominal wall injury. Suspecting a soft tissue contusion she was given intramuscular analgesic, but the symptom of referred pain to right shoulder was suggestive of an intra-abdominal pathology and warranted further investigations.
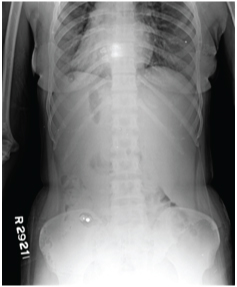
An erect chest and abdominal X-ray as well as an ultrasound abdomen-pelvis were done. It revealed situs inversus totalis with cardiac apex to the right, mild hemoperitoneum, with suspected splenic laceration [Table/Fig-1&2]. The hemogram showed haemoglobin 8.1gm%, total count 5000 cells/mm3 and platelets 1.85 lac. Baseline ECG and 2D Echocardiography was done which ruled out any congenital heart defects and conduction abnormalities.
X-ray Chest PA view showing cardia apex to the right (dextrocardia)

X-ray Abdomen Erect PA view with no significant findings except dextrocardia
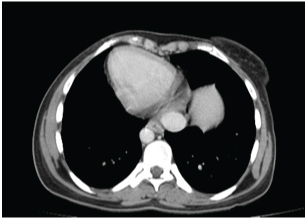
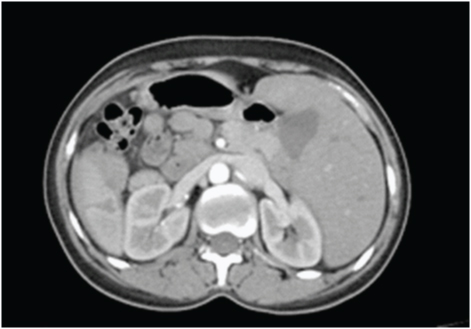
Contrast Enhanced Computed Tomography (CECT) of the abdomen was suggestive of situs inversus totalis with dextrocardia [Table/Fig-3]. It depicted the spleen in right hypochondrium showing laceration at lower pole measuring 2.2cm in transverse diameter extending across medial to lateral border and a 4.6 x 3.4 x 4.8 cm hematoma at the lower pole [Table/Fig-4]. A 14 x 9 mm size area of contrast blush was noted in lower pole, superior to laceration site on arterial phase which appeared isodense in venous and delayed phase suggesting pseudoaneurysm rather than active arterial extravasation. Splenic vessels were unremarkable. Mild to moderate hemoperitoneum was noted in abdomen and pelvis.
CECT scan showing the cardiac apex to the right (dextrocardia)
CECT Abdomen showing laceration of spleen present in the right hypochondrium with hematoma
Since the patient was vitally stable with no evidence of peritonitis and abdominal distension, conservative management was started with strict bed rest, intravenous fluids, blood transfusions, strict monitoring of input-output and abdominal girth. On the second day she developed hypotension and rapid increase in abdominal girth. Emergency explorative laparotomy revealed 1000ml hemoperitoneum, the injured spleen in the right hypochondrium with a 3 x 2 x 1 cm laceration in the lower pole, 2 x 1 x 1 cm laceration in the hilar region not involving the splenic pedicle [Table/Fig-5]. All other abdominal organs were normal except for the obvious situs inversus. Splenectomy was done with due consideration of the mirrored positions of the intra abdominal organs. Prophylactic appendicectomy was also done which was present in the left iliac fossa. Postoperative period was uneventful and the patient was immunized with pneumococcal, meningococcal and H influenza vaccines. The patient was discharged 10 days later and is being followed up for the past 6 months.
Intra-operative image showing the injured spleen with hematoma in the right hypochondrium

Discussion
Situs inversus totalis is a rare congenital anomaly, prevalence of which is 1 in 10,000 individuals [1]. In situs inversus totalis, the heart and abdominal organs are mirror image of the normal anatomy called as situs solitus. It is an autosomal recessive disease, at times X-linked [2]. The incidence of congenital heart disease is higher in patients of situs inversus with levocardia (90%) [2]. There is a 5-10% prevalence of congenital heart disease in patients with situs inversus totalis, most commonly being transposition of great vessels [3]. A patient of situs inversus may lead a normal life without being diagnosed in his or her lifetime. It is usually diagnosed incidentally when patient is evaluated for some other complaint or when there is an associated congenital heart disease. Situs inversus totalis may be associated with primary ciliary dyskinesia, known as Kartagener syndrome [4]. Surgical management in situs inversus totalis is difficult because of the altered anatomy. Anaesthetic complications may arise in these patients because of the high incidence of congenital heart diseases. A situs inversus patient undergoing splenectomy as a result of traumatic splenic injury is exceedingly rare and very few cases are reported in literature [3,5–8]. Srivastva V et al., [5] and Rohan Khandelwal et al., [6] described cases with situs inversus undergoing splenectomy for splenic injury following blunt abdominal trauma. Ribas-Filho JM et al., [7] reported case of situs inversus undergoing splenectomy after a penetrating abdominal trauma, in which there were co-existing injuries to stomach, pancreas and the diaphragm. To the best of our knowledge, this is the third reported case of splenectomy for splenic injury following blunt abdominal trauma in a patient with situs inversus totalis.
Though no difficulties were encountered during emergency splenectomy in this case, anatomical variations have to be considered. The fact that our patient presented in the outpatient department with history of trivial trauma four days earlier, could have mislead any health-care professional. The injured organ being the spleen in the right hypochondrium, initially misleading the surgeon, and the varied orientation of the viscera and anatomical aberrations makes such cases exceptional.
Conclusion
To conclude, a high index of suspicion should be maintained in any case of seemingly trivial abdominal trauma with signs of peritoneal or diaphragmatic irritation, even if the patient is initially hemodynamically stable with due consideration for altered visceral anatomy.
[1]. Splitt MP, Burn J, Goodship J, Defects in determination of left-right asymmetryJ Med Genet 1996 33:498-503. [Google Scholar]
[2]. Casey B, Genetics of human situs abnormalitiesAm J Med Genet 2001 101(4):356-58. [Google Scholar]
[3]. Francisco RC, Zulu Casanova M, Patient with situs inversus stabbed in the right flankThe Internet Journal of Surgery 2009 20(1):24 [Google Scholar]
[4]. Holzmann D, Ott PM, Felix H, Diagnostic approach to primary ciliary dyskinesia: a reviewEur J Pediatr 2000 159:95-98. [Google Scholar]
[5]. Srivastva V, Kumar P, Dosar S, A case of splenic rupture in patient of situs inversusIndian J Surg 2010 72(1):326-27. [Google Scholar]
[6]. Khandelwal R, Chaudhary R, Kumar L, Singh M, Usurumarthi P, Singh S, Splenic rupture in a patient with situs inversusJRSM 2012 3(9):61 [Google Scholar]
[7]. Ribas-Filho JM, Maluf-Junior I, Ribas FM, Czeczko LEA, Kuradomi IY, Badia EA, Firearm Injury Patients with Situs InversusTotalis - Case ReportArq Bras Cir Dig 2011 24(3):249-50. [Google Scholar]
[8]. Suthar T, Banker H, Shah M, Thakkar G, Splenic infarct with polysplenia syndrome and situsinversusBMJ 2012 doi: 10.1136/bcr.02.2012.5831 [Google Scholar]