Anaesthesia for a Rare Case of Down’s Syndrome with Morgagni’s Hernia Undergoing Laparoscopic Repair
Nethra H Nanjundaswamy1, Vinay Marulasiddappa2
1Assistant Professor, Department of Anaesthesia, Bangalore Medical College and Research Institute, Bengaluru, India.
2Associate Professor, Department of Anaesthesia, Bangalore Medical College and Research Institute, Bengaluru, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nethra H Nanjundaswamy, Assistant Professor, Department of Anaesthesia, Bangalore Medical College and Research Institute, Fort, KR Road, Bengaluru-560002, India.
E-mail: drnethrahn@gmail.com
Morgagni’s hernia is a type of congenital diaphragmatic hernia and it is rare in children. The association between Down’s syndrome and Morgagni’s hernia in children is also rare. Laparoscopic repair is a preferred surgical approach than open surgical procedures as laparoscopy offers a bilateral view of Morgagni’s hernia, minimal tissue damage and a faster recovery. When children with Down’s syndrome and associated Morgagni’s hernia present for laparoscopic repair, they pose several complex challenges to the anaesthetist due to the involvement of multiple organ systems, difficulties in airway management and effects of laparoscopic surgery on the organ systems. Therefore, such children need a very careful anaesthetic plan, including a thorough preoperative assessment and preparation for a successful perioperative outcome.
Congenital, Diaphragmatic, Hernias, Hernioplasty, Retrosternal-hernia, Trisomy 21
Case Report
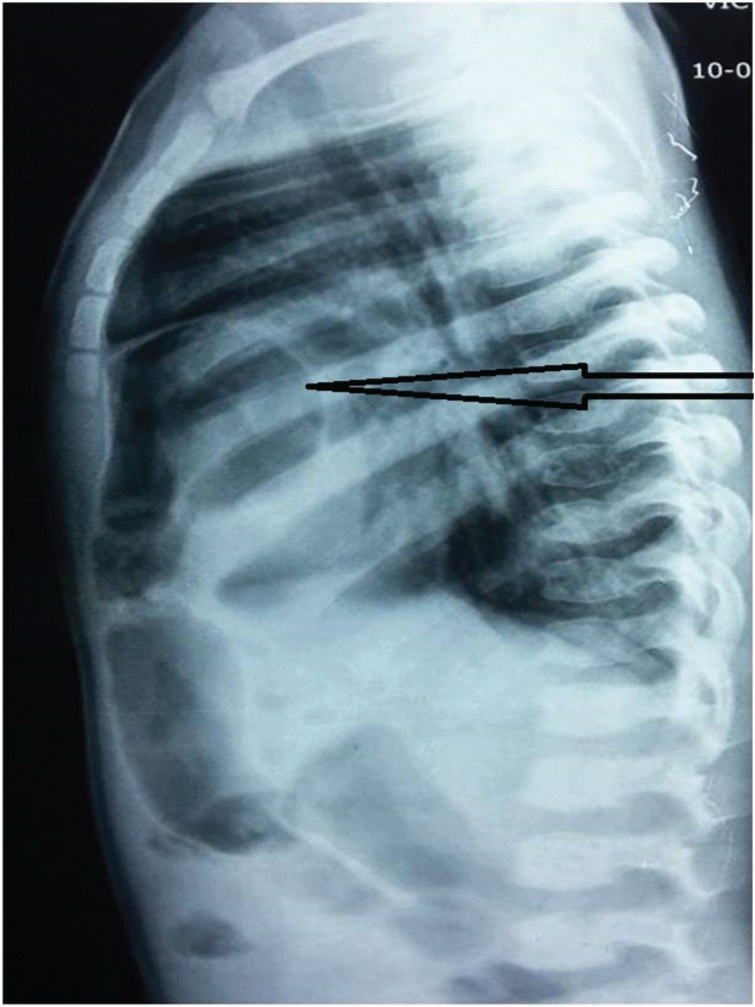
A 2-year-old male child was admitted to Paediatric Superspeciality hospital with symptoms of lower respiratory tract infection. He presented with history of recurrent respiratory distress and cough. Radiological reports revealed haziness in the mid-zone of the right lung and incidental finding of bowel loops in retrosternal area. He was treated for lower respiratory tract infection and subsequently referred to paediatric surgery. Chest X-ray showed herniation of bowel loops into the chest, suggesting congenital diaphragmatic hernia [Table/Fig-1]. Computerized tomography (CT) scan showed Morgagni type of congenital diaphragmatic hernia. Child was posted for laparoscopic hernia repair. Pre-anaesthetic evaluation was done. Child was the third issue of a non consanguineous couple. He had history of recurrent respiratory problems, delayed milestones of development and growth retardation. Child weighed eight Kg. Physical examination findings were - up slanting lateral canthus, large tongue and single palmar crease. Airway assessment revealed normal neck movements and adequate mouth opening. Systemic examination revealed occasional bilateral crepitations. Other systems were normal. Echocardiography, karyotyping and haemogram were advised. Haemogram was normal with haemoglobin content of 12gms/dl. Serum electrolytes and renal parameters were also normal. Karyotyping confirmed Trisomy 21. Cervical spine X-ray was normal.
