Seroepidemiological Survey of Chikungunya in and Around the Regions of Bijapur (Vijayapura - North Karnataka)
Bharath Mudurangaplar1, Basavaraj V. Peerapur2
1 PhD Scholar, Department of Microbiology, Shri B M Patil Medical College and Research Center, BLDE University, Bijapur, Karnataka, India.
2 Professor, Department of Microbiology, Raichur Institute of Medical Sciences, Raichur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Mr. Bharath Mudurangaplar, PhD Scholar, Department of Microbiology, Shri B M Patil Medical College and Research Center, BLDE University, Bijapur. Karnataka, India.
E-mail: Bharathmd12@gmail.com
Background
Chikungunya is a debilitating, non-fatal, mosquito borne viral fever caused by Chikungunya virus (CHIVA). The disease is transmitted to humans by the bite of Aedes aegypti and Aedes albopictus mosquitoes. Severe outbreaks of Chikungunya have been reported in several countries of Africa and Asia. Chikungunya fever is characterized by fever with sudden onset, arthralgia, rash, headache and myalgia. However, arthralgia is painful and long-lasting, affecting primarily the peripheral joints.
Objectives
To find out the prevalence of Chikungunya fever in and around the regions of Bijapur district.
Materials and Methods
The study was conducted from April 2011 to December 2014. Five hundred serum samples were collected from cases with pyrexia and arthralgia. Serum samples were tested for Chikungunya antibodies by Chikungunya IgM ELISA.
Results and Conclusion
Out of 500 samples 33 samples were confirmed positive for Chikungunya IgM antibodies. The prevalence rate of Chikungunya was 6.6% with maximum number of cases in the year 2013 (8.5%) and age group 15 to 40 (8.3%). Females (6.9%) were more affected than males. Thus, continuous sero-epidomological surveillance is needed for the control of Chikungunya fever.
Arboviral, IgM ELISA, Viral fever
Introduction
Chikungunya is a “debilitating non-fatal viral fever”. ‘Swahili’ is a language spoken in East Africa. The meaning of Chikungunya in Swahili language is ‘that which bends up’ in reference to the stooped posture developed as a result of the arthritic symptoms of the disease. The disease was first documented in 1952, following an outbreak on the Makonde Plateau, along the border between Tanganyika (Tanzina) and Mozambique [1]. Chikungunya fever is an arboviral disease caused by Chikungunya virus (CHIVA). It is a member of family Togaviridae and genus alphavirus. It is an enveloped ribonucleic acid virus. RNA is single-stranded, linear, positive-sense of approximately 11.8 kb [2].
The disease is transmitted to humans by the bite of the female Aedes aegypti and Aedes albopictus mosquitoes. Chikungunya fever has been originally distributed in several parts of Africa, South Asia and Southeast Asia. In India, well-documented outbreaks occurred in 1963 and 1964 in Kolkata and southern India respectively. A small outbreak of Chikungunya (CHIK) was Reported from Solapur district, Maharashtra in 1973. The virus disappeared for three decades and re-emerged in French island of Reunion in the Indian Ocean in 2005. In 2006, a large outbreak occured in India Andhra Pradesh, Andaman & Nicobar Islands, Tamil Nadu, Karnataka, Maharashtra, Gujarat, Madhya Pradesh, Kerala and Delhi were badly affected. An outbreak of Chikungunya was reported from Italy in 2007 and Thailand and south India in 2009 [3–7]. Recently in 2014, Chikungunya reached United States and cases have been reported from Florida by Centers for Disease Control and Prevention [8].
The Chikungunya fever presents with triad of symptoms fever, arthralgia and rashes. A very important feature of Chikungunya fever is a debilitating and prolonged arthralgia that primarily affects the peripheral small joints. While the acute febrile phase of the illness normally resolves within a few days, the pain associated with CHIKV infection of the joints typically persists for weeks to months or years together in chronic cases [9,10].
In the present study clinically suspected cases were tested by ELISA for Chikungunya IgM antibodies. Disease in general, serological diagnosis and the prevalence of Chikungunya in and around Bijapur has been described. Recently in 2014 Bijapur name has been changed to Vijayapura by Government of India.
Materials and Methods
The study was conducted from April 2011 to December 2014. A total of 500 blood samples from suspected Chikungunya cases were included in the study. Blood samples from clinically suspected Chikungunya patients, i.e. pyrexia of more than >38.50C and polyarthralgia were collected from BLDE’s hospital, Bijapur and Government PHC, CHC, taluk and district hospitals of Bijapur district. Informed consent was obtained from all the patients prior to sample collection. Two to five ml of venous blood was collected aseptically. The samples were transported to the laboratory in a vaccine carrier. Serum was separated by centrifugation and labelled with patient identification number and stored at -70°C. Serum samples were tested for Chikungunya IgM antibody with SD (standard diagnostics) Chikungunya IgM ELISA kits. Direct Enzyme linked immune sorbent assay (ELISA) was performed. The tests were performed strictly as per the manufacturers’ instructions. The data thus obtained was presented by using frequencies and percentages.
Results
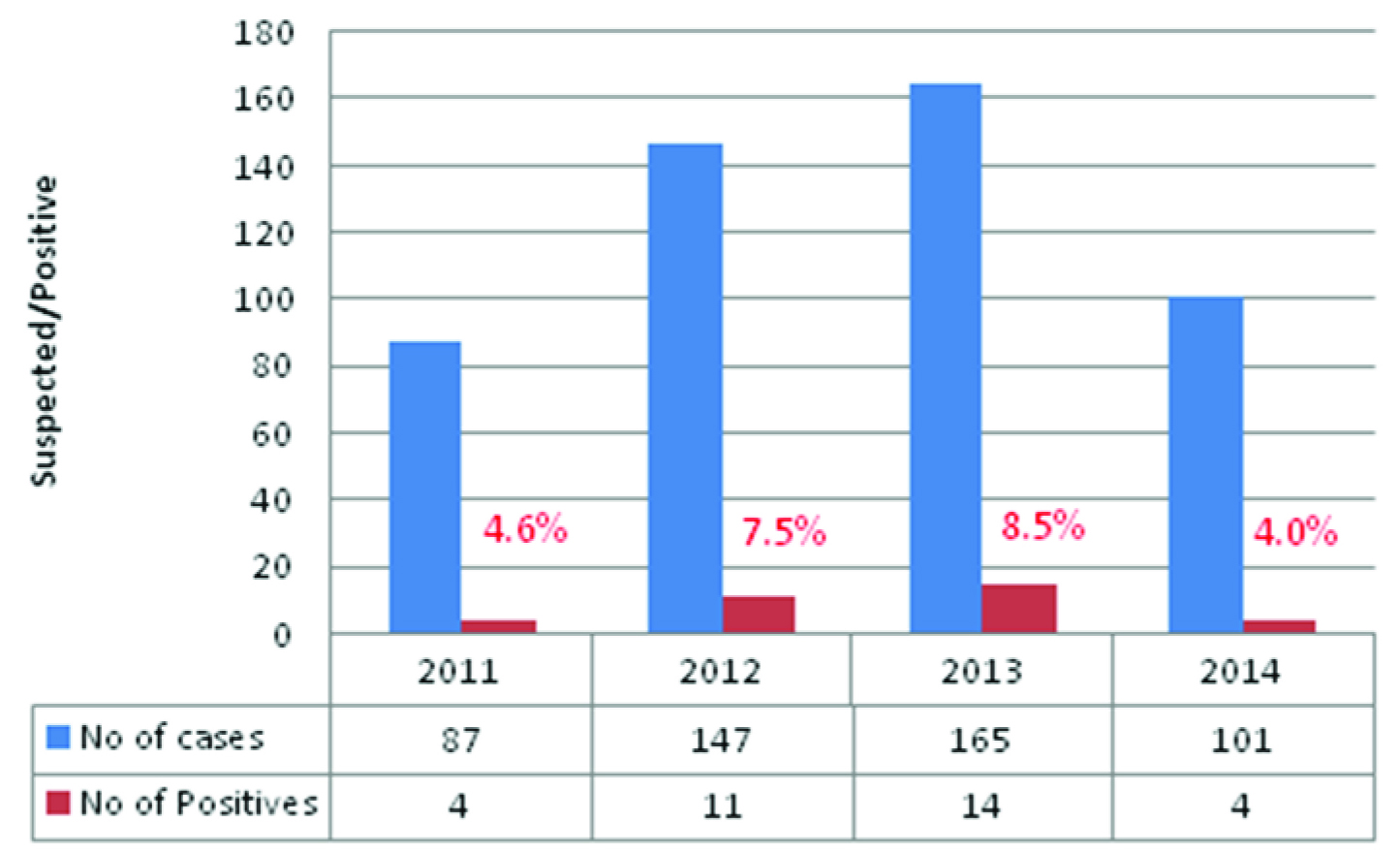
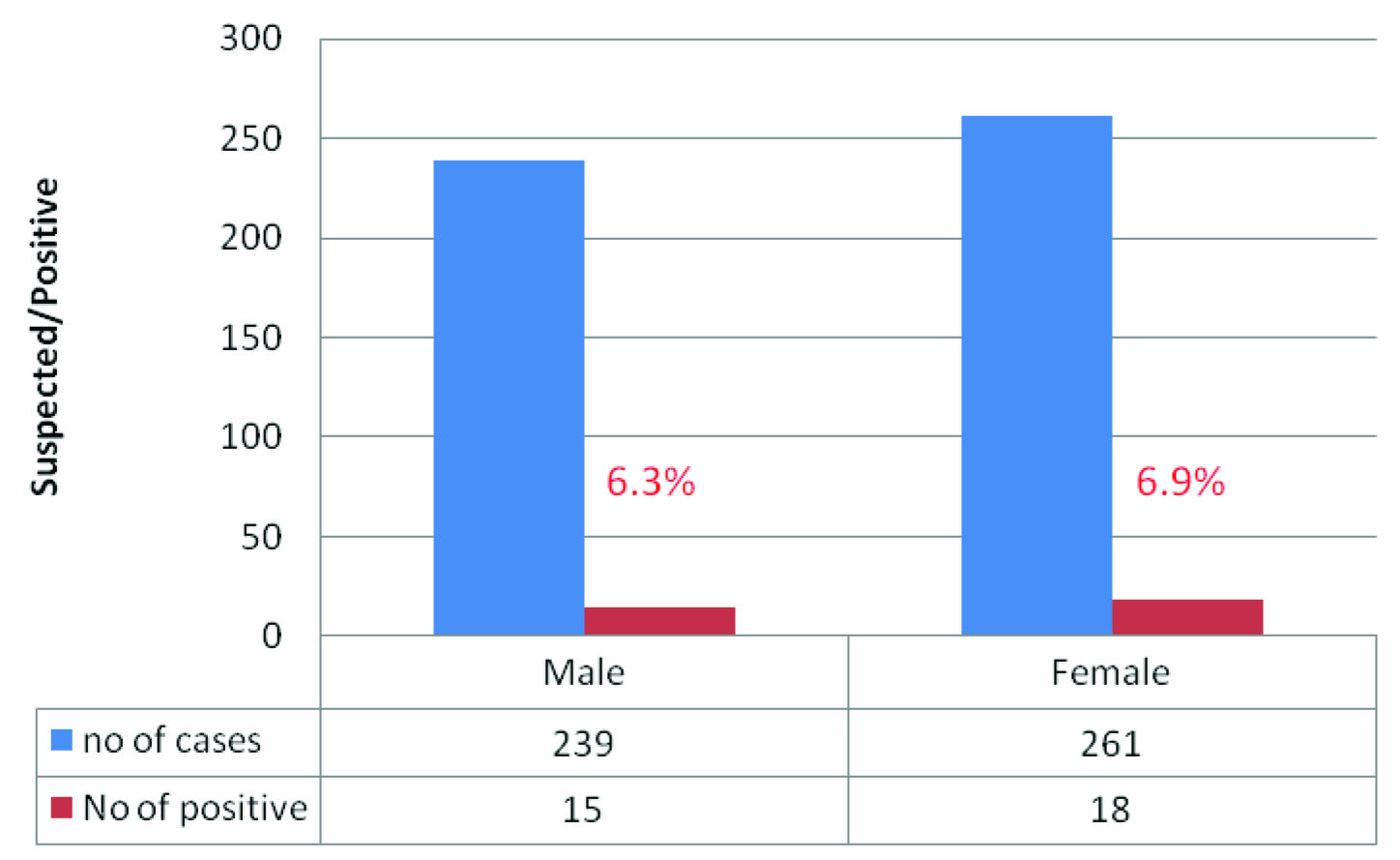
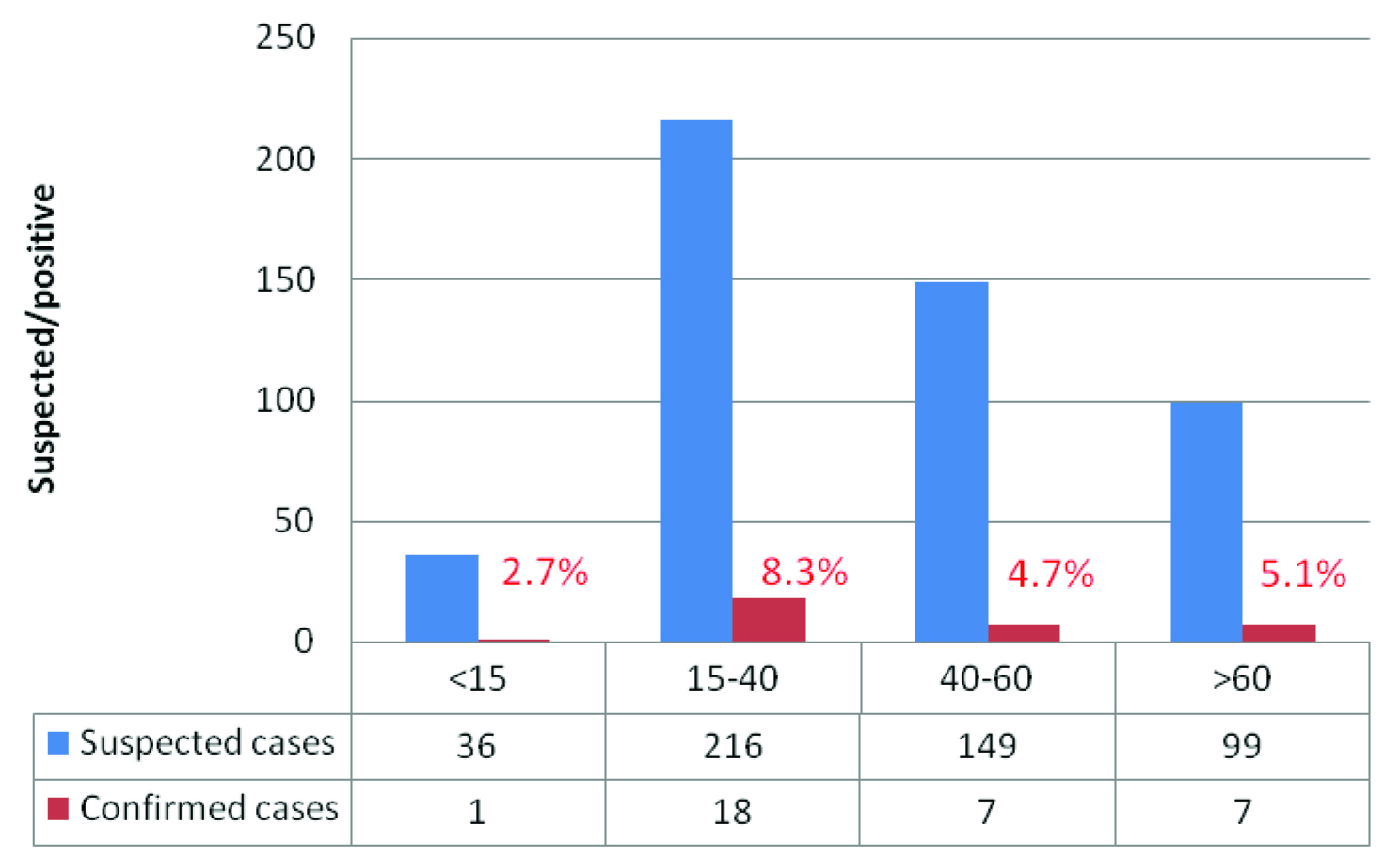
Cut-off was calculated by sum of mean negative control to 0.300. The samples of absorbance less than cut-off was considered as negative and samples of absorbance more than cut-off was considered as positive. Out of 500 samples tested, 33 samples were found positive for Chikungunya IgM antibodies. The disease was more prevalent in 2013 (8.5%), followed by 2012 (7.5%) [Table/Fig-1]. Females (6.9%) were more affected compared to males [Table/Fig-2]. More number of cases belonged to age group of 15 to 40 (8.3%) [Table/Fig-3].
Distribution of Chikungunya suspected and confirmed cases year wise
Distribution of clinically suspected and confirmed cases according to gender
Distribution of clinically suspected and confirmed cases according to age
Discussion
Chikungunya has emerged as a major public health problem in many tropical countries of Africa and Asia. In 2005- 2006 an explosive outbreak of Chikungunya occurred in India affecting more than 1.4 million people in 13 states especially in southern India [11]. Kerala and Karnataka were the worst affected states during 2006 CHIKV outbreak, 27 districts of the Karnataka state reported over 54.74% of the total suspected cases. Several districts of the state such as Bijapur, Gulbarga, Tumkur, Bidar, Raichur, Dharwad, Bellary, Chitradurga, Davangere and Kolar have recorded large number of Chikungunya fever cases (Bijapur district over 80,00 cases) [6,12,13]. Chikungunya fever presents with similar symptoms to other arboviral diseases. Proper aetiological identification (serological diagnostic tests) is necessary for the better clinical management of disease.