After the treatment of infection with antibiotics and chest optimization, child was posted for laparoscopic repair of congenital diaphragmatic hernia. Written informed consent was taken from parents. Child was kept fasted for six hours. Intravenous (IV) fluids were started at 6 AM. Premedication was given in the form of Inj. Glycopyrrolate 0.04mcg/kg, Inj. Ondansetron 0.08mcg/kg IV. Inj. Ranitidine 1mg/kg was administered as aspiration prophylaxis one hour prior.
Patient was shifted to operation theatre. Pre-induction monitors such as electrocardiogram (ECG), pulse oximetry, end tidal carbon-di-oxide (EtCO2) were placed. After preoxygenation for three minutes, child was induced with intravenous thiopentone sodium 5mg/kg and fentanyl 2mcg/kg. Muscle relaxation was achieved with injection atracurium 0.5mg/kg. Intubated with endotracheal (ETT) tube of size 4.5. Bilateral air entry was checked and ETT fixed. Laparoscopy was started with head elevated position. Anaesthesia was maintained with oxygen and air with sevoflurane along with intermittent doses of atracurium. Ventilation was with pressure control mode with PEEP during pneumoperitonium. Minute ventilation was frequently altered by modifying tidal volume and respiratory rate to maintain ETCO2 between 35-40 mm/hg.
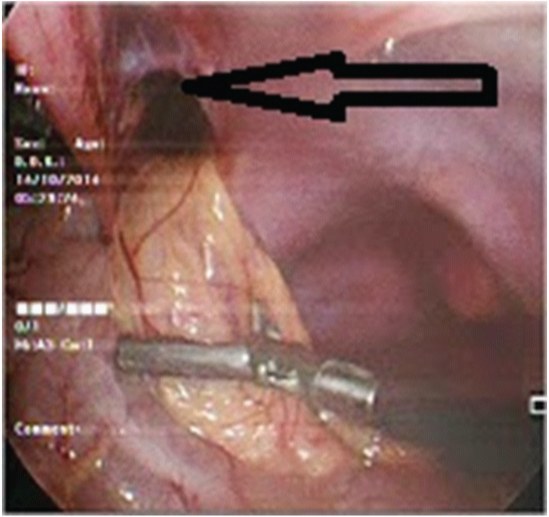
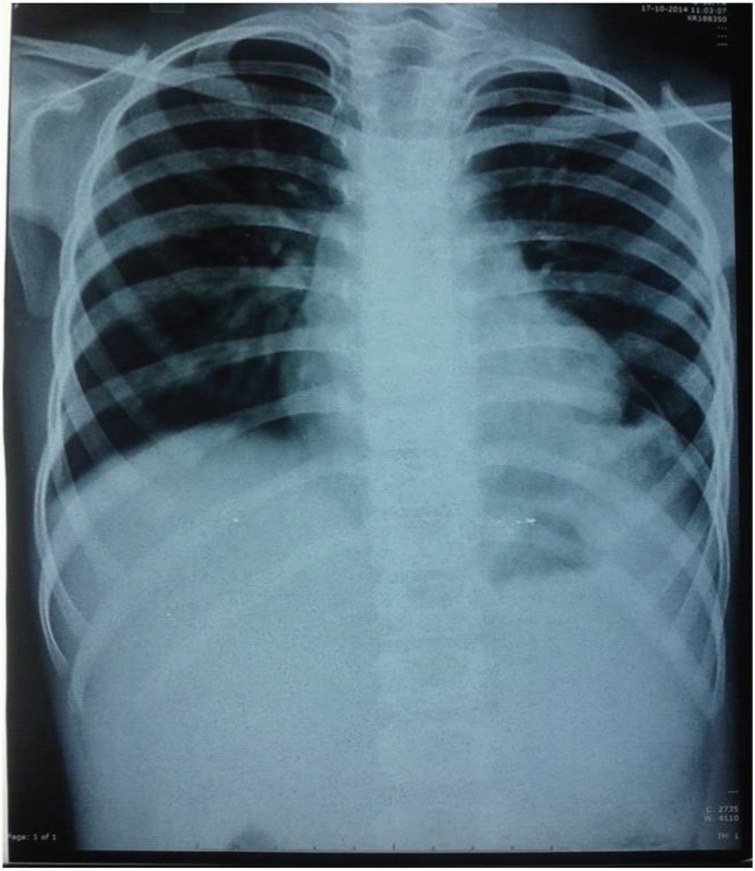
Laparoscopy revealed Morgagni’s hernia containing loops of intestine [Table/Fig-2]. The contents of the hernia were reduced and the anchoring sutures were placed by laparoscopic assisted technique to occlude the hernia defect. Child was haemodynamically stable throughout the surgery. At the end of surgery, patient was extubated fully awake in the operating room. He was shifted to Paediatric ICU for observation for 24 hours. His postoperative x-ray chest was done on 5th postoperative day and was normal [Table/Fig-3]. His postoperative recovery was excellent, and he was discharged on the 5th postoperative day.
Discussion