Narayan Shrihari et al., conducted a study on prevalence of Chikungunya arboviral infection in and around Bellary district, Karnataka from 2009-2011. Sero positivity rate of Chikungunya was 24.75%. The number of positive cases were more in 2010 (28.04%), than 2009 (23.07%) and subsequently decreased in 2011 (19.05%). Male to female ratio was 0.98 [14].
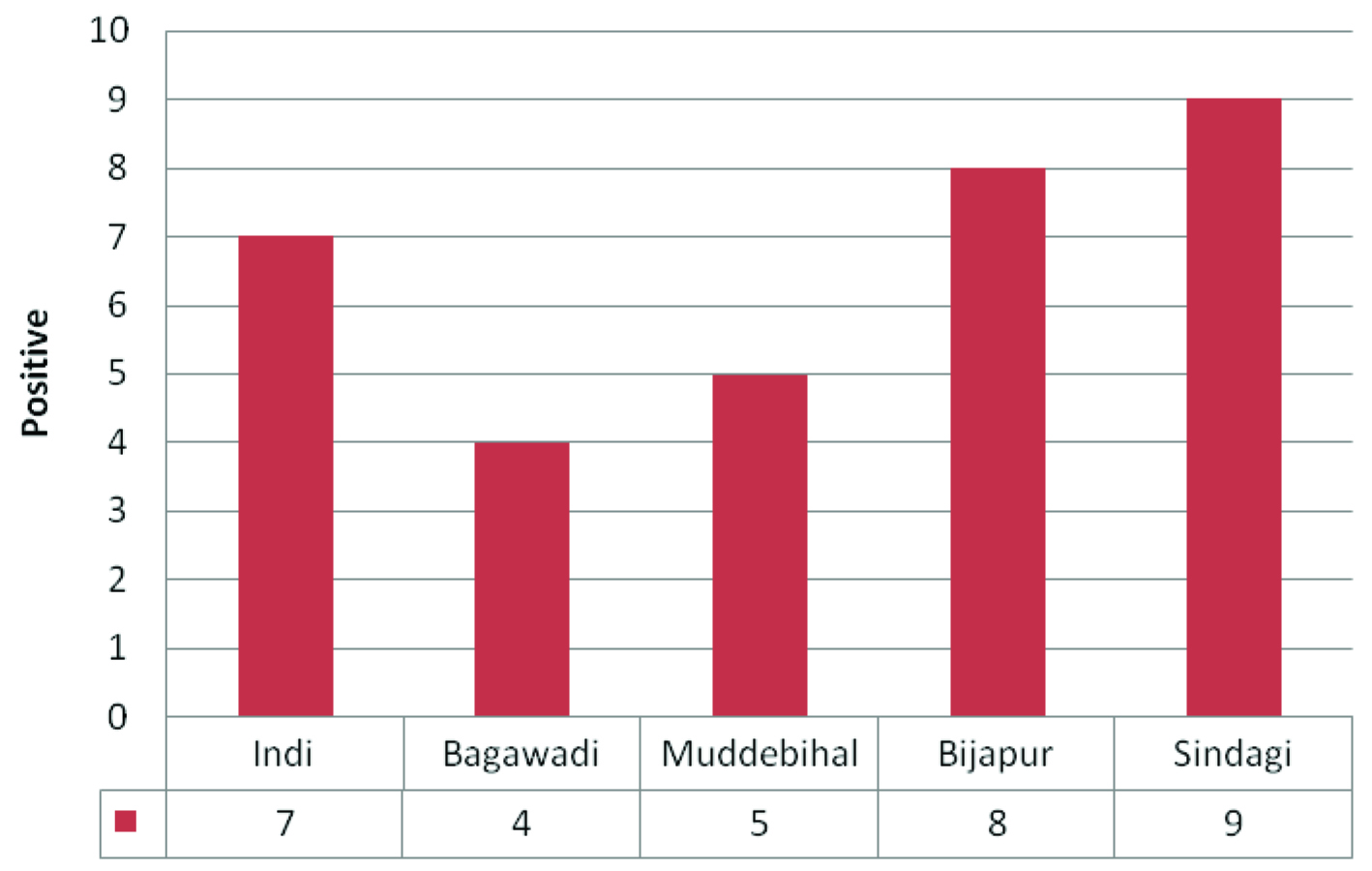
Present study was conducted in Bijapur, which is 250km distant from Bellary. This study included cases with strong suspicion of CHIVA infection. Inclusion criteria were cases with fever and arthralgia. In this study we have noticed the prevalence of Chikungunya was 6.6% in and around regions of Bijapur. More number of cases affected were in 2013 (8.5%) in decreasing order 2012 (7.5%), 2011 (4.6%) and 2014 (4.0%) [Table/Fig-1]. Females (6.9%) were more affected compared to males (6.2%) [Table/Fig-2]. The majority of cases affected were in age group of 15 to 40 (8.3%) [Table/Fig-3]. Bijapur has six taluks, more number of confirmed cases were found in Sindagi, in the decreasing order from taluks Bijapur, Indi, Muddebihal and Bagewadi [Table/Fig-4].
Chikungunya confirmed cases taluk* wise *Taluk is an administrative division in India
Conclusion
Bijapur (Northern part of Karnataka) is endemic to Chikungunya, it is necessary to diagnose the disease for the treatment and management. The prevalence rate of Chikungunya in and around regions of Bijapur was 6.6%. IgM antibody detection by ELISA is a very important tool in diagnosis of infection.
[1]. Text book of Medical Microbiology - Topley & Wilson’s Microbiology and microbial infections by Brian W J Mahy & Leslie collier ninth edition volume 1 [Google Scholar]
[2]. Text book of Medical Microbiology jawetz, Melnick & Adelbergs 24th edition [Google Scholar]
[3]. Staples JE, Breiman RF, Powers AM, Chikungunya fever: an epidemiological review of a re-emerging infectious disease. Review articleClinical Infectious Disease 2009 49(6):942-48. [Google Scholar]
[4]. Padbidri VS, Wairagkar NS, Joshi GD, Umarani UB, a serological survey of arboviral diseases among the human population of the Andaman and Nicobar islands, IndiaSoutheast Asian Journal of Tropical Medicine and Public Health 2002 33(4):749-800. [Google Scholar]
[5]. Kumar CVM Naresh, Johnson AM Anthony, Gopal DVR Sai, Molecular characterization of chikungunya virus from Andhra Pradesh, India & phylogenetic relationship with Central African isolatesIndian J Med Res 2007 126:534-40. [Google Scholar]
[6]. Manimunda SP, Sugunan AP, Rai SK, Vijayachari P, Shriram AN, Outbreak of chikungunya fever, Dakshina Kannada District, South India, 2008Am J Trop Med Hyg 2010 83(4):751-54. [Google Scholar]
[7]. Philippe Renault, Jean-Louis Solet, Daouda Sissoko, A Major Epidemic of Chikungunya Virus Infection on Réunion Island, FranceAm J Trop Med Hyg 2007 77(4):727-31. [Google Scholar]
[8]. Johansson MA, Powers AM, Pesik N, Cohen NJ, Staples JE, Now casting the Spread of Chikungunya Virus in the AmericasPLoS ONE 2014 9(8):e104915 [Google Scholar]
[9]. Pialoux G, Alex B, Stéphane G, Chikungunya, an epidemic arbovirosis- Review articleLancet Infect Dis 2007 7:319-27. [Google Scholar]
[10]. Suryawanshi SD, Dube AH, Khadse RK, Jalgaonkar SV, Sathe PS, Clinical profile of chikungunya fever in patients in a tertiary care centre in Maharashtra, IndiaIndian J Med Res 2009 129:438-41. [Google Scholar]
[11]. Sudeep AB, Parashar D, Chikungunya: an overviewJournal of Bioscience 2008 33(4):443-49. [Google Scholar]
[12]. Talawar AS, Pujar HS, An outbreak of chikungunya epidemic in south india- KarnatakaIJRRAS 2010 5(3):229-34. [Google Scholar]
[13]. Kannan M, Rajendran R, Sunish IP, Balasubramaniam R, A study on chikungunya outbreak during 2007 in Kerala, south IndiaIndian J Med Res 2009 129:311-15. [Google Scholar]
[14]. Narayan S, Kumudini TS, Mariraj J, Krishna S, The prevalence of chikungunya arboviral infection in and around bellary district, karnatakaJournal of evolution of Dental and Medical sciences 2012 1(5):677-81. [Google Scholar]