Down’s syndrome is a congenital anomaly occurring due to extra chromosome attached to Chromosome 21. This is also called as Trisomy 21 [1]. Trisomy 21 is the commonest chromosomal abnormality that affects people with an incidence of 1:800 live births [1]. Congenital diaphragmatic hernia is the herniation of abdominal contents through the patent pleuroperitoneal canals in the diaphragm. Commonest type is posterior-lateral hernia (Bochdalek hernia) and rarest is retrosternal hernia (Morgagni’s hernia). Morgagnian hernia is rare and contributes to 1-6% of congenital diaphragmatic hernias [2,3].
Down’s syndrome is associated with anomalies in various systems. Cardiovascular, respiratory and central nervous system may be involved in Down’s syndrome as an isolated system involvement or multiple system involvement, thus posing several anaesthetic challenges. Clinical features of Down’s syndrome include microcephaly, macroglossia, and ligamentous laxity at atlanto occipital joint and subglottic stenosis, which can pose problems for securing airway [1]. Atlantoaxial instability has been reported in 20% of patients and spinal cord compression in 2% [4]. Hence, it is important to do a cervical spine X-ray preoperatively. In our case, it was normal. Down’s syndrome is associated with several types of congenital heart defects such as endocardial cushion defects (40%), ventricular septal defects, atrial septal defects (30-60%), patent ductus arteriosus (12%) and Tetrology of fallot (8%) [5].
Therefore, it is important that echocardiography should be performed in these cases. Echocardiography was normal in our case. Gastrointestinal anomalies associated are duodenal stenosis, gastro esophageal reflux, imperforate anus and Hirschsprung's disease [6]. Therefore, premedication should include prophylaxis to prevent gastro esophageal reflux. Congenital diaphragmatic hernia is the herniation of abdominal contents through unfused pleuroperitoneal canals in the diaphragm. Commonest type is posterior-lateral (Bochdalek) hernia. Morgagnian hernia is herniation through retrosternal space also known as foramen of Morgagni. Morgagni’s hernia is rare in the paediatric age group accounting for approximately 5% of all types of congenital diaphragmatic hernia and is usually asymptomatic, discovered accidentally or by production of vague gastrointestinal or respiratory symptoms [7]. Only few cases of Morgagni’s type of congenital diaphragmatic hernia are associated with Down’s syndrome [3].
Morgagnian hernia has also been noted in identical twins with Down’s syndrome. This indicates the possibility that it may be an inherited defect. This is supported by the frequent association of Morgagni’s hernia with other congenital defects such as Down’s syndrome [7]. Morgagnian hernia presents with vague symptoms like pain abdomen, repeated chest infections or detected incidentally in imaging studies performed for chest symptoms [7]. Our patient too presented with repeated chest infections and initially diagnosed with congenital diaphragmatic hernia (CDH) on chest X-ray and subsequently CT scan confirmed Morgagnian type of CDH.
The age of presentation is from neonatal age group to 12 years of age. Sometimes Morgagnian hernias are detected when patients present with intestinal obstruction or trauma. Diagnosis is confirmed by chest x-ray, barium study and CT scan of chest and abdomen. Once detected, treatment is reducing the contents and surgical closure of the defect. Morgagni’s hernia may be repaired through transabdominal or transthoracic approach. However, minimally invasive procedure such as laparoscopy offers greater benefits of better bilateral view of hernia, less tissue trauma and rapid recovery for the patient. Hence, laparoscopic repair is the gold standard technique for hernia repair [8].
Laparoscopic surgeries in children pose several challenges to the anaesthetist. The increase in Intra Abdominal Pressure (IAP) affects respiratory function. In infants the increase in the intraabdominal pressure due to pneumoperitonium causes alveolar collapse thus significantly reducing the functional residual capacity and increase in venous admixture leading to faster desaturation than in adults [4]. The challenges faced by the anaesthetist in such case would be that of Down’s syndrome with its associated airway problems like atlanto-axial instability, susceptibility to respiratory tract infections, pulmonary hypoplasia, gastro-esophageal reflux and sensitivity to anaesthetic agents. These challenges would be further complicated by the associated Morgagnian hernia and the challenges associated with laparoscopic surgeries in children.
Lateral view of the Chest X-ray showing herniation of bowel loops into the chest, suggestive of congenital diaphragmatic hernia
Intraoperative laparoscopic view showing the foramen of Morgagni with herniation of abdominal contents into the chest
Posterio-anterior view of the postoperative chest X-ray showing complete resolution of the Morgagni’s hernia
Conclusion
The association between Down’s syndrome and Morgagnian hernia in children is rare and such children pose several challenges to the anaesthetist, especially when they undergo laparoscopic surgery. In our case, a detailed preoperative assessment and optimization was done. There was no atlanto-axial instability and cardiovascular anomalies. However, child was evaluated thoroughly and anaesthetic management was planned with anticipation for difficult airway, sensitivity to drugs and ventilation challenges in laparoscopy. A meticulous anaesthetic management resulted in a good perioperative outcome in our case.
[1]. JV Kale, Anaesthetic management in Congenital Diaphragmatic Hernia with Down’s syndrome -A case reportIndian Journal of Applied Research 2013 3(8):596-97. [Google Scholar]
[2]. A Al-Salem, Congenital hernia of Morgagni in childrenAnn Saudi Med 1998 18(3):260-62. [Google Scholar]
[3]. MH Beg, ME Rashidi, V Jain, Morgagni hernia with Down’s syndrome: A rare associationIndian J Chest Dis Allied Sci 2010 52:115-17. [Google Scholar]
[4]. S Singh, R Verma, A Pandey, C Tandon, A Wakhlu, A Agarwal, Laparoscopic surgery in a paediatric patient with Down’s syndrome and patent foramen ovaleBMJ Case Reports 2011 2011:1-2. [Google Scholar]
[5]. GL Wells, SE Barker, SC Finley, EV Colvin, WH Finley, Congenital heart disease in infants with Down's syndromeSouth Med J 1994 87(7):724-27. [Google Scholar]
[6]. PJ Buchin, JS Levy, JN Schullinger, Down's syndrome and the gastrointestinal tractJ Clin Gastroenterol 1986 8(2):111-14. [Google Scholar]
[7]. A Al-Salem, HA Khawahery, Delayed presentation of bilateral Morgagni’s hernia in a child with Down’s syndromeSaudi Med J 2002 23(2):237-39. [Google Scholar]
[8]. GH Godazandeh, M Mortazian, Laparoscopic Repair of Morgagni Hernia using Polyvinylidene Fluoride (PVDF)MeshMiddle East J Dig Dis 2012 4:232-35. [Google Scholar